Performance Evaluation of the New High-Sensitivity Cardiac Troponin I Immunoassay on CL-2600i Mindray Analyzer
Flaminia Tomassetti, Denise Fiorelli, Edoardo Cappa, Alfredo Giovannelli, Martina Pelagalli, Silvia Velocci, Eleonora Nicolai, Marilena Minieri, Marco Alfonso Perrone, Sergio Bernardini, Massimo Pieri

TL;DR
This study compares a new high-sensitivity cardiac troponin test from Mindray with an existing Abbott test, finding them to perform similarly in detecting heart injury.
Contribution
The study validates a new high-sensitivity cardiac troponin I immunoassay on the CL2600i Mindray analyzer for clinical use.
Findings
The Mindray hs-cTnI test showed strong correlation with the Abbott system (plasma R2: 0.974; serum R2: 0.995).
The test demonstrated excellent analytical performance with a high detection rate in healthy individuals (79%).
Linearity was confirmed within the measuring range (R2: 0.994).
Abstract
Background: International guidelines recommend the use of high-sensitivity cardiac troponin (hs-cTn) I and T methods for the detection of myocardial injury as a pre-requisite for the diagnosis of acute myocardial infarction (AMI) in patients admitted to the emergency department. Recently, Mindray (Mindray Bio-Medical Electronics Co., Ltd., Shenzhen, China) has introduced a new chemiluminescence immunoassay (CLIA) for the detection of the cTn complex. The present study aims to verify and validate the hs-cTnI Mindray assay on the new automated CL2600i analyzer compared to the routine Alinity-i series instrument by Abbott (Abbott, Chicago, IL, USA). Methods: This study evaluated linearity, precision through the 5 × 5 protocol, methodological comparison on plasma and serum matrices, hs-cTnI 99th percentile imprecision, and the hs-cTnI detection rate in a healthy population. Results: The…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
