The Mesothelioma Systemic Inflammation Score Is Independently Associated with Overall Survival and Predicts Benefit of Multimodality Treatment in Pleural Mesothelioma
Berta Mosleh, Katharina Sinn, Anna Cho, Anton Reiner, Ariane Steindl, Christian Lang, Sabine Zöchbauer-Müller, Karin Dieckmann, Joachim Widder, Helmut Prosch, Balazs Dome, Karin Schelch, Clemens Aigner, Thomas Klikovits, Michal Benej, Stefan Watzka, Martin Filipits

TL;DR
A new inflammation-based score helps predict survival and treatment benefits in pleural mesothelioma patients.
Contribution
The Mesothelioma Systemic Inflammation Score (MSIS) is introduced as a novel prognostic and predictive tool for treatment outcomes.
Findings
MSIS independently predicts overall survival in pleural mesothelioma patients.
Multimodality treatment benefits are limited to patients with low MSIS.
MSIS accurately stratifies patient survival outcomes across two independent cohorts.
Abstract
Few malignancies generate as many controversies about clinical management as pleural mesothelioma. The merits of multimodality treatment protocols have been continuously discussed, often with limited evidence from prospective trials. Given that the first randomized prospective studies investigating the role of surgery in mesothelioma produced debatable results, it may be too soon to retire the concept of multimodality treatment protocols including surgery for selected candidates. Accurate prognostication could improve treatment allocation, offering multimodality therapy pathways or sparing patients from aggressive and potentially morbid treatment strategies. The aim of our study was to validate the prognostic and predictive power of a novel inflammation-based score—the Mesothelioma Systemic Inflammation Score (MSIS)—in a large cohort of pleural mesothelioma patients treated in a…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
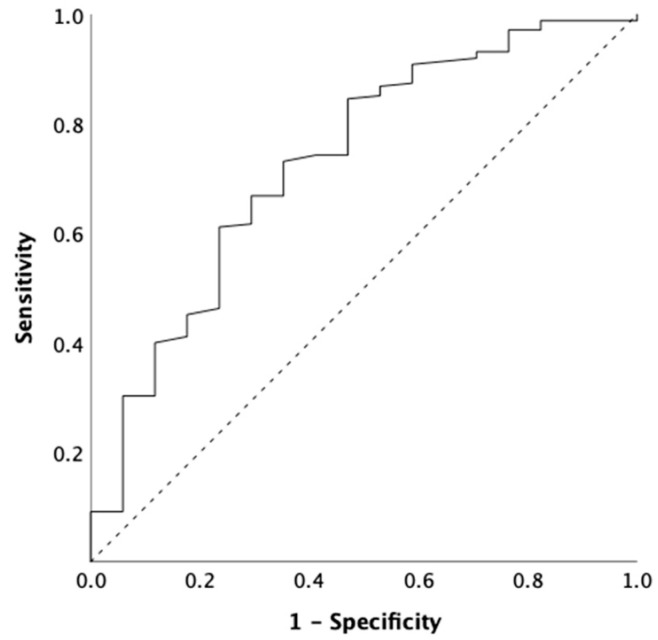 Figure 1
Figure 1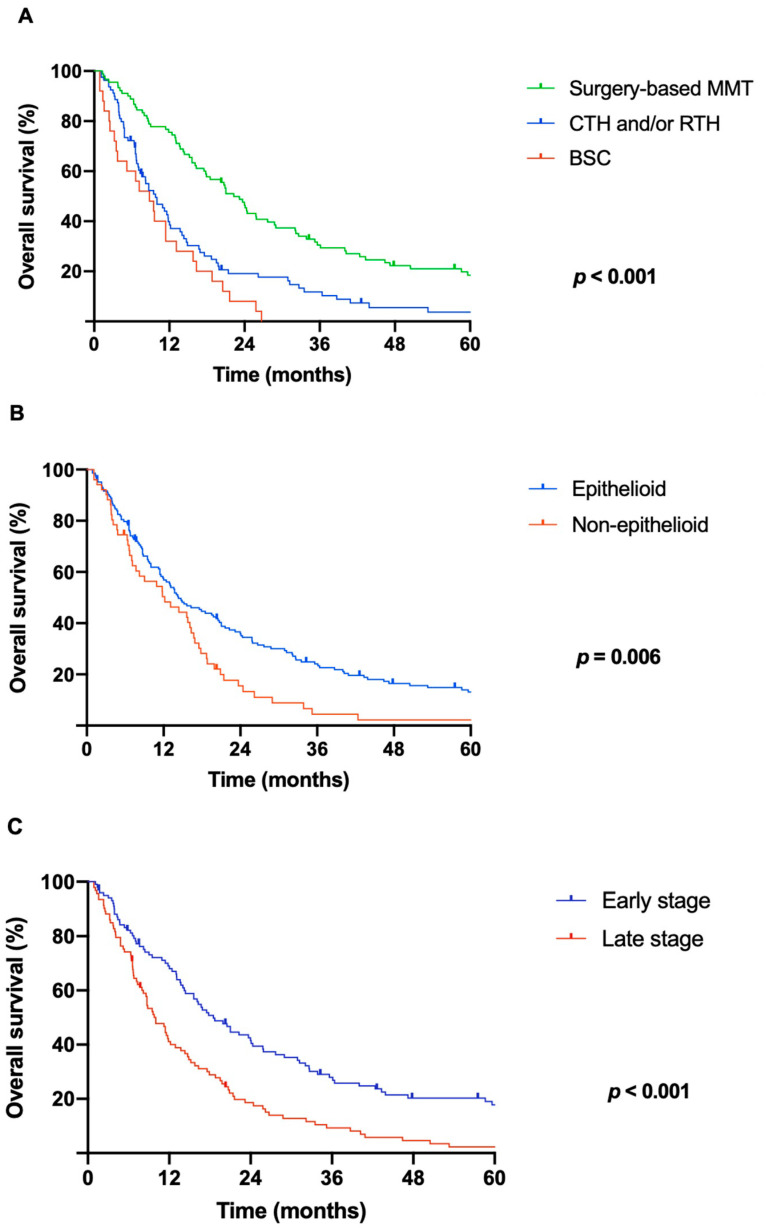 Figure 2
Figure 2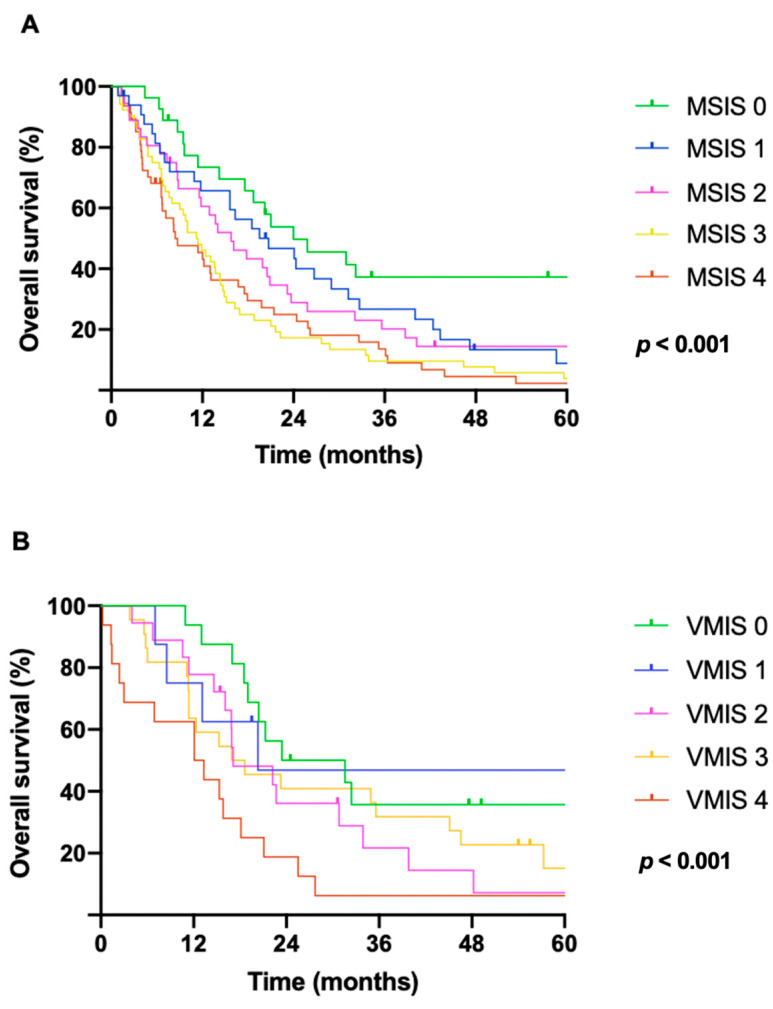 Figure 3
Figure 3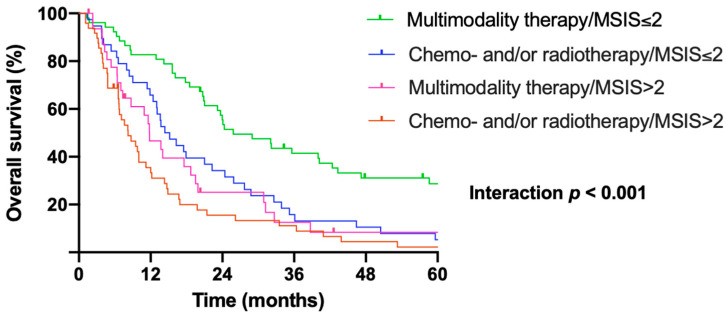 Figure 4
