Incidence Rates of Cutaneous Immune-Related Adverse Events in Patients with Lung Cancer: A Systematic Review and Meta-Analysis
Zhihui Yang, Yuanyuan Luo, Ruiqi Lu, Xinqi Liu, Hanyu Liu, Suting Liu, Chen Huang, Jinhui Tian, Lili Zhang

TL;DR
This study finds that about 20% of lung cancer patients experience skin-related side effects from immune therapy, with higher rates in those on combined treatments.
Contribution
The study provides the first comprehensive meta-analysis of cirAE incidence in lung cancer patients treated with ICIs.
Findings
The pooled incidence of cirAEs in lung cancer patients is 20.26%.
Subgroup analyses show significant variation in cirAE rates based on treatment type and diagnostic criteria.
Combined or dual ICI therapies are associated with higher cirAE incidence.
Abstract
Objective: Cutaneous immune-related adverse events (cirAEs) represent a prevalent manifestation of adverse reactions linked to immune checkpoint inhibitors (ICIs) therapy, substantially affecting patients’ quality of life. This systematic review and meta-analysis aimed to quantify the pooled incidence of cirAEs in this population and strengthen clinical awareness for early recognition and management. Methods: A comprehensive search of PubMed, Embase, CINAHL, Cochrane Library, CBM, CNKI, and Wanfang databases was conducted from inception to December 2022. Literature that reported the incidence of cirAEs in patients with lung cancer receiving ICIs therapy was included. A meta-analysis was conducted using R