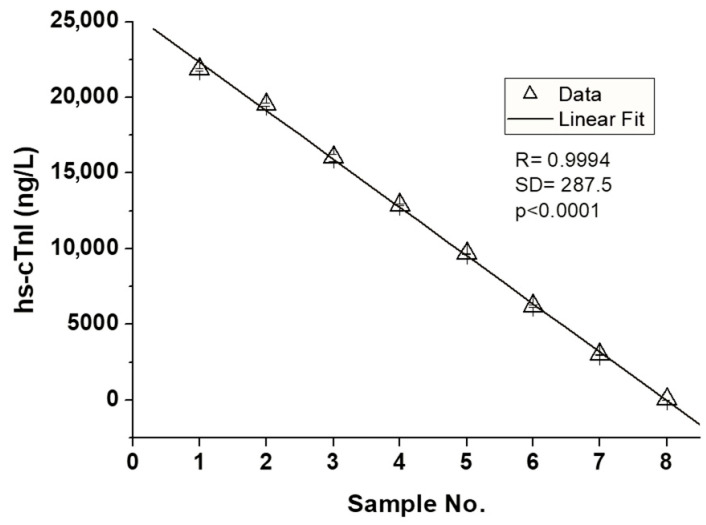 Figure 1
Figure 1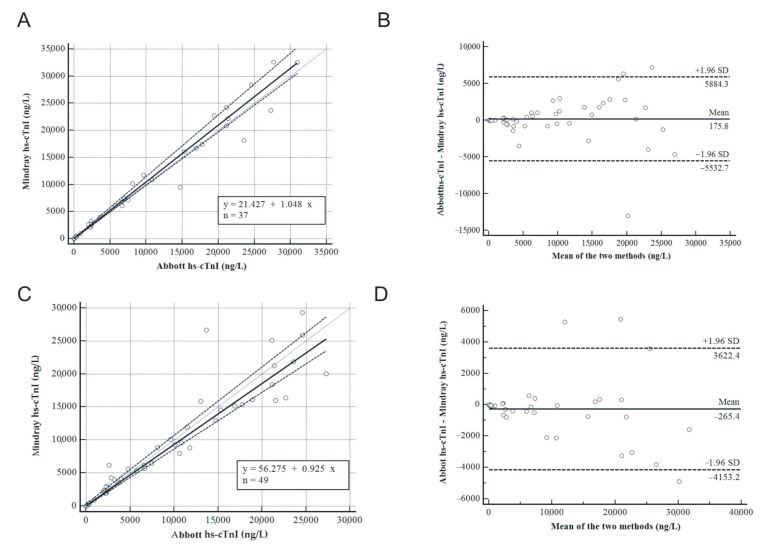 Figure 2
Figure 2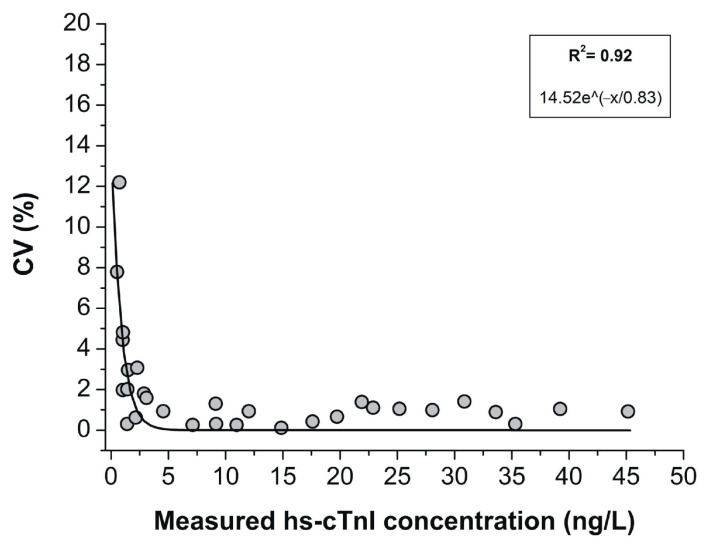 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAcute Myocardial Infarction Research · ECG Monitoring and Analysis · Cardiac electrophysiology and arrhythmias
1. Introduction
Cardiac troponin, particularly high-sensitivity cardiac troponin (hs-cTn) I and T tests are essential tools for the early and accurate diagnosis of acute myocardial infarction (AMI) [1]. In 2018, the Fourth Universal Definition of Myocardial Infarction [2] established that a myocardial injury is present when a single hs-cTnI or hs-cTnT value above the 99th percentile URL (Upper Reference Limit) occurs. Accordingly, the most recent international guidelines recommend the use of hs-cTnI and hs-cTnT methods for the detection of myocardial injury as a pre-requisite for the diagnosis of AMI in patients admitted to the emergency department [2,3]. In patients undergoing cardiac revascularization, particularly per cutaneous procedures, measuring hs-cTn levels is also essential for identifying any per procedural ischemic episodes. As recently shown, these occurrences are not unusual and significantly affect prognosis [4].
Moreover, the 2018 Expert opinion from the International Federation Clinical Chemistry and Laboratory Medicine (IFCC) and American Association for Clinical Chemistry (AACC) [5] recommends that the high-sensitivity assay for cTnI and cTnT should meet two key criteria: 1. it should measure the 99th percentile URL with an imprecision (expressed as Coefficient of Variation, %CV ≤ 10; 2. it should measure cTn concentrations above the Limit of Detection (LoD) of the method in at least 50% of healthy subjects enrolled in large populations, including more than 300 men and 300 women [6].