Figure 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsOccupational and environmental lung diseases · Pleural and Pulmonary Diseases · Inflammatory Biomarkers in Disease Prognosis
1. Introduction
Malignant pleural mesothelioma (MPM) is a highly aggressive, often asbestos-induced malignancy with dismal outcomes. The incidence may still rise in some countries, reflecting the global trend of commercial asbestos use [1,2]. The prognosis is poor, with a median overall survival time (OS) ranging from 10 to 22 months depending on the stage, histology, sex, and type of treatment [3,4]. Identifying clinically useful biomarkers and prognostic scores for this disease is imperative to facilitate early diagnosis and guide treatment allocation. Prognostic factors such as age, sex, histologic subtype, tumor stage, performance status, and several routine laboratory parameters have been validated in different population studies [5,6,7,8,9]. Also, systemic inflammatory response has been shown to have a pivotal role in cancer outcome. In consequence, inflammatory scores have been proposed to indicate prognosis [5,6,7,10,11,12,13]. Prognostic scoring systems such as the European Organization for Research and Treatment of Cancer (EORTC) and the Cancer and Leukemia Group B (CALGB) have been designed to assess clinical outcomes in cancer patients. Prognostic factors for pleural mesothelioma included in these models are performance status, age, sex, histologic subtype, symptoms, and blood parameters, particularly LDH, platelet, and white blood cell counts. The practical use of these scoring systems is limited in daily clinical management [14,15]. Furthermore, the literature lacks large-scale studies evaluating the prognostic value of systemic inflammation scores in MPM. A lack of homogeneity in the optimal cut-off values also exists.
