Performance of the 2021 Estimated Glomerular Filtration Rate CKD-EPI Refit and the European Kidney Function Consortium (EKFC) Formulas
Evelyn O. Ilori, Casey R. Cai, Fatou Sahor, Brianna Wilson, Tanooha Veeramachaneni, Samir M. Parikh, Ibrahim A. Hashim

TL;DR
This study compares kidney function estimation formulas in Black and White populations in the U.S., finding that both new formulas underestimate kidney function at lower levels.
Contribution
The study validates the EKFC and REFIT formulas in U.S. populations, highlighting racial differences in GFR estimation accuracy.
Findings
REFIT equation underestimates measured GFR in Black individuals at eGFR < 80 and in White individuals at eGFR > 20.
EKFC underestimates measured GFR at eGFR > 20 in both Black and White individuals.
REFIT had the least absolute median bias compared to EKFC and CKD-EPI in both racial groups.
Abstract
Background: The glomerular filtration rate (GFR) is a universal clinical measure central to assessing kidney function and to the management of kidney disorders. Several formulas for the estimation of GFR are in use. The European Kidney Function Consortium (EKFC) formula has been reported to more accurately estimate the GFR as compared to the Chronic Kidney Disease Epidemiology Collaboration (CKD-EPI) formula and its recent version (REFIT equation) in European and African populations. However, validation of the EKFC equation in diverse U.S. populations, especially the Black subpopulation, is needed. Methods: Data from the electronic medical records of 75,442 individuals presenting to a large safety net county hospital with measurements of serum creatinine and/or iohexol clearance studies were used to calculate the estimated GFR (eGFR) and to determine CKD stage using the various reported…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
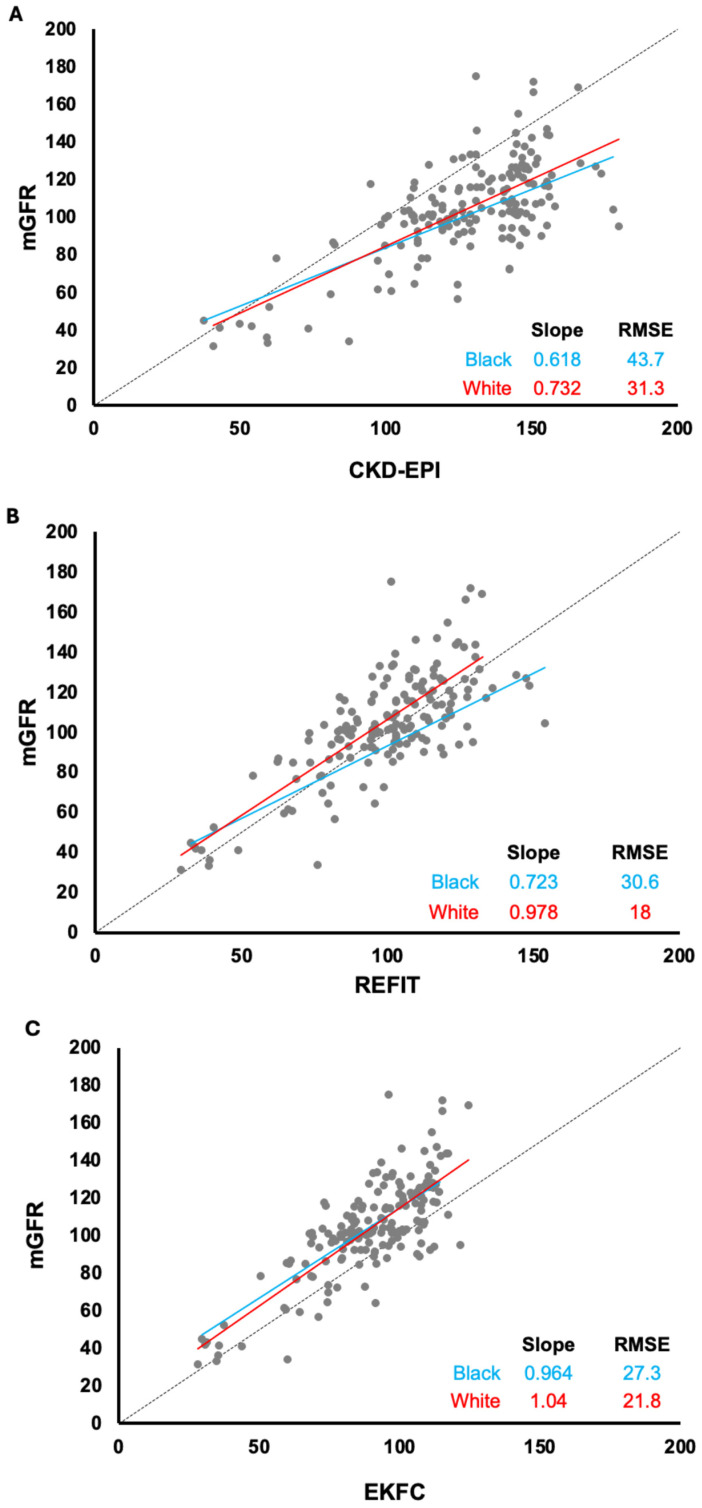 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsChronic Kidney Disease and Diabetes · Dialysis and Renal Disease Management · Renal and Vascular Pathologies
1. Introduction
Chronic kidney disease (CKD) affects over 800 million individuals worldwide, posing a major public health burden due to its significant contribution to morbidity and mortality [1]. Comorbidities such as hypertension, cardiovascular disease, and diabetes can further impair renal function, leading to a decline in the glomerular filtration rate (GFR) [2]. The GFR is the primary clinical measure of kidney function and is essential for diagnosing CKD, staging its severity, and