software, version 4.4.1 to estimate the pooled incidence of cirAEs, and a random-effects model was used for data synthesis. Begg’s rank correlation and funnel plots were used to assess…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
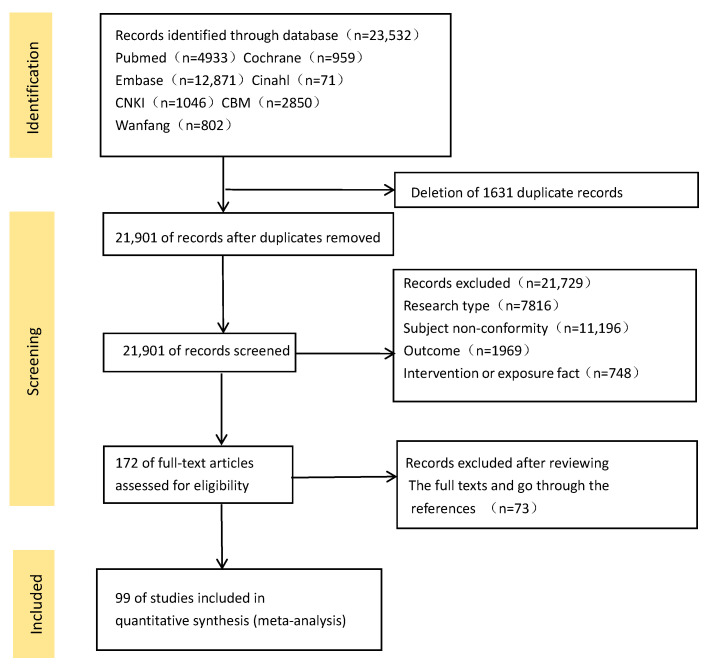 Figure 1
Figure 1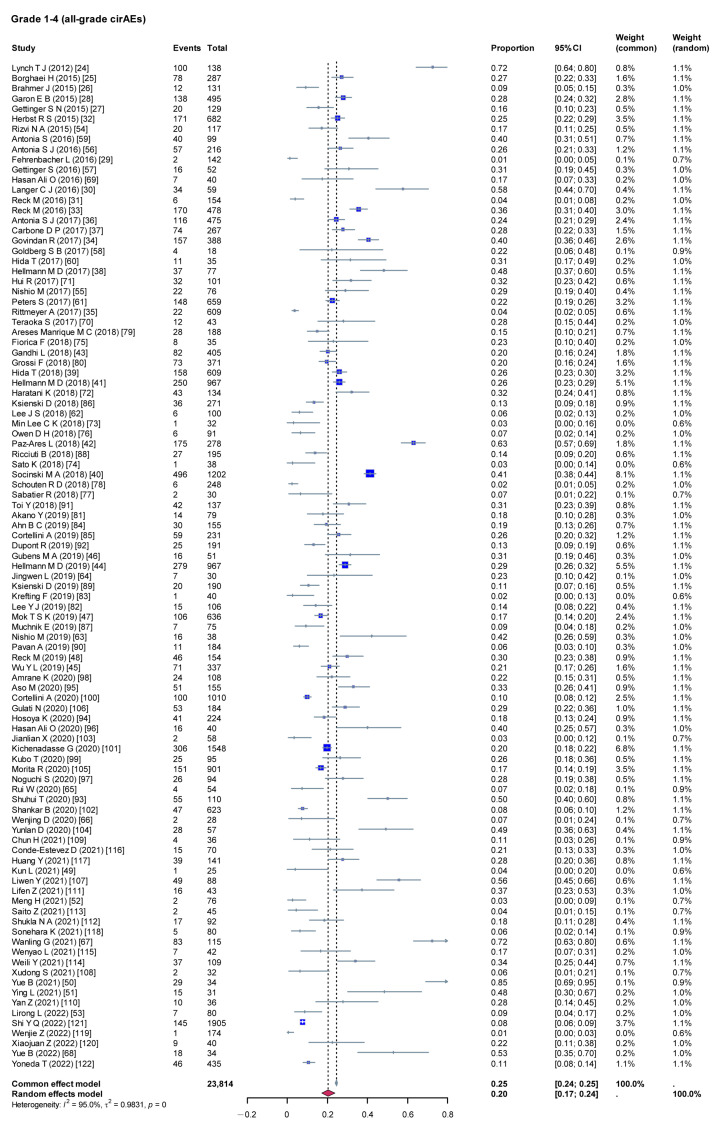 Figure 2
Figure 2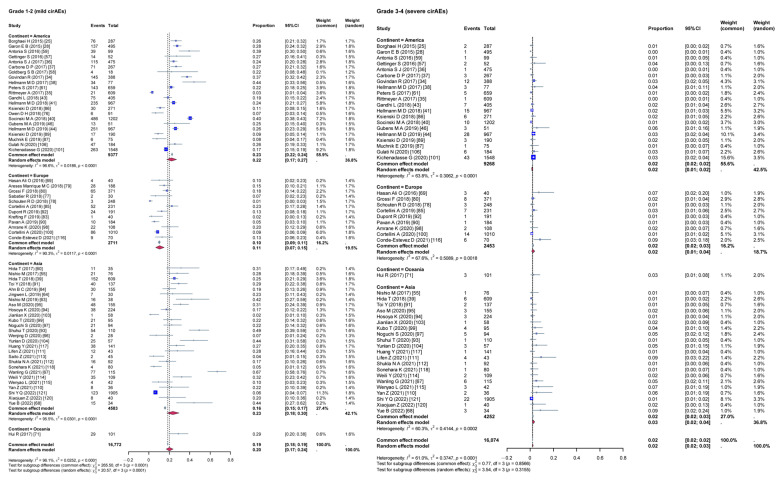 Figure 3
Figure 3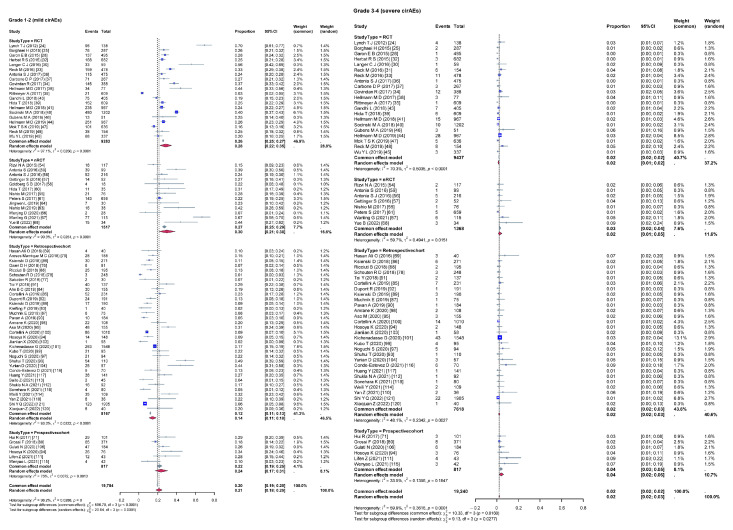 Figure 4
Figure 4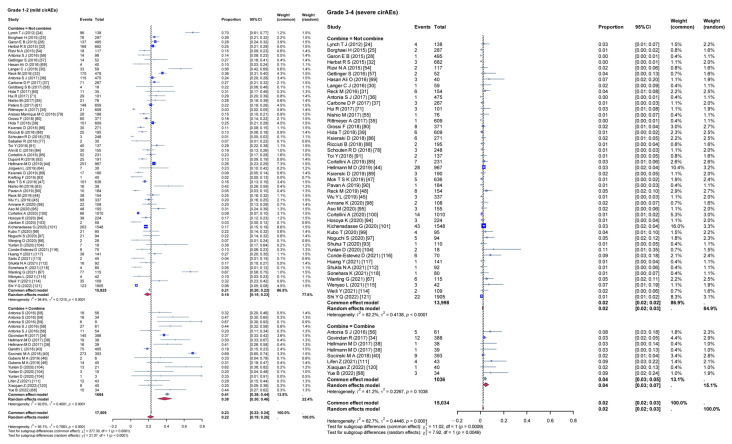 Figure 5
Figure 5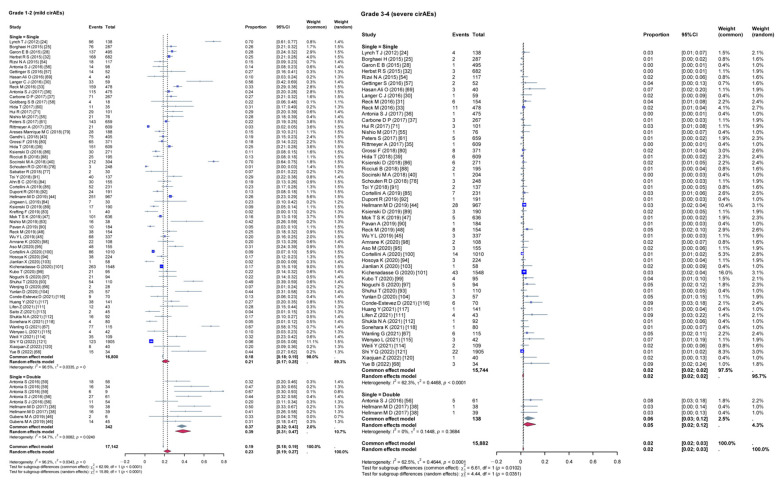 Figure 6
Figure 6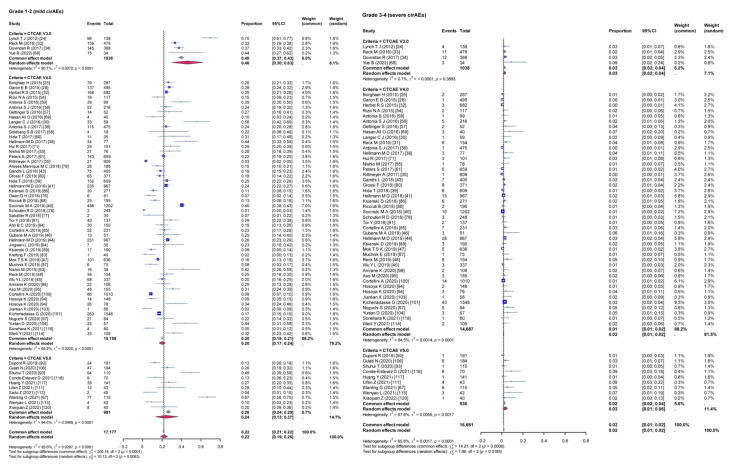 Figure 7
Figure 7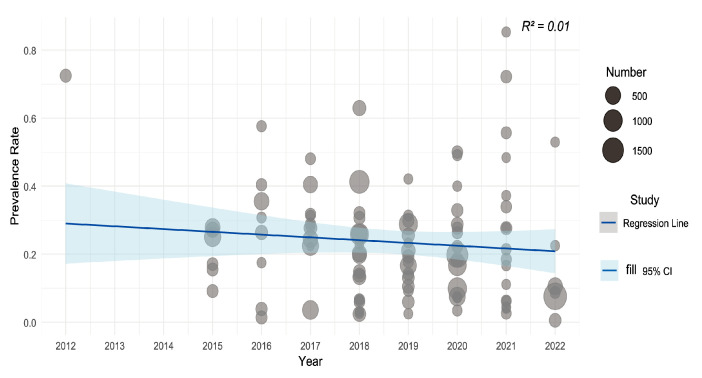 Figure 8
Figure 8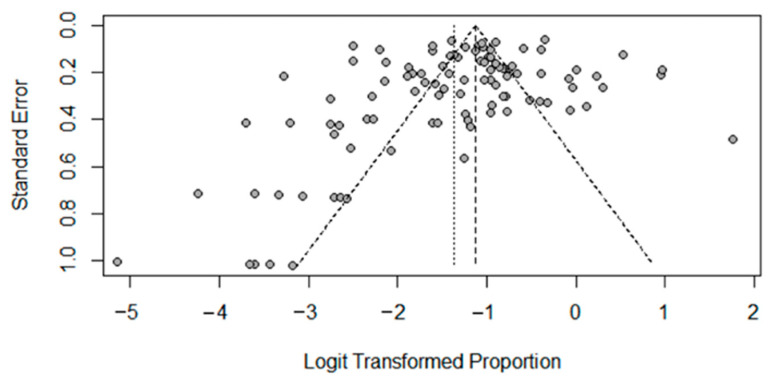 Figure 9
Figure 9- —Youth Project of the National Natural Science Foundation of China
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCancer Immunotherapy and Biomarkers · Immunotherapy and Immune Responses · Drug-Induced Adverse Reactions
1. Introduction
According to Global Cancer Statistics, there has been a rapid increase in the incidence and mortality rates of cancer worldwide [1]. In 2022, approximately 4.82 million new cancer cases were recorded in China [2]. Lung cancer is one of the most lethal cancers in the world [3]. Non-smallcell lung cancer (NSCLC) accounts for approximately 85% of all lung cancer cases and accounts for more than 80% of newly diagnosed lung cancers [4].