Inflammation scores, namely the neutrophil-to-lymphocyte ratio (NLR), the platelet-to-lymphocyte ratio (PLR), the lymphocyte-to-monocyte ratio (LMR), and the modified Glasgow prognostic score (mGPS), as well as inflammatory biomarkers including C-reactive protein (CRP), fibrinogen, and albumin, have been investigated as independent prognostic factors [16,17,18,19,20,21,22,23,24,25,26]. In particular, NLR, PLR, and LMR have been studied for their prognostic significance in MPM [17,27,28]. In different malignancies, including lung cancer, prostate cancer, renal cell carcinoma, esophageal and gastric cancer, inflammation-based scores have been suggested as predictive factors of patients´ outcomes [29,30,31,32,33,34,35,36,37,38]. Consequently, establishing rational and easily available prognostic systems with clinical utility is of growing interest.
The aim of this study was to validate the prognostic and predictive power of our novel inflammation-based score, the Mesothelioma Systemic Inflammation Score (MSIS), in a large retrospective cohort of MPM patients treated in a high-volume institution.
2. Materials and Methods
2.1. Patients and Methods
In this retrospective study, patients with histologically confirmed MPM, diagnosed between 1994 and 2020, at the Department of Thoracic Surgery, Medical University of Vienna, Austria, were included. Clinical data were consecutively collected from hospital databases and medical records including age, sex, histologic subtype, ECOG performance status, disease stage, diagnostic methods, treatment approaches, symptoms, tumor site, and laboratory parameters. All patients were (re)staged according to the eighth edition of the pleural mesothelioma tumor, node, metastasis (TNM) staging system developed by the International Mesothelioma Interest Group (IMIG) and the International Association for the Study of Lung Cancer (IASLC) [4,39,40,41]. For staging purposes, computed tomography (CT) of the chest and abdomen as well as magnetic resonance imaging (MRI) of the brain or cranial CT scans before 2015 and positron emission tomography CT scans (PET-CT) and brain MRIs after 2015 were performed. This study was approved by the Ethics Committee of the Medical University of Vienna (EK 2137/2022, approval date 31 March 2024) according to the Declaration of Helsinki.