guiding clinical decision-making and management [3]. While measured GFR (mGFR) using exogenous markers such as iothalamate or iohexol clearance remains the gold standard, its routine use is limited by cost, complexity, and availability [4]. Similarly, endogenous creatinine clearance, which relies on timed urine collections (often for 24 h), is inconvenient and prone to inaccuracies due to incomplete urine collection, variability in muscle mass, protein metabolism, technical interference in creatinine measurements, and renal tubular handling of creatinine [5]. Consequently, estimated GFR (eGFR) equations based on serum creatinine (Cr) remain easier to use and indispensable for the clinical assessment of kidney function.
The Chronic Kidney Disease Epidemiology Collaboration (CKD-EPI) equation, developed in the 2000s, has become the most widely used eGFR formula due to its improved accuracy compared to the earlier Modification of Diet in Renal Disease (MDRD) formula [6]. However, the CKD-EPI has limitations, particularly its adoption of patient race as a variable, which is widely recognized as a social construct rather than a biologic determinant of kidney function [7,8]. Furthermore, racial disparities in the early recognition of kidney disease and outcomes have been well documented, with Black and Hispanic populations presenting late and with more severe glomerular disease compared to White populations [9]. The CKD-EPI Refit (REFIT) equation was developed in 2021 to reduce bias by eliminating the race coefficient [8].
In parallel, the European Kidney Function Consortium developed an alternative formula (EKFC) that incorporates age and sex and utilizes a population-dependent normalization coefficient (Q) for improved precision [10]. The EKFC equation has been validated across a broad adult age range among Europeans and Africans, including a few studies among Asians [10,11,12,13,14]. Although it is widely used, however, there have been few studies examining the impact of the EKFC equation in Americans, especially the Black American population that is at significant risk of advanced CKD [15,16]. This study compares the performance of commonly used eGFR equations with regards to accuracy and clinical impact on patients at a large, tertiary academic medical center also serving as a safety net county hospital.
2. Materials & Methods
This observational study was approved by the University of Texas Southwestern Institutional Review Board and the Parkland Hospital Research Office (IRB STU-2021-1030).