Cancer treatment has recently benefited from the introduction of immune checkpoint inhibitors (ICIs), providing a better and longer clinical response [5]. ICIs therapy has already entered clinical practice in the upfront setting either alone (pembrolizumab) or in combination with chemotherapy [6], as well as in locally advanced NSCLC after chemo-radiotherapy [7]. The introduction of ICIs therapy has significantly improved the outcomes of patients with cancer, especially in terms of survival rates. ICIs work differently from standard anticancer therapies. However, their wide application can lead to immunity-related adverse events. Although blocking the negative regulatory signals of T cells may be abnormal, it can also alleviate immunosuppression and enhance normal immune response [8]. The gastrointestinal tract, endocrine glands, skin, and liver are the organs most affected by these adverse events [9]. Adverse events of any grade occur in approximately 30% of patients, and toxic effects of grades 3, 4, or 5 occur in up to 10% of cases of NSCLC [10]. Immune-related adverse events not only affect the patient’s quality of life but can also result in the reduction in or discontinuation of antitumor medications, which may affect the treatment [11,12,13]. Cutaneous immune-related adverse events (cirAEs) appear to be one of the most common forms of immune-related adverse events, including pruritus, rash, skin capillary endotheliosis, oral mucosal lichenoid reaction, Sjögren’s syndrome, bullous pemphigoid, vitiligo, and Stevens–Johnson syndrome [14,15].