All patients were presented at thoracic oncology multidisciplinary tumor boards, including thoracic surgeons, oncologists, radiation oncologists, radiologists, and pulmonologists, to define treatment strategies. Patients were stratified to treatment protocols by a comprehensive assessment of the histologic subtype of the disease, stage, tumor volume, and resectability according to the latest guidelines as well as co-morbidities and performance status. Patients aged between 18 and 75 years.
Treatment strategies included multimodality treatment, chemotherapy and/or palliative radiotherapy, and best supportive care (BSC). Multimodality treatment consisted of neoadjuvant platinum-based chemotherapy combined with pemetrexed, subsequent macroscopic complete resection, and adjuvant hemithoracic radiation therapy. Extrapleural pneumonectomy was systematically performed following a standard technique defined by en bloc resection of the entire lung, visceral and parietal pleura, pericardium and diaphragm, and subsequent reconstruction of the pericardium and diaphragm with prosthetic patches. Patients with an ECOG performance status of 0–1, adequate pulmonary function (predicted postoperative forced expiratory volume in 1s [FEV1] and a diffusing capacity for carbon monoxide [DLCO] > 45%), normal cardiac function (ejection fraction > 55% and no major heart valve disease), no major organ dysfunctions, and no history of other malignancies were eligible for multimodality treatment.
BSC was defined as symptom relief and palliative care without active anticancer treatment, including pleural effusion and ascites management, as well as pain management to improve quality of life.
2.2. Prognostic Scores
For all patients, pretreatment laboratory parameters and prognostic scores were evaluated. Laboratory parameters were measured at the date of diagnostic procedures before surgical biopsies and talc pleurodesis to eliminate their potential impact on the inflammatory response. In accordance with the literature, the optimal cut-off value was defined as 1 mg/dL for CRP, 5 for NLR, 160 for PLR, and 2.6 for LMR [17,25,28,42,43,44,45,46,47]. For fibrinogen, the optimal cut-off value was defined as 537.5 mg/dL by the receiver operating characteristic (ROC) curve analysis (Figure 1). Based on these cut-off values validated by Cox regression analysis in our cohort, we established a novel pretreatment inflammatory scoring system, named the Mesothelioma Systemic Inflammation Score (MSIS), consisting of NLR, PLR, CRP, and fibrinogen. Patients with elevated values received one point for each component, resulting in a scoring system of 0–4 in total (Table 1).
2.3. Validation Cohort
External validation of the Mesothelioma Systemic Inflammation Score was performed in an independent cohort of patients (n = 80) treated at the Department of Thoracic Surgery, Karl Landsteiner Institute for Clinical and Translational Thoracic Surgery Research, Clinic Floridsdorf, Vienna, Austria. Treatment approaches included multimodality treatment (MMT), chemo- and/or radiotherapy (CTH and/or RT), or best supportive care (BSC).
2.4. Statistical Analysis
Categorical data were displayed as counts and percentages and continuous variables as median and interquartile ranges (IQRs). Previously published, widely accepted cut-off values were used when available. In case of a lack of substantial evidence from the literature, the optimal cut-off values were determined by the receiver operating characteristic curve (ROC). Fisher´s exact test was performed to assess the relationship between pretreatment MSIS and clinical characteristics of patients. The Cox proportional hazard regression model was used for univariable and multivariable survival analyses to identify independent factors correlated with overall survival (OS). OS was calculated as the time from the definitive histopathological diagnosis to the date of death or last follow-up. Disease-free survival (DFS) was defined from the time of the end of treatment to the time of pathologically or clinically proven recurrence. Survival analyses were displayed as Kaplan–Meier curves. Differences were considered statistically significant for p-values < 0.05. All statistical analyses were performed using the SPSS 27.0 software system (SPSS Inc., Chicago, IL, USA). Graphics were generated with GraphPad Prism version 8.4.3. (GraphPad Software, Boston, MA, USA).