2.1. Patient Population
Clinical laboratory results and demographics (self-declared race and gender) data were obtained from the electronic health record system (Epic^®^, Epic Systems, Verona, WI, USA) of patients ≥ 18 years old presenting to a large safety net county hospital with clinically ordered serum creatinine and/or GFR estimation via iohexol measurement from August 2019 to November 2020.
Of the 78,472 patients eligible, 75,442 Black and White individuals were included in this study. Other racial groups aside from White and Black were excluded from this study due to relatively small numbers. Female patients represented 66.8% of Black individuals and 70.3% of the White study population.
2.2. Estimated GFR Determination (eGFR)
Serum creatinine (Cr) was measured enzymatically (via creatinine kinase and sarcosine oxidase) using COBAS^®^ automated instrument (Roche Diagnostics, Indianapolis, IN, USA). The assay is standardized and traceable to the isotope-dilution mass spectrometry. eGFR was calculated using the following equations.
CKD-EPI:
where (k) was 0.7 for women and 0.9 for men, (a) being −0.329 for women and −0.411 for men [3].
REFIT:
where (A) was 0.7 for women and 0.9 for men, and (B) was −0.241 for women and −0.302 for men [16].
EKFC [17]:
(Q) values were 1.0 mg/dL (Black male), 0.93 mg/dL (White male), and 0.73 mg/dL (Black and White female). Creatinine was expressed as mg/dL.
2.3. Measured GFR (mGFR)
GFR was measured in 171 of the study participants as part of their routine medical care (e.g., assessment as candidate donors for renal transplant). Iohexol was administered intravenously and its clearance determined as previously described using an in-house liquid chromatography–mass spectroscopy method. The assay’s analytical measurement ranged from 5 to 1000 mg/mL with imprecision < 10%. The two-compartment model was used to calculate the GFR [18].
2.4. Kidney Disease Staging
CKD stages were assigned using the Kidney Disease Improving Global Outcomes (KDIGO) guidelines (2012) [19]. The CKD stage was determined using the eGFR calculated using the CKD-EPI, REFIT, and EKFC equations and compared.
2.5. Statistical Analyses
The 2-sided Pearson’s Chi square analysis was used to assess the significance of CKD reclassification based on the respective eGFR equations. The mean comparative difference (bias) is calculated by subtracting the eGFR from the mGFR, along with the 95% confidence interval (95%CI). The P30 accuracy was also calculated with 95%CI. The KDIGO reports P30 > 75% as adequate for an eGFR equation to be considered good for clinical decision [15]. All other p values were calculated using the paired t test. All statistical analyses were performed using the Version 25.0.2 NCSS 2025 Statistical Software (NCSS, LLC. Kaysville, UT, USA, https://www.ncss.com/software/ncss/, accessed on 15 April 2025).
3. Results
The demographic and laboratory data for 75,442 individuals, comprising 25,003 Black individuals and 50,439 White individuals, included in the study are summarized in Table 1. The median ages for Black (54 years) and White (49 years) patients are statistically different (p < 0.0001). Females represented 66.8% of the Black and 70.3% of the White study participants. The median serum creatinine level is significantly higher in Black participants, with the eGFR values calculated using the CKD-EPI, REFIT, and EKFC equations being lower, as expected, in the Black population (p < 0.0001) (Table 1). The EKFC formula resulted in the lowest eGFR values for both Black and White individuals, followed by the REFIT formula.
3.1. Reclassification of CKD Stages (As Defined by KDIGO) [15]
The clinical impact of applying the different eGFR equations was evaluated by comparing the obtained CKD stage with the respective eGFR formula (Table 2A). Among Black participants, the REFIT equation reclassified about 80.3% of patients to a higher CKD stage compared to when using the CKD-EPI equation (Table 2A). However, applying the EKFC equation resulted in the reclassification of only 6.5% of Black patients to a higher stage and 8.3% to a lower stage when compared to the REFIT equation (Table 2B).