Prior research indicates significant variability in cirAEs incidence, with anti-PD-1/PD-L1 therapies showing rates of 30–40% and anti-CTLA-4 treatments exhibiting up to 50% [16]. Another study reported a lower incidence of cirAEs. Among patients receiving CTLA-4 inhibitor therapy, the incidence of cirAEs is 43–45%, compared to approximately 18–23% for those undergoing PD-1 inhibitor treatment [17]. Notably, investigations also found variations in the incidence of cirAEs across cancer types. A systematic review and meta-analysis by Wang et al. [18] encompassing 125 clinical trials with 20,128 patients revealed that the lowest incidence was observed in lung cancer (1.55%; 95% CI, 1.23–1.81%), which was not much different from the highest mean incidence of all adverse events documented in melanoma (1.72%; 95% CI, 1.45–2.27%). Such variation may lead to confusion among health professionals. Conducting a comprehensive analysis of cirAEs incidence can serve as a valuable reference for guiding clinical practice. Other systematic reviews have evaluated immune-related adverse events and the safety of one or more ICI classes [19,20,21]. Moreover, some studies have had limited database searches for a specific period. None of these articles were included in the Chinese articles, which may have led to bias in the incidence of cirAEs. Accurate estimation of cirAEs incidence is critical for developing effective control and prevention programs. Thus, this review aimed to identify the incidence of cirAEs in patients with lung cancer receiving ICIs therapy.