Circulating levels of hs-cTnI and hs-cTnT have been found to increase progressively after 55 years of age in asymptomatic men and women enrolled in multicenter studies including large reference populations [3,7,8,9]. Many clinical studies and some meta-analyses have recently confirmed that some individuals, apparently free from any cardiac disease, have hs-cTnI or hs-cTnT concentrations in the third tertile of biomarker distribution values (i.e., still below the 99th percentile URL cut-off value), presenting a higher risk of early cardiac or non-cardiac mortality and rapid progression to heart failure [10,11]. Additionally, it is important to emphasize that hs-cTnI and hs-cTnT are distinct cardiac-specific biomarkers, each exhibiting a biological variability around 10%CV. The individuality index expresses the relationship between the intra-individual variability and the general variability among individuals for a specific biomarker. For cardiac troponins, the individuality index is ≤0.3, making repeated single measurements more clinically manageable compared to the analytical range [12]. Considering the methodological point of view, other manufacturers have developed different immunoassays to measure cTn in serum and/or plasma. In this context, it is possible to understand differences registered among different commercial immunoassays with regard to reference ranges, specimen type (serum, heparin/EDTA plasma), different epitope specificity of capture and detection antibodies, LoD, and percentage of %CV at the 99th percentile [13].
Furthermore, the IFCC Task Force on Clinical Applications of Cardiac Biomarkers addressed the question of whether cTn harmonization could be achieved through a secondary reference material based on a pooled serum. However, harmonization between assays remains elusive [14]. Nowadays, the market is addressing cTnI, as an assay target, rather than cTnT. The cTnI appears to be a more specific cardiac biomarker of AMI, whereas cTnT is more strongly associated with the risk of non-cardiovascular disease [15]. However, measurements of cTnI are influenced by multiple factors, including proteolytic degradation, phosphorylation, complexing with cTnC, heparin, heterophile or human antimouse antibodies, and cTnI-specific autoantibodies [16]. In addition, the path of hs-cTns has become even more uncertain with the renewed interest in hs-cTns fragments [17,18,19].
Recently, Mindray (Mindray Bio-Medical Electronics Co., Ltd., Shenzhen, China) has introduced a new chemiluminescence immunoassay (CLIA) for hs-cTnI tests. An innovative method with a detection antibody directed towards cTn complexes is used. The most novel feature of this assay is the cTn-complex-assay target. Several studies indicated that cTnI mainly exists in the forms of binary cTnIC complexes and ternary cTnITC complexes in circulation with little free cTnI [20,21]. The Mindray hs-cTnI assay utilized anti-cTn complex antibodies for the detection of the total concentration of binary cTnIC complexes and ternary cTnITC complexes, which was theoretically equivalent to the cTnI concentration. Two papers have been recently published about the verification/validation of hs-cTnI assay. Li et al. validated the Mindray CL8000i instrument in comparison with the Abbott Architect-I [22], while Lippi et al. compared the Mindray CL1200i with Access hs-TnI Beckman Coulter [23]. Results of these studies both demonstrated that the overall performance of the new Mindray assay is comparable to other commercially available methods.
In this study, we report our experience in verifying and validating the Mindray c-hsTnI assay on CL2600i in comparison with the Abbott Alinity-i.
2. Materials and Methods
2.1. Study Design
Serum or plasma samples were collected from residual routine specimens of patients admitted to the emergency department with chest pain symptoms or acute coronary syndrome. A total of 49 lithium heparin plasma and 37 serum samples were used for the comparison of cTnI assay between Alinity-i (Abbott, Abbott Park, IL, USA) and CL-2600i (Mindray, Shenzhen, China) instruments. Samples were centrifuged at 2000× g for 10 min and then processed according to the manufacturer’s instructions.
A total of 400 leftover samples (200 from males and 200 from females, age 18–60 years old, Caucasian ethnicity) from blood donors were collected as the healthy population to evaluate the 99th percentile. The inclusion criteria for the healthy population’s samples were glomerular filtration rate, glycosylated hemoglobin, and NT-proBNP in the range of normality. Participants had no symptoms of heart disease or any history of cardiovascular events. The exclusion criteria were neoplastic diseases, chronic and acute kidney disease, malignancies, recent infections or pharmacological treatment.