3. Results
3.1. Patient Characteristics
Details on baseline characteristics are displayed in Table 2. In total, 195 (147 male, 75%) consecutive histologically confirmed MPM patients with sufficient clinical data could be enrolled. The median age was 67 years (IQR 58–74). At the time of diagnosis, 137/195 (70%) patients presented with pleural effusions. Other common symptoms were dyspnea (121/195, 62%) followed by chest pain (76/195, 39%) and cough (36/195, 19%). A reduced ECOG performance status (ECOG PS 1–3) could be observed in 77 patients (40%). 96 patients (49%) were diagnosed with early-stage disease (Stage I–II). The most common diagnostic method was video-assisted thoracoscopy (VATS; 160/195, 82%), followed by the thoracotomy approach (35/195, 18%). The majority of patients presented with an epithelioid subtype (n = 144, 74%).
3.2. Treatment Strategy
All patients were allocated to either multimodality treatment (MMT), chemo- and/or radiotherapy (CTH and/or RT), or best supportive care (BSC). In total, 90 patients (90/195, 46%) received surgery within a multimodality treatment approach. Extrapleural pneumonectomy (EPP) was the most commonly performed procedure (n = 73). Following a shift from lung-sacrificing to lung-sparing surgery, extended pleurectomy/decortication (EPD) and pleurectomy/decortication (P/D) were completed in 12 and 5 patients, respectively. We report six (8.2%) perioperative deaths (within 30 days) following EPP. Lethal adverse events included pulmonary embolism (n = 2, 2.7%), acute respiratory distress syndrome (ARDS; n = 3, 4.1%), and acute heart failure (n = 1, 1.4%). In 80 cases (41%), chemotherapy and/or radiation was proposed; 25 patients (13%) received best supportive care.
3.3. Survival and Prognostic Scores
The median OS was 14 months for the entire cohort (95% CI; 11.4–16.6) with a survival rate of 56% at 1 year, 17% at 3 years, and 10% at 5 years, respectively.
The median OS and DFS of patients undergoing multimodality treatment protocols including macroscopic complete resection were 22.3 months (95% CI; 18.6–26.0) and 15.7 months (95% CI; 12.7–18.7), respectively.
Notably, patients after multimodality therapy including surgery survived significantly longer (p < 0.001, median OS 22.3 months) compared to patients treated with chemo- and/or radiotherapy alone (9.8 months) or those receiving best supportive care (8.8 months; Figure 2A).
Significant overall survival benefit was observed in patients with epithelioid histology compared to patients with non-epithelioid subtypes (14.3 months vs. 12.2 months, p = 0.006; Figure 2B) as well as in early (I–II) tumor stages compared to advanced (III–IV) stages (21 months vs. 9.5 months, p < 0.001; Figure 2C).
Elevated fibrinogen (≥537.5 mg/dL; 10 vs. 20.5 months, p < 0.001), CRP (≥1 mg/dL; 11.9 vs. 20.5 months, p = 0.004), NLR (≥5; 11.4 vs. 16.1 months, p = 0.006), and PLR (≥160; 12.9 vs. 20.2 months: p = 0.009) were significantly associated with poorer prognosis.
Similarly, patients with elevated mGPS had a shorter overall survival (6.7, 12.9, and 20.7 months for mGPS 2, 1, and 0, respectively; p = 0.008).
The estimated median survival did not significantly differ between patient groups with high (≥2.6) and low (<2.6) LMR values (15.6 vs. 13.6 months, p = 0.053).
MSIS was able to stratify patients with significant survival differences. As displayed in Figure 3A, the median OS was significantly decreased with higher scores (24.0 months, 95% CI: 11.4–36.5; 20.7 months, 95% CI: 10.3–31.1; 15.8 months, 95% CI: 10.1–21.4; 11.2 months, 95% CI: 8.1– 14.3; and 8.4 months, 95% CI: 3.2–13.6 for MSIS of 0, 1, 2, 3, and 4, respectively; p < 0.001).
The prognostic power of MSIS to predict survival differences was further validated in an independent cohort (n = 80). The results of the baseline analysis could be verified in the external validation cohort. The median OS in the validation cohort significantly decreased with higher scores (23.4, 20.3, 17.2, 16.9, and 12.1 months for MSIS of 0, 1, 2, 3, and 4, respectively; p < 0.001; Figure 3B).
Furthermore, survival rates for patients with the lowest (0) and highest (4) MSIS were 74% and 46% at 1 year, 37% and 14% at 3 years, and 37% and 2% at 5 years, respectively. Higher pretreatment MSIS was associated with more advanced disease stages (p = 0.001).