2. Methods
This meta-analysis was registered in the PROSPERO (CRD42023446074), and the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines [22] were implemented for reporting. As this was a meta-analysis review, approval from an ethics committee was not required.
2.1. Search Strategy
We searched eight databases, including PubMed, Embase, CINAHL, Cochrane Library, CBM, CNKI, and Wanfang, from inception up to 31 December 2022. A combination of MeSH terms and free-text terms was used. Initial key words included “Neoplasm”, “neoplas*”, “tumor*”, “cancer*”, “malignan*”, “carcinoma*”, “Immunotherapy”, “Immune Checkpoint Inhibitors”, “skin”, “irAEs”, “cirAEs”, “derma*”, and “cut*”. The Medical Subject Headings (MeSH) of each key search term and combinations were explored in every database. Boolean operators, such as ‘AND’ and ‘OR’, were used to search for relevant studies. In addition, a search of gray literature was conducted, including the Virginia Henderson International Nursing Library and Google Scholar. We also found additional articles by searching for relevant published meta-analyses for forward and backward citation tracking of the included studies. In the Supplementary Materials, we have provided a detailed description of the search strategy (see Supplementary File S1), which focuses solely on the study of humans and adults in English and Chinese. A list of references to relevant articles was examined to identify additional articles.
2.2. Inclusion and Exclusion Criteria
The criteria were as follows: (1) the participants were patients with lung cancer receiving therapy; (2) reporting data on the incidence rate or risk factors of cirAEs; and (3) the research design included a non-randomized controlled trial (nRCT) (including cross-sectional, case–control, and quasi-experimental studies), cohort studies, and a randomized controlled trial (RCT). The exclusion criteria were as follows: (1) studies that were not in English or Chinese, (2) studies with incomplete data or data that could not be analyzed, and (3) duplicate articles and/or data (selected the most recent article).
2.3. Data Extraction and Outcomes
Two reviewers (Yuanyuan Luo and Xinqi Liu) independently screened the literature and extracted data after importing the documents into Excel. The process of literature screening was as follows: excluding duplicate studies, reading the titles and abstracts to exclude clearly irrelevant articles (unrelated to outcome of interest) based on the inclusion criteria, and reading the full text to further determine their suitability. The following data were extracted: study characteristics (author, year, country, language, design, sample size, and diagnostic criteria), characteristics of the participants, drug, cancer stage, incidence rate or risk factors of cirAEs. Any disagreements in the data were resolved by a third partner (Ruiqi Lu).
2.4. Quality Assessment
The included studies were independently evaluated for methodological quality by two authors (Yuanyuan Luo and Zhihui Yang) applying the JBI critical appraisal checklist [23] (see Supplementary File S2). If disagreement occurred, the reviewers reached a consensus, with a third reviewer (Ruiqi Lu) resolving disagreements or discussing them within the team if needed. Data synthesis and analysis we used statistical software R, version 4.4.1 (with ggplot2 and forest plot packages). Due to the different measurements used in these enrolled studies, effect size was used to evaluate the incidence rate. Statistical significance was defined as a two-tailed p < 0.05. The I^2^ statistics and p value were used to assess heterogeneity. If I^2^ ≤ 50% and p > 0.1, heterogeneity was considered statistically significant and aggregated using a fixed-effects model. If I^2^ was >50% and p < 0.1, a random-effects model was used. Sensitivity analyses were performed to examine the stability of the pooled outcomes, and meta-regression analyses were conducted to explore the relationship between the year of publication and incidence of cirAEs. Subgroup analyses were based on continent, study type, combination therapy group, dual ICIs therapy group, and diagnostic criteria of cirAEs. Funnel plots were used to assess potential publication bias.
3. Results
3.1. Study Selection
The search identified 23,532 relevant studies from nine databases, of which 1631 studies were excluded due to duplication, and 21,729 studies were omitted based on titles and abstracts. Of these, 172 were selected for full-text screening. After reviewing the full texts and reviewing the references, 99 articles [24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51,52,53,54,55,56,57,58,59,60,61,62,63,64,65,66,67,68,69,70,71,72,73,74,75,76,77,78,79,80,81,82,83,84,85,86,87,88,89,90,91,92,93,94,95,96,97,98,99,100,101,102,103,104,105,106,107,108,109,110,111,112,113,114,115,116,117,118,119,120,121,122] met the criteria. The reasons for exclusion and the process details are shown in Figure 1.