However, among White participants, using the REFIT equation reclassified 61.0% on average to a higher CKD stage compared to using CKD-EPI (Table 3A), whereas, when applying the EKFC formula, about 7.5% were reclassified to a higher CKD stage and only about 2.6% reclassified to a lower stage (Table 3B). The transitions were all statistically significant (p < 0.005).
3.2. Accuracy of eGFR as Compared to Measured GFR
Measured GFR (mGFR) by iohexol was compared with estimated (eGFR) using the CKD-EPI, REFIT, and EKFC formulas for Black and White participants (Figure 1).
Among Black individuals, all three eGFR formulas underestimated GFR when compared to mGFR at eGFR < 60 mL/min per 1.73 m^2^. However, the CKD-EPI formula overestimated the GFR compared to the measured GFR (mGFR) among Black participants for eGFR > 60 mL/min per 1.73 m^2^ and among White participants for eGFR > 40 mL/min per 1.73 m^2^ (Figure 1A).
The REFIT equation underestimated the GFR compared to the mGFR among Black participants when eGFR < 80 mL/min per 1.73 m^2^ and overestimated the GFR compared to the mGFR when eGFR > 80 mL/min per 1.73 m^2^ (Figure 1B). Among the White population, the REFIT equation underestimated the GFR compared to the mGFR, irrespective of the eGFR values. Furthermore, the EKFC formula underestimated the GFR compared to the mGFR among both White and Black populations when eGFR > 20 mL/min per 1.73 m^2^ (Figure 1C).
Among the Black population, the line slope is similar for the CKD-EPI and REFIT equations, while the line slope is similar for the REFIT and EKFC equations among the White population.
The median bias between mGFR and eGFR was determined for all three equations in both racial populations (Table 4). Median GFR bias was significantly different between mGFR and eGFR as obtained by the different formulas—CKD-EPI and REFIT, and EKFC and REFIT—for both the Black and White groups (p < 0.0001 for all comparisons). Although the absolute median bias is >5 for all three eGFR equations for both subgroups, the REFIT equation results in the least absolute median bias.
When compared to CKD-EPI, the REFIT equation had a significantly higher P30 among both the Black and White populations (p = 0.0055 and p < 0.0001, respectively). However, although higher than that for the EKFC, the P30 for the REFIT equation is not statistically significant in either the Black (p = 0.16) or White (p = 0.37) subgroups.
4. Discussion
More than one in seven adults in the United States is affected by chronic kidney disease, which makes accurate estimation of the glomerular filtration rate critical for diagnosis and management, particularly in populations where disparities in CKD prevalence and outcomes persist [20]. This study evaluated the performance of three widely used creatinine-based eGFR equations—CKD-EPI, REFIT, and EKFC—in a large cohort of Black and White individuals. Notably, our institution is a safety net county hospital that serves a unique population of patients with a high burden of chronic diseases and morbidity. Our findings provide important insights into the strengths and limitations of these equations and contribute to the ongoing debate on the best approach to GFR estimation.
4.1. Performance of the EKFC Equation in Our Cohort
The EKFC equation was developed to improve accuracy across diverse populations by incorporating age, sex, and serum creatinine that is normalized using a Q value [10]. While earlier studies have reported the improved accuracy of the EKFC equation in Black and non-Black populations in Europe, Africa, and Asia, limited validation studies have been conducted in the United States, particularly among U.S.-based Black populations [15].
In our cohort, the EKFC equation consistently underestimated the mGFR in both Black and White individuals. Although the REFIT equation yielded the smallest median bias in both racial subgroups, it also underestimated the mGFR in Black participants at eGFR < 80 mL/min per 1.73 m^2^. Underestimation of the glomerular filtration rate could result in a significant increase in nephrology referrals, overtreatment, patient harm, and medical waste. A recent evaluation of the EKFC equation in over 12,000 adults from multiple U.S. cohorts reported less median bias for both the race-free and population-specific versions of the EKFC equation as compared to the REFIT, with similar P30 across equations [15]. Our study shows that institutions in the United States with unique patient populations should evaluate the effectiveness of the EKFC equation before adoption.