This retrospective study was evaluated and approved by the local Ethics Committee at Tor Vergata University Hospital (ID number 41.17) and was carried out according to the Declaration of Helsinki, as revised in 2013.
2.2. Chemiluminescence Immunoassays
The CL-2600i is a new automated immunochemistry (Mindray Bio-Medical Electronics Co., Shenzhen, China) instrument based on the “sandwich” principle. The innovation of the method includes a 4-step magnetic separation system to ensure the effective detachment of immune complexes from magnetic particles. The sample is incubated with the pretreatment solution, paramagnetic microparticles with mouse monoclonal anti-cTnI antibody (HyTest), and mouse monoclonal anticTnI-complex antibodies (HyTest) conjugated with alkaline phosphatase (ALP). After washing, addition of the chemiluminescent substrate (3-(2-helical adamantane) 4-methoxy-4-(3-phosphoxyyl)-phenyl-1,2-dioxane, AMPPD) produces chemiluminescence. The photon counting technique, using a photomultiplier (PMT), detects the light signals produced by the chemiluminescence reaction, converting the signal into a concentration (ng/L). The device is calibrated via an LED reference module, ensuring high measurement accuracy.
The internal quality controls (iQC) were analyzed at every work session.
2.3. Precision Evaluation
Precision estimations were obtained using quintuplicate measurements of aliquots of three pools (low, high, and very high levels of cTnI), performed for a total of 5 replicates each day, respectively, for a total of five days, following the Clinical and Laboratory Standards Institute (CLSI) EP15-A3 protocol [24]. Results obtained for precision evaluation were compared to those claimed by the manufacturer.
2.4. Linearity Assessment
Samples at eight different concentrations within the expected range were used to verify linearity. High-concentration samples were created by pooling samples at a concentration near the limit of linearity; they were then diluted with negative samples, as shown in Table 1. The test was performed three times for each sample concentration. The mean value and standard deviation were then calculated, and the least squares method was used to fit a straight line between the resulting mean values and the dilution ratios. Finally, the correlation coefficient r was calculated in the linear range.
2.5. Repeatability
The repeatability was assessed, analyzing quality controls for each level 20 times. The results are expressed as %CVs, Standard Deviation (SD), mean. The acceptance criteria were set at %CV ≤ 5.
2.6. Methodological Comparison
The comparability of the Mindray hs-cTnI methodological test performed on the CL-2600i platform was assessed with the Abbott hs-cTnI assay on the Alinity-i series. The same samples processed on the Abbott Alinity-i series were subsequently measured on the CL-2600i instrument within three hours.
2.7. hs-cTnI 99th Percentile Imprecision
To calculate the hs-cTnI 99th percentile imprecision, the EP15-A3 protocol was followed [24]. The imprecision profile was plotted according to cTnI concentrations measured with corresponding CVs observed in a series of 30 samples, with hs-cTnI concentrations ranging between LoD values and 99th percentile URLs.
2.8. hs-cTnI Detection Rate in the Healthy Population
The 99th URLs were determined using 400 serum specimens from the healthy population. Based on the measurements of serum specimens obtained by the laboratory records, the sex-specific 99th-percentile URLs were calculated. The detection rate in a healthy population was calculated according to the following formula: number of samples above LoD/total number of samples (LoD values of 0.5 ng/L). The detection rate for the male, female, and overall healthy populations should be ≥50%.
2.9. Statistical Analysis
The 99th percentile upper reference limits (URLs) were determined using serum specimens from a healthy population as previously described. The coefficient of variation (%CV) was calculated as the standard deviation divided by the mean value. Data were considered using standard deviation (SD), Spearman rank correlation coefficient (R^2^), and linear regression equations. Passing–Bablok regression analysis was used to compare the two instruments (Mindray vs. Abbott) and the two matrices (serum vs. plasma and plasma vs. plasma), while the Bland–Altman test was performed to determine the agreement and to investigate the true value (i.e., proportional bias).