3.2. Characteristics of the Included Studies
Across studies, sample sizes ranged from 18 to 1905, totaling 23,814 samples. The incidence rate was 20.26% [95% CI 17.12–23.81)]. Among the 99 studies, 30 were RCTs, 15 were nRCTs, and 54 were cohort studies. The studies were published between 2012 and 2022 and their characteristics are shown in Table 1, Table 2 and Table 3.
3.3. Incidence Rate of Cutaneous Immune-Related Adverse Events
A heterogeneity test was performed on the 99 included studies, and the results show high heterogeneity (I^2^ = 95%, p < 0.001); therefore, a random-effects model was used to combine the effect values. Meta-analysis results show that the incidence rate of cirAEs was 20.26% (95% confidence interval [CI], 0.1712–0.2381), as shown in Figure 2.
We also analyzed the real-world data from the European Union pharmacovigilance database (EudraVigilance) up to 9 March 2025 for ICIs—including PD-1 inhibitors (pembrolizumab, nivolumab, toripalimab), PD-L1 inhibitors (atezolizumab, durvalumab), and the CTLA-4 inhibitor ipilimumab—commonly used in lung cancer therapy. The aggregated incidence of skin and subcutaneous tissue disorders varied significantly across these agents, with no stratification by specific cancer types. Ipilimumab (Yervoy), a CTLA-4 inhibitor, exhibited the highest incidence rate (15.73%, 2865/18,215 cases). Among PD-1 inhibitors, pembrolizumab (Keytruda) showed a slightly elevated incidence compared to nivolumab (Opdivo) (13.97% [7254/51,928] vs. 13.64% [5654/41,438]), while toripalimab (Loqtorzi) data remained inconclusive due to insufficient reports (0/1 case). PD-L1 inhibitors demonstrated the lowest adverse event rates, with atezolizumab (Tecentriq) at 8.95% (949/10,606) and durvalumab (Imfinzi) at 7.03% (633/8998).
3.4. Subgroup Analysis
Given the high heterogeneity among the included studies, a subgroup analysis was conducted to evaluate the impact of various variables on the incidence rates of cirAEs. The analysis compared the incidence rates of different grades of cirAEs across subgroups defined by continent (Figure 3), study type (Figure 4), combination therapy (Figure 5), dual ICIs therapy (Figure 6), and diagnostic criteria for cirAEs (Figure 7). As illustrated in Figure 3, Figure 4, Figure 5, Figure 6 and Figure 7, statistically significant differences were observed between all the subgroups for Grade 1–2 and Grade 3–4 cirAE incidences.
3.5. Meta Regression
The bubble plot (Figure 8) shows the estimated regression slope for rash incidence and publication time (years). There was no statistically significant relationship between the year of publication and the incidence of cirAEs (R^2^ = 0.01, p = 0.2628). The incidence of cirAEs showed a decreasing trend.
3.6. Risk Factors for cirAEs in Patients with Lung Cancer Receiving ICIs
Due to the small number of study factors and the large difference in the included risk factors, it was impossible to conduct a combined analysis of the data; therefore, a descriptive analysis of the risk factors of cirAEs was conducted. In terms of demographic data, female patients [93,107] and older patients [80] had a higher incidence of cirAEs. This may be due to damage to the skin barrier structure caused by excessive skincare cleaning, cosmetic use, and excessive use of household chemicals (laundry detergent, dishwashing liquid, etc.) in the female population [93]. Physiological changes and comorbidities in older patients can lead to increased susceptibility to drug-related toxicities [80]. In terms of disease-related data, factors such as cancer stage [93,107], allergy history [93], drug type, and drug combination [93] may influence cirAEs. In patients with advanced tumors (stage II and above), the tumor’s impact and their compromised bodily functions combine to elevate the risk of cirAEs. Patients with a history of allergies are more likely to develop cirAEs after ICIs therapy. CirAEs are more common in patients with a history of chemotherapy. In terms of blood indicators, rheumatoid factors may be risk factors for cirAEs [91,95]. Among patients with pre-existing rheumatoid factors, the incidence of cirAEs was elevated compared to those without it.