Clinical characteristics according to the Mesothelioma Systemic Inflammation Scores are shown in Table 3, whereby significant differences between MSIS groups were found regarding stage (p = 0.001) and the type of treatment (p = 0.047). Detailed OS of patients according to the MSIS in different treatment groups is listed in Table 4.
Potential prognostic factors were investigated by univariable analyses. Hereby, the following parameters were predictors for OS: age (p = 0.019), ECOG performance status (p < 0.001), histologic subtype (p = 0.006), tumor stage (p < 0.001), type of treatment (p < 0.001), mGPS (p = 0,008), NLR (p = 0.006), PLR (p = 0.009), fibrinogen (p < 0.001), CRP (p = 0.004), and MSIS (p < 0.001). As a next step, multivariable analysis was performed, wherein treatment (p = 0.004), stage (p = 0.001), and the MSIS (p < 0.001) were independently associated with OS (Table 5).
3.4. Pretreatment Msis Predicts Benefit of Surgery Within Multimodality Treatment Protocols
To further validate the predictive value of the pretreatment MSIS in MPM, we performed a sub-analysis regarding treatment modalities and MSIS. Thus, patients were divided into four subgroups: (1) patients with low (≤2) MSIS undergoing surgery within multimodality treatment, (2) patients with low (≤2) MSIS undergoing chemo- and/or radiotherapy alone, (3) patients with elevated (>2) MSIS receiving surgery within multimodality treatment, and (4) patients with elevated (>2) MSIS receiving chemo- and/or radiotherapy alone. The pairwise comparison between the four groups revealed that significant survival benefit of aggressive multimodality regimens including surgery was limited to patients with low MSIS. The median survival was significantly different between these four groups, whereby patients with low MSIS receiving multimodality treatment including macroscopic complete resection showed the longest survival, while patients with high MSIS receiving CTH and/or RTH alone showed the shortest survival time (p < 0.001; Figure 4). Accordingly, patients with low MSIS had a significantly longer overall survival after undergoing surgery within multimodality treatment protocols compared to patients after chemo- and/or radiotherapy alone (25.8 months, 95% CI: 16.4–35.3 vs. 14.4 months, 95% CI: 10.4–18.4; p < 0.001). In contrast, the treatment strategies did not significantly influence the overall survival in patients with elevated MSIS (surgery within multimodality protocols: 11.8 months, 95% CI: 8.3–15.3 vs. CHT and/or RTH: 8.2 months, 95% CI: 5.2–11.3; p = 0.233).
4. Discussion
In the present study, we investigated the prognostic and predictive power of a novel inflammation-based system—the Mesothelioma Systemic Inflammation Score, a product of NLR, PLR, CRP, and fibrinogen—in a large cohort of pleural mesothelioma patients treated in a high-volume center. Our results indicate that MSIS is an easily accessible, non-invasive, inexpensive, and reproducible tool in routine clinical management and is strongly associated with outcome prediction in MPM.
Currently, there is a lack of accurate biomarkers and inflammatory scoring systems for diagnosis, patient selection, prognostication, and treatment prediction in mesothelioma [17,47,48].
Prognostication in MPM has been mainly studied in single-center settings and with a limited number of patients. Investigated factors have frequently included age, sex, histologic subtype, tumor stage, tumor site, performance status, and treatment approaches, as well as laboratory parameters and biomarkers such as white blood cell counts, platelet counts, CRP, fibrinogen, albumin, activin A, and combined inflammatory markers of those [9,17,18,19,20,49]. Male sex, non-epithelioid histology, high white blood cell and platelet counts, high CRP, low hemoglobin, chest pain, right-sided disease, and treatment without surgical resection have been validated as poor prognostic indicators across the literature [5,7,50,51,52]. Only a few advances in disease prognostication and prediction were reported in recent research, including the proposal of nuclear grading in epithelioid mesothelioma by the 2021 WHO Classification of Tumors of the Pleura [53]. Pathologic grading and morphological features such as necrosis and mitosis characteristics were proven as independent prognosticators with therapeutic implications for treatment allocation and clinical management [54,55,56].