All data were analyzed using Med Calc Ver.18.2.18 (MedCalc Software Ltd., Ostend, Belgium) and OriginLab Ver. 6.1 (Northampton, MA, USA).
3. Results
3.1. Precision Study
Precision data of the coefficients of variation obtained in the laboratory are shown in Table 2 in comparison with the data declared by the manufacturer. No significant difference was observed between the %CVs of the two methods (p > 0.05: n.s.), even though the CV values evaluated in the laboratory were slightly higher than the %CV values declared.
3.2. Linearity Analysis
The linearity measurements performed on the Mindray CL-2600i instrument are shown in Figure 1. The dilution performed was obtained by diluting high-value pools with low-value pools. All tested pools of serum samples do not deviate from linearity, with an equation of y = 25,518.56 − 3194.05x.
3.3. Repeatability
Repeatability was assessed by analyzing the three iQC levels 20 times. Results were reported in Table 3. The %CVs evaluated met the acceptance criteria and were CV < 5%.
3.4. Methodological Comparison
Two linear regressions were built using Passing–Bablok analysis to compare the two methods with two different matrices: plasma vs. plasma and plasma vs. serum.
A significant correlation between the two methods for plasma vs. plasma (n = 49) was observed (Figure 2A), with a correlation coefficient of 0.974 (95% Confidence Interval, CI: 0.954 to 0.985) and a p-value less than 0.0001, indicating a strong and statistically significant correlation. The Bland–Altman analysis (Figure 2B) revealed a mean bias between the Alinity-i and CL-2600i instruments of 175.8 ng/L with the upper and lower limits of 5884.3 ng/L and −5532.7 ng/L, respectively. The probability associated with the two-sided test was non-significant (p = non-significant, n.s.), indicating that the differences between the methods are not statistically significant.
A significant correlation between the two methods for plasma vs. serum (n = 37) was observed (Figure 2C), with a correlation coefficient of 0.990 (95% CI: 0.981 to 0.995) and a p-value less than 0.0001, indicating again a strong and statistically significant correlation even in different matrices. The Bland–Altman analysis (Figure 2D) revealed a mean difference between the two instruments of −265.5 ng/L with the upper and lower limits of 3622.4 ng/L and −4152.2 ng/L, respectively. The probability associated with the two-sided test was non-significant (p = n.s.), indicating that the differences between the methods are not statistically significant.
3.5. hs-cTnI 99th Percentile Imprecision
The imprecision profile was plotted (Figure 3) using hs-cTnI concentrations along with the corresponding CVs and SDs observed in a series of 27 samples, with hs-cTnI concentrations ranging from LoD values to the 99th percentile URLs. Results showed a R^2^ of 0.92 and an equation of 14.52 × e^(−x/0.83)^.
3.6. hs-cTnI Detection Rate in Healthy Population
The 99th percentile URLs were evaluated in 200 healthy female and 200 healthy male patients.
A significant difference was observed between the cTnI values of females and males, being 1.17 ng/L and 2.28 ng/L, respectively (p < 0.001). Overall, the samples showed a mean of 1.72 ng/L (SD 1.44 ng/L and 95% CI from 1.52 to 1.92 ng/L).
Therefore, the detection rate in a healthy population, i.e., the number of samples above the LoD of the method on the total samples was 60% for females, 97% for males, and 79% for overall, proving the optimal performance of the test, as can be seen in Table 4.
4. Discussion
As technological advancements continue to enhance the precision of biomarker detection, evaluating the performance of new hs-cTn assays becomes essential. A current issue lies in the variability observed across different commercial immunoassays [25]. These discrepancies arise from various factors, including differences in the reference ranges established by various tests, the type of biological sample used (serum, heparinized plasma, or EDTA plasma), and the specificity of capture and detection antibodies for specific cardiac troponin epitopes [26].