3.7. Publication Bias
The Egger test was used to check the publication bias of the included literature, and the test results show that the difference was not statistically significant (t = 1.46, p = 0.1478), and the scatter distribution in the funnel plot (Figure 9) was basically symmetrical and uniform, so it could be considered that there was no publication bias.
4. Discussion
The incidence of cirAEs in patients receiving ICIs therapy is high and should be given sufficient attention. A total of 99 studies published between 2012 and 2022 were included in this study, and the incidence and risk factors of ICIs therapy were described through a systematic review and meta-analysis. The overall incidence of cirAEs was 20.26%. A similar incidence was reported in another study. A systematic review of cirAEs reported an incidence of 20.8% among NSCLC patients, with rash and pruritus occurring rates at of 12.4% and 10.4%, respectively [123]. Meta-analysis enhances drug safety evaluation by aggregating data across studies, compensating for the limited sample sizes of individual clinical trials. However, key challenges include the following: differing incidence rates of adverse events across studies, the possible infrequency of specific target adverse events, and incomplete or inconsistent reporting of adverse events, especially when event counts were below predefined thresholds. Excluding such censored data can bias incidence estimates, necessitating careful handling to ensure accurate statistical inferences [124].
ICIs therapy has achieved remarkable progress in lung cancer treatment, significantly extending patients’ survival time. However, with its widespread use, cirAEs have emerged as a major adverse effect of ICIs therapy. To date, no conclusive evidence has established an association between the clinical manifestations of cirAEs and primary tumor types. Current consensus predominantly attributes these events to drug-related toxicity stemming from the pharmacological properties of therapeutic agents. Some scholars speculate that this may be due to the abnormal targeting of dermal antigens by reactivated T cells and inflammation after cross-reaction with normal skin [125,126]. However, the specific mechanism remains under investigation. With the development of ICIs therapy, an increasing number of scholars have found that the appearance of cirAEs does not seem to be detrimental.
A meta-analysis published in JAMA Dermatology showed that an association was observed between the existence of cirAEs and improved cancer prognosis among patients receiving ICIs therapy. These data suggest that cirAEs may have useful prognostic value in ICIs therapy. More large-scale prospective studies are needed to validate and establish the association between cirAEs and survival outcomes [127]. CirAEs indicate a better prognosis, which may be related to the improvement in body immunity [27,31,35,70]. According to Indini et al. [128], the development of immune-related adverse events during treatment demonstrates a strong correlation with significantly improved progression-free survival and overall survival in patients with metastatic melanoma. Notably, among various adverse events, vitiligo occurrence exhibited a specific association with enhanced overall survival outcomes. Therefore, cirAEs may also reflect the treatment effect. However, this has not been observed in lung cancer. In view of the high incidence of cirAEs in patients with ICIs therapy, the attention of clinical staff should be further improved, relevant risk factors should be identified, and active measures should be taken to prevent the occurrence and development of cirAEs, to avoid progression to severe cirAEs, resulting in forced changes in the treatment program, or even interruption.
The meta-analysis revealed significant heterogeneity among the studies. Further subgroup analysis showed that the heterogeneity may be mainly due to differences in the research methodology and diagnostic criteria. Methodological heterogeneity was due to differences in the sample size, exclusion and inclusion criteria, age distribution, and drugs used in the various original studies. These differences may lead to significant variations in the prevalence of cirAEs. Another heterogeneity was mainly due to differences in the measurement tools, which lead to variations in the grades of cirAEs. Currently, the CTCAE scale is a commonly used assessment tool for cirAEs. However, frequent updates to its version and changes in standards over time have led to discrepancies in the findings. Additionally, the frequency and time of evaluation of cirAEs varied in each study. CirAEs exhibit dose-dependence. Short evaluation periods or infrequent assessments may lead to underestimation of their incidence, thereby causing high outcome heterogeneity. To avoid significant heterogeneity among studies and reduce publication bias, it is recommended to establish uniform standards for future studies. This will facilitate the clinical monitoring of the occurrence of cirAEs and improve the comparability between studies.