The clinical impact of transitioning to the EKFC equation from the REFIT equation is highlighted by the reclassification of CKD stages for both Black and White participants. For example, a mean of 6.5% of Black participants were reclassified to a higher CKD stage and 8.3% reclassified to a lower stage. For White participants, 7.5% were reclassified to a higher CKD stage, and 2.6% were reclassified to a lower stage. These shifts in CKD staging may have significant clinical implications, as they can influence decisions regarding medication dosing, nephrology referral, and eligibility for kidney transplantation for individual patients. Our study highlights the importance of selecting an eGFR equation that aligns with the clinical context and is appropriate for the patient population being served.
4.2. Comparison of the REFIT and CKD-EPI Equations
Our study demonstrates that the REFIT equation, which does not include a race correction factor, results in significantly more accurate eGFR compared to the race-based CKD-EPI formula in both Black and White populations. Black individuals are disproportionately affected by CKD and experience worse outcomes compared to White individuals, including in pediatric populations [21]. Eliminating the race factor from the eGFR equation may facilitate earlier identification of renal impairment in Black patients, enabling timely intervention and potentially preventing further kidney dysfunction. The clinical impact of transitioning from the CKD-EPI to the REFIT equation is highlighted by the reclassification of an average of 80.3% and 61.0% of Black and White participants, respectively, to a higher CKD stage. The median bias and P30 are also significantly improved using the REFIT as compared to the CKD-EPI equation. An epidemiological study using the NHANES database and examining the potential effects of switching to the REFIT equation from the CKD-EPI equation showed an 11% increase in the number of chronic kidney disease diagnoses among Black adults and a 20% decrease among non-Black adults [6]. Interestingly, the trend affects kidney transplant eligibility at CKD stage 3b and higher, with a 9% increase among Black adults as compared to an 8% decrease among non-Black adults. This study underscores the value of removing race as a component of the eGFR calculation, promoting the transition from the CKD-EPI to the REFIT equation. This study also highlights the discrepancy in CKD classification among the populations studied. Adoption of the REFIT formula will aid in the earlier identification of patients with CKD and, thus, the institution of therapy. Future studies will examine outcomes with respect to the adoption of the revised formula.
4.3. Discourse on the Accuracy of Creatinine-Based Equations
This study aligns with prior studies suggesting that creatinine-based equations demonstrate imprecision, particularly due to factors that influence serum creatinine levels, and advocating the use of multiple filtration markers such as creatinine and cystatin C instead of solely creatinine in calculating eGFR to lessen the impact of muscle mass in eGFR calculations [16]. While cystatin-based equations have shown promise in improving accuracy and reducing racial bias, creatinine remains widely used due to its accessibility and cost-effectiveness. A recent study of >4000 adults indicated that both REFIT and EKFC are effective depending on the population being evaluated [22].
4.4. Strengths and Limitations
This study has several strengths, including its large sample size, especially the large population of Black individuals, served by our county hospital. Our findings provide valuable insights into the clinical impact of three widely used eGFR equations in a population with advanced and complex medical conditions. Notably, we showed that the EKFC equation underestimates the mGFR while the REFIT tends to underestimate the mGFR at eGFR < 80 mL/min per 1.73 m^2^ in the Black population. This could potentially result in the overdiagnosis of CKD in this subgroup. These findings underscore the importance of careful clinical interpretation of eGFR values. However, our study also has limitations. First, the retrospective design may introduce selection bias, as participants with available iohexol measurements may differ from the general population. Secondly, we did not evaluate cystatin C-based equations, which have shown promise in reducing racial bias in GFR estimation [15]. This study was conducted at a single institution, which also impacted the number of patients with urinary iohexol clearance data. Although iohexol is considered one of the gold standards for mGFR, studies have reported imprecision, which may result in increased bias [23].