In this context, the Mindray hs-cTnI test on the CL-2600i instrument, utilizing multiple antibodies that recognize cTnI complexes, demonstrates robust analytical performance and minimizes interferences [23], as shown in the results. This design avoided the influence of cTnI degradation and autoantibody interference and improved sensitivity and specificity, leading to better LoB, LoD, and LoQ values and anti-interference performance.
These features not only improve diagnostic accuracy, raising optimal %CVs (3.17, 2.37, and 2.02 for each level of iQC), but facilitate the integration of this method into clinical practice, showing a strong correlation with the routine method in both plasma and serum matrices (R^2^ 0.974 and R^2^ 0.995, respectively). Additionally, to lead to standardization and harmonization of results, the variability in the %CVs at the 99th percentile [21] was evaluated as a 79% detection rate for the total population, 60% for females, and 97% for males, much better than the IFCC recommendations (>50%). These data confirmed that the new Mindray assay is more sensitive than other commercially available tests [23], allowing the detection of very low cTnI concentrations in healthy populations. The use of these advanced methodologies ensures the detection of binary and ternary complexes of cTnI, capturing a broader spectrum of clinically relevant troponin forms released during myocardial injury. Indeed, a recent study explored thresholds and algorithms to investigate the best combination of cTn forms detected by specific immunoassays for diagnosing, monitoring, and follow-up of AMI [17]. This strategy, which involves developing immunoassays that detect troponin complexes rather than individual epitopes, enhances specificity and reduces the likelihood of interference from troponin degradation products or autoantibodies that could compromise assay accuracy [27] and may also be detected in non-AMI patients. High levels of cTn complex are often detected in patients with chronic disease, inflammation status, and in professional athletes [17,28,29,30]. Moreover, in this context, an assay, such as the Mindray test, that meets the criteria of standardization and high sensitivity over the 99th percentile is quite needed in routine practice. The LOD < 0.5 ng/L discriminates the minimal cTn unbalance, even in the possibly healthy individual or in patients with the slightest cardiovascular symptoms. Moreover, highly sensitive cTn can function not only as an effective diagnostic tool for cardiovascular disease (CD), but also as a marker for screening and primary prevention, predicting future risk of cardiovascular events [31,32]. Also, it could increase interest in studying the role of hs-cTnI even in other populations and ethnicities [33,34].
These results highlight the cTnI assay’s high reproducibility, particularly within clinically significant concentration ranges. Linear measurements further validated the assay performance. This indicates that the test provides accurate and proportional responses to varying troponin concentrations, ensuring reliable, even stricter quantification in diverse clinical scenarios, such as the emergency department, and avoiding misclassification [5,13,35,36].
The linearity and precision of the Mindray hs-cTnI test underline its robustness and suitability for clinical application, particularly in contexts requiring high sensitivity and reproducibility. Specifically, the %CVs were consistently low, indicating high reproducibility and reliability across a wide range of troponin concentrations.
While the Mindray hs-cTnI test (and similar tests) is designed to minimize interferences through various mechanisms like reagent optimization or advanced calibration techniques, some degree of interference is still possible, which could impact the accuracy or reliability of the results, especially in samples and autoantibodies, or with heterologous antibodies. Therefore, it is important for healthcare providers to be aware of these potential interferences when interpreting test results [34], especially in patients with autoimmune conditions or those on certain biopharmaceutical treatments.
The findings of this study support the integration of the Mindray hs-cTnI test into clinical practice, particularly in environments where rapid clinical decision-making and high accuracy are critical. Future studies should focus on the clinical application of the Mindray hs-cTnI test in larger and more diverse patient populations to confirm its robustness and utility in routine practice and the biological variability of cTnI analysis.