In various malignancies, inflammation-based markers have been suggested as prognostic indicators of patients´ outcomes as inflammation plays a critical part in cancer progression. Neutrophil, lymphocyte, monocyte, and platelet counts as well as NLR, PLR, LMR, CRP, and the systemic immune-inflammation index (SII) have been verified as key inflammatory factors [57,58,59,60]. The association between NLR and outcome in MPM has been laboriously studied in smaller and larger-scale studies as well as in patient cohorts receiving systemic therapy or macroscopic complete resection [28,61,62,63,64]. The prognostic effect of NLR was further validated in a meta-analysis of a total of 11 studies involving 1533 patients [28]. The significance of high SII (calculated as neutrophil × platelet/lymphocyte counts) has been tested and correlated with unfavorable prognosis in MPM, as well as in non-small-cell lung cancer, esophageal squamous cell carcinoma, gastric cancer, and renal cell cancer [30,31,32,33,65].
In mesothelioma patients, high CRP and low albumin levels have been strongly associated with poor prognosis. The C-reactive protein/albumin ratio (CAR) has also been validated as an independent predictor [66,67]. Previously, our group verified elevated CRP as an independent marker of poor survival in MPM and identified the interaction between CRP and treatment modalities indicating a benefit of surgery within multimodality treatment in selected patients with normal pretreatment CRP levels. [25] Furthermore, the C-reactive protein/albumin ratio as well as the C-NR index (CRP × neutrophil counts) were correlated with histology and disease stage and were able to predict clinical outcome in patients who underwent extrapleural pneumonectomy as preoperative predictors [68].
Another clinically significant major prognostic score for patient stratification for multimodality treatment—the Multimodality Prognostic Score (MMPS)—also included CRP and albumin along with histology and tumor volume and was prospectively validated as a predictive score to allocate patients to surgery in pleural mesothelioma [69,70].
Formerly, we also investigated and found fibrinogen to be an independent prognostic biomarker in MPM with predictive value for treatment benefits achieved by macroscopic complete resection within multimodality therapy [18].
In spite of extensively ongoing research on biomarkers for diagnosis, prognosis, and clinical decisions in mesothelioma, there is no clear consensus in regard to their clinical implementation [71].
Moreover, pleural mesothelioma remains challenging to treat with poor prognosis despite recent developments in the field of immunotherapy and checkpoint inhibitors as well as less aggressive surgical techniques with reduced morbidity. A selected subgroup of patients (<10%) is eligible for radical multimodality treatment including macroscopic complete resection in combination with systemic chemo- and/or immunotherapy and/or radiotherapy with added survival benefit.
The merits of multimodality treatment protocols have been endlessly discussed, often with limited evidence from prospective trials. The prospective Surgery for Mesothelioma After Radiation Therapy (SMART) trial was able to show that eligible patients can benefit from radical treatment modalities [72]. The highly anticipated results from the only randomized clinical trials evaluating the feasibility of surgery, the Mesothelioma and Radical Surgery (MARS) and MARS 2 trials, showed no benefit in survival time in patients who underwent surgery compared to patients treated medically [73,74]. However, several potential problems with the study have been highlighted since and it appears that the controversy about treatment decisions will continue.
So far, treatment allocation in MPM has been subject to a number of unquantifiable parameters such as symptoms and performance status. Accurate biomarker prognostication could potentially improve clinical outcome by supporting early detection and treatment decisions offering multimodality therapy pathways or sparing patients from aggressive and potentially morbid treatment strategies [2,75,76,77,78,79].
A fair prognostic ability of NLR, PLR, CRP, and fibrinogen with respect to overall survival has been demonstrated in the literature in mesothelioma as well as in other malignancies. In our study, these predictors were also validated and found to be strongly associated with survival, thus being selected duly as a basis for a newly developed combined inflammation-based score that was assessed for its prognostic and predictive value in the present analysis in a large cohort in MPM. Moreover, the multivariable analysis determined that this novel inflammatory score was independently associated with survival. In agreement with evidence from the literature, we selected widely accepted, validated, predefined cut-off values to facilitate clinical applicability. The components of the MSIS are easily available and routinely measured in blood analyses in clinical work-up at the time of diagnosis before treatment decisions with the potential of identifying patients who may benefit from multimodality treatment protocols. MSIS in mesothelioma was able to indicate prognosis by stratifying patient groups with significant survival differences. Higher scores were significantly associated with reduced survival. Additionally, MSIS predicted a survival benefit of aggressive multimodality treatment including surgery in patients with low scores. Patients with low scores had a significantly longer overall survival when undergoing surgery within multimodality therapy compared to chemo- and/or radiotherapy alone, while both treatment subgroups with elevated scores had comparably poor survival.