5. Conclusions and Future Directions
In conclusion, our study provides novel insights into the performance of the EKFC, REFIT, and CKD-EPI equations in a patient population at a county hospital with a high proportion of Black patients. Both the EKFC and REFIT equations demonstrated superiority to the CKD-EPI equation, with the REFIT showing the least bias and highest accuracy in both Black and White participants. Screening and diagnostic tools based on inherent biology are needed to overcome the imprecision of race-based medicine and address health disparities in minority populations. Future studies should continue to explore eGFR equations that incorporate biomarkers aside from creatinine, such as cystatin C. Also, longitudinal studies are needed to assess the clinical impact of eGFR reclassification on patient outcomes, especially with the adoption of the EKFC equation in U.S. populations.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Kovesdy C.P. Epidemiology of chronic kidney disease: An update 2022 Kidney Int. Suppl.20221271110.1016/j.kisu.2021.11.00335529086 PMC 9073222 · doi ↗ · pubmed ↗
- 2Fraser S.D. Roderick P.J. May C.R. Mc Intyre N. Mc Intyre C. Fluck R.J. Shardlow A. Taal M.W. The burden of comorbidity in people with chronic kidney disease stage 3: A cohort study BMC Nephrol.201516193 Erratum in BMC Nephrol. 2020, 21, 54310.1186/s 12882-020-02205-w 26620131 PMC 4666158 · doi ↗ · pubmed ↗
- 3Musso C.G. Alvarez-Gregori J. Jauregui J. Macias-Nunez J.F. Glomerular filtration rate equations: A comprehensive review Int. Urol. Nephrol.2016481105111010.1007/s 11255-016-1276-127052619 · doi ↗ · pubmed ↗
- 4Delanaye P. Ebert N. Melsom T. Gaspari F. Mariat C. Cavalier E. Björk J. Christensson A. Nyman U. Porrini E. Iohexol plasma clearance for measuring glomerular filtration rate in clinical practice and research: A review. Part 1: How to measure glomerular filtration rate with iohexol?Clin. Kidney J.2016968269910.1093/ckj/sfw 07027679715 PMC 5036902 · doi ↗ · pubmed ↗
- 5Hsu C.Y. Bansal N. Measured GFR as “gold standard”—All that glitters is not gold?Clin. J. Am. Soc. Nephrol.201161813181410.2215/CJN.0604061121784836 · doi ↗ · pubmed ↗
- 6Diao J.A. Wu G.J. Wang J.K. Kohane I.S. Taylor H.A. Tighiouart H. Levey A.S. Inker L.A. Powe N.R. Manrai A.K. National Projections for Clinical Implications of Race-Free Creatinine-Based GFR Estimating Equations J. Am. Soc. Nephrol.20233430932110.1681/ASN.202207081836368777 PMC 10103103 · doi ↗ · pubmed ↗
- 7Ahmed S. Nutt C.T. Eneanya N.D. Reese P.P. Sivashanker K. Morse M. Sequist T. Mendu M.L. Examining the Potential Impact of Race Multiplier Utilization in Estimated Glomerular Filtration Rate Calculation on African-American Care Outcomes J. Gen. Intern. Med.20213646447110.1007/s 11606-020-06280-533063202 PMC 7878608 · doi ↗ · pubmed ↗
- 8Delgado C. Baweja M. Crews D.C. Eneanya N.D. Gadegbeku C.A. Inker L.A. Mendu M.L. Miller W.G. Moxey-Mims M.M. Roberts G.V. A Unifying Approach for GFR Estimation: Recommendations of the NKF-ASN Task Force on Reassessing the Inclusion of Race in Diagnosing Kidney Disease Am. J. Kidney Dis.202279268288.e 26110.1053/j.ajkd.2021.08.00334563581 · doi ↗ · pubmed ↗