5. Conclusions
Ongoing research into the standardization and harmonization of hs-cTn assays is crucial, as variations among instruments and tests continue to pose challenges in clinical diagnostics. Advances in assay technology, including the development of even more sensitive detection methods and enhanced specificity, have the potential to improve the accuracy and reliability of cardiac biomarker tests, ultimately leading to better patient outcomes in the management of AMI and other cardiac conditions.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Lazar D.R. Lazar F.-L. Homorodean C. Cainap C. Focsan M. Cainap S. Olinic D.M. High-Sensitivity Troponin: A Review on Characteristics, Assessment, and Clinical Implications Dis. Markers 20222022971332610.1155/2022/971332635371340 PMC 8965602 · doi ↗ · pubmed ↗
- 2Thygesen K. Alpert J.S. Jaffe A.S. Chaitman B.R. Bax J.J. Morrow D.A. White H.D. Executive Group on behalf of the Joint European Society of Cardiology (ESC)/American College of Cardiology (ACC)/American Heart Association (AHA)/World Heart Federation (WHF) Task Force for the Universal Definition of Myocardial Infarction Fourth Universal Definition of Myocardial Infarction (2018)Circulation 2018138 e 618e 65110.1161/CIR.000000000000061730571511 · doi ↗ · pubmed ↗
- 3Apple F.S. Collinson P.O. Kavsak P.A. Body R. Ordóñez-Llanos J. Saenger A.K. Omland T. Hammarsten O. Jaffe A.S. Getting Cardiac Troponin Right: Appraisal of the 2020 European Society of Cardiology Guidelines for the Management of Acute Coronary Syndromes in Patients Presenting without Persistent ST-Segment Elevation by the International Federation of Clinical Chemistry and Laboratory Medicine Committee on Clinical Applications of Cardiac Bio-Markers Clin. Chem.20216773073510.1093/clinchem/hvaa 33733377906 · doi ↗ · pubmed ↗
- 4Armillotta M. Bergamaschi L. Paolisso P. Belmonte M. Angeli F. Sansonetti A. Stefanizzi A. Bertolini D. Bodega F. Amicone S. Prognostic Relevance of Type 4a Myocardial Infarction and Periprocedural Myocardial Injury in Patients With Non–ST-Segment–Elevation Myocardial Infarction Circulation 202515176077210.1161/CIRCULATIONAHA.124.07072939968630 PMC 11913249 · doi ↗ · pubmed ↗
- 5Wu A.H.B. Christenson R.H. Greene D.N. Jaffe A.S. Kavsak P.A. Ordonez-Llanos J. Apple F.S. Clinical Laboratory Practice Recommendations for the Use of Cardiac Troponin in Acute Coronary Syndrome: Expert Opinion from the Academy of the American Association for Clinical Chemistry and the Task Force on Clinical Applications of Cardiac Bio-Markers of the International Federation of Clinical Chemistry and Laboratory Medicine Clin. Chem.20186464565510.1373/clinchem.2017.27718629343532 · doi ↗ · pubmed ↗
- 6Apple F.S. Sandoval Y. Jaffe A.S. Ordonez-Llanos J. IFCC Task Force on Clinical Applications of Cardiac Bio-Markers Cardiac Troponin Assays: Guide to Understanding Analytical Characteristics and Their Impact on Clinical Care Clin. Chem.201763738110.1373/clinchem.2016.25510928062612 · doi ↗ · pubmed ↗
- 7Clerico A. Zaninotto M. Padoan A. Masotti S. Musetti V. Prontera C. Ndreu R. Zucchelli G. Passino C. Migliardi M. Evaluation of Analytical Performance of Immunoassay Methods for C Tn I and C Tn T: From Theory to Practice Adv. Clin. Chem.20199323926210.1016/bs.acc.2019.07.00531655731 · doi ↗ · pubmed ↗
- 8Clerico A. Zaninotto M. Ripoli A. Masotti S. Prontera C. Passino C. Plebani M. The 99th Percentile of Reference Population for C Tn I and C Tn T Assay: Methodology, Pathophysiology and Clinical Implications Clin. Chem. Lab. Med.2017551634165110.1515/cclm-2016-093328599373 · doi ↗ · pubmed ↗