4.1. Limitations
This study has various limitations that should be acknowledged. First, this study solely queried the EudraVigilance database without integrating real-world data from other pharmacovigilance databases into the comprehensive assessment of cirAEs incidence, which may limit the validity of the findings. Second, although the statistical results from Figure 9 indicate no publication bias, this meta-analysis of adverse event incidence may be subject to potential overestimation bias due to selective reporting, which could influence the pooled estimates of circulating cirAEs in this review. Additionally, cirAEs exhibit a time-dependent pattern—their incidence increases with prolonged treatment duration and cumulative drug exposure. However, inconsistent definitions of “cirAEs initiation time” across studies created uncertainty in evaluating dose–response relationships. Third, significant methodological heterogeneity in diagnostic tools, monitoring frequency, and follow-up durations (e.g., variations in CTCAE versions) persisted despite subgroup analyses. Furthermore, language barriers limited inclusion to Chinese and English literature, potentially omitting critical evidence from other languages. Notably, the research team’s affiliation with the JBI Center for Evidence-Based Practice predisposed us to favor JBI assessment tools, which may affect methodological objectivity.
4.2. Implications for Further Research
Future studies on patients receiving ICIs therapy should provide a comprehensive classification of cirAEs and a longer documentation period to better understand their occurrence and patterns. Moreover, future studies must explore the factors that influence cirAEs and their correlation with other immune-related adverse events.
5. Conclusions
This study’s results indicate that patients with lung cancer who use immune checkpoint inhibitors are more likely to experience grade 1 and 2 cirAEs compared to those with grades 3 and 4. Combination therapy and dual ICIs therapy can increase the incidence of cirAEs in patients with lung cancer. Regular follow-up and identification of risk factors can help manage and reduce the symptoms of these adverse events. To further explore the incidence and risk factors of cirAEs on patients receiving ICIs therapy, a large-scale, multi-center study is recommended. Health professionals should pay close attention to patients with cirAEs after ICIs therapy and take the necessary measures to manage and reduce the incidence of such events.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Sung H. Ferlay J. Siegel R.L. Laversanne M. Soerjomataram I. Jemal A. Bray F. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries CA Cancer J. Clin.20217120924910.3322/caac.2166033538338 · doi ↗ · pubmed ↗
- 2Xia C. Dong X. Li H. Cao M. Sun D. He S. Yang F. Yan X. Zhang S. Li N. Cancer statistics in China and United States, 2022: Profiles, trends, and determinants Chin. Med. J.202213558459010.1097/CM 9.000000000000210835143424 PMC 8920425 · doi ↗ · pubmed ↗
- 3Fitzmaurice C. Abate D. Abbasi N. Abbastabar H. Abd-Allah F. Abdel-Rahman O. Abdelalim A. Abdoli A. Abdollahpour I. Abdulle A.S.M. Global, regional, and national cancer incidence, mortality, years of life lost, years lived with disability, and disability-adjusted life-years for 29 cancer groups, 1990 to 2017: A systematic analysis for the global burden of disease study JAMA Oncol.201951749176810.1001/jamaoncol.2019.299631560378 PMC 6777271 · doi ↗ · pubmed ↗
- 4Dos Santos Garrett N.F.M. Da Costa A.C.C. Damiani G. Vasques C.I. Patients with lung cancer undergoing immune checkpoint inhibitors: A meta-analysis of dermatological toxicities Crit. Rev. Oncol. Hematol.202015210298310.1016/j.critrevonc.2020.10298332570149 · doi ↗ · pubmed ↗
- 5Collins L.K. Chapman M.S. Carter J.B. Samie F.H. Cutaneous adverse effects of the immune checkpoint inhibitors Curr. Probl. Cancer 20174112512810.1016/j.currproblcancer.2016.12.00128190531 · doi ↗ · pubmed ↗
- 6Russo A. Franchina T. Ricciardi G.R.R. Toscano G. Schifano S. Lo Certo G. Battaglia A. PantòE. Scaffidi Fonti M. Adamo V. The changing scenario of 1st line therapy in non-oncogene addicted NSCL Cs in the era of immunotherapy Crit. Rev. Oncol. Hematol.201813011210.1016/j.critrevonc.2018.06.00730196906 · doi ↗ · pubmed ↗
- 7Murakami S. Durvalumab for the treatment of non-small cell lung cancer Expert. Rev. Anticancer. Ther.2019191009101610.1080/14737140.2019.169940731782989 · doi ↗ · pubmed ↗
- 8Wu L.X. Li S.L. Du X.P. Han Z.X. Cutaneous adverse events (A Es) of immunotherapy in patients with advanced non-small-cell lung cancer(NSCLC):A Meta-analysis and systematic review J. Mod. Oncol.2022301388139310.3969/j.issn.1672-4992.2022.08.010 · doi ↗