One limitation of this study is the retrospective single-center design; however, the score was developed based on a large number of patients with a constant treatment allocation algorithm. Treatment allocation was based on the recommendations of mesothelioma expert guidelines such as the National Comprehensive Cancer Network (NCCN) guidelines, the American Society of Clinical Oncology Clinical Practice Guidelines (ASCO), the ERS/ESTS/EACTS/ESTRO guidelines (European Respiratory Society [ERS]/European Society of Thoracic Surgeons [ESTS]/European Association for Cardio-Thoracic Surgery [EACTS]/European Society for Radiotherapy and Oncology [ESTRO]), and the ESMO Clinical Practice Guidelines (European Society for Medical Oncology). Due to the retrospective study design, treatment allocation may still reflect a selection bias. Validation of the score, ideally in a prospective setting, is warranted. Overall, these findings encourage the initiation of further large-scale investigations to prospectively assess the role of inflammation-based markers in terms of prediction in clinical practice and treatment decisions. Determination of serum markers should be a subject of extensive research as they are easy to obtain and may contribute to better patient selection in mesothelioma treatment. As described, existing evidence suggests that inflammation-related scoring systems are associated with high prognostic value, but limits still exist. The literature lacks prospective evaluations that are needed to confirm the results. Moreover, the ability of inflammation scoring to clarify the role of different treatment approaches in patients’ outcomes needs to be further investigated.
5. Conclusions
The Mesothelioma Systemic Inflammation Score predicted benefits from macroscopic complete resection as part of multimodality treatment in distinct patients.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Robinson B.M. Malignant pleural mesothelioma: An epidemiological perspective Ann. Cardiothorac. Surg.2012149149610.3978/j.issn.2225-319X.2012.11.0423977542 PMC 3741803 · doi ↗ · pubmed ↗
- 2Brims F. Epidemiology and Clinical Aspects of Malignant Pleural Mesothelioma Cancers 202113419410.3390/cancers 1316419434439349 PMC 8391310 · doi ↗ · pubmed ↗
- 3Rusch V.W. Giroux D. Kennedy C. Ruffini E. Cangir A.K. Rice D. Pass H. Asamura H. Waller D. Edwards J. Initial analysis of the international association for the study of lung cancer mesothelioma database J. Thorac. Oncol.201271631163910.1097/JTO.0b 013e 31826915 f 123070243 · doi ↗ · pubmed ↗
- 4Rusch V.W. Chansky K. Kindler H.L. Nowak A.K. Pass H.I. Rice D.C. Shemanski L. Galateau-Salle F. Mc Caughan B.C. Nakano T. The IASLC Mesothelioma Staging Project: Proposals for the M Descriptors and for Revision of the TNM Stage Groupings in the Forthcoming (Eighth) Edition of the TNM Classification for Mesothelioma J. Thorac. Oncol.2016112112211910.1016/j.jtho.2016.09.12427687962 · doi ↗ · pubmed ↗
- 5Van Gerwen M. Alpert N. Wolf A. Ohri N. Lewis E. Rosenzweig K.E. Flores R. Taioli E. Prognostic factors of survival in patients with malignant pleural mesothelioma: An analysis of the National Cancer Database Carcinogenesis 20194052953610.1093/carcin/bgz 00430649229 PMC 6556702 · doi ↗ · pubmed ↗
- 6Linton A. Pavlakis N. O’Connell R. Soeberg M. Kao S. Clarke S. Vardy J. van Zandwijk N. Factors associated with survival in a large series of patients with malignant pleural mesothelioma in New South Wales Br. J. Cancer 20141111860186910.1038/bjc.2014.47825188323 PMC 4453733 · doi ↗ · pubmed ↗
- 7Nojiri S. Gemba K. Aoe K. Kato K. Yamaguchi T. Sato T. Kubota K. Kishimoto T. Survival and prognostic factors in malignant pleural mesothelioma: A retrospective study of 314 patients in the west part of Japan Jpn. J. Clin. Oncol.201141323910.1093/jjco/hyq 15920798232 · doi ↗ · pubmed ↗
- 8Edwards J.G. Abrams K.R. Leverment J.N. Spyt T.J. Waller D.A. O’Byrne K.J. Prognostic factors for malignant mesothelioma in 142 patients: Validation of CALGB and EORTC prognostic scoring systems Thorax 20005573173510.1136/thorax.55.9.73110950889 PMC 1745842 · doi ↗ · pubmed ↗