The Pericardium Cells Junctions Are a Target for Autoantibodies of Patients Affected by a Variant of Endemic Pemphigus Foliaceus in El Bagre and Surrounding Municipalities in Colombia, South America
Ana Maria Abreu Velez, Takashi Hashimoto, Yulieth A. Upegui, Jorge Mario Vélez Arango, Adriana Milena Olarte Aponte, Jose A. Vega, Michael S. Howard

TL;DR
This study shows that patients with a variant of pemphigus in Colombia produce autoantibodies targeting heart tissue, particularly cell junctions in the pericardium.
Contribution
The study identifies pericardium cell junctions as a novel target for autoantibodies in a specific variant of pemphigus.
Findings
El Bagre-EPF patient sera showed reactivity with pericardial cell junctions and nerve formations.
Autoantibodies against specific proteins like MIZAP and desmoplakin were found in patients.
Controls showed no such reactivity, confirming the specificity of the findings.
Abstract
Background: Patients suffering from a new variant of endemic pemphigus foliaceus in El Bagre, Colombia, South America (El Bagre-EPF) produce autoantibodies (Abs) to different proteins in the skin (frustre form), as well as to those in other organs (Senear–Usher-like and systemic forms). Here, we hypothesize whether patients’ autoantibodies play a role in triggering epicardium and pericardium autoimmunity and pathogenicity. We based this hypothesis on knowing that these patients frequently show clinical symptoms of the chest and heart, and we hypothesize that the autoantibodies of this disease are the main contributors to the base of the pericardial conditions of these patients. Materials and Methods: A case-control study for testing the sera of patients affected by El Bagre-EPF (n = 45) and matched controls from the endemic area (n = 45) was conducted to evaluate reactivity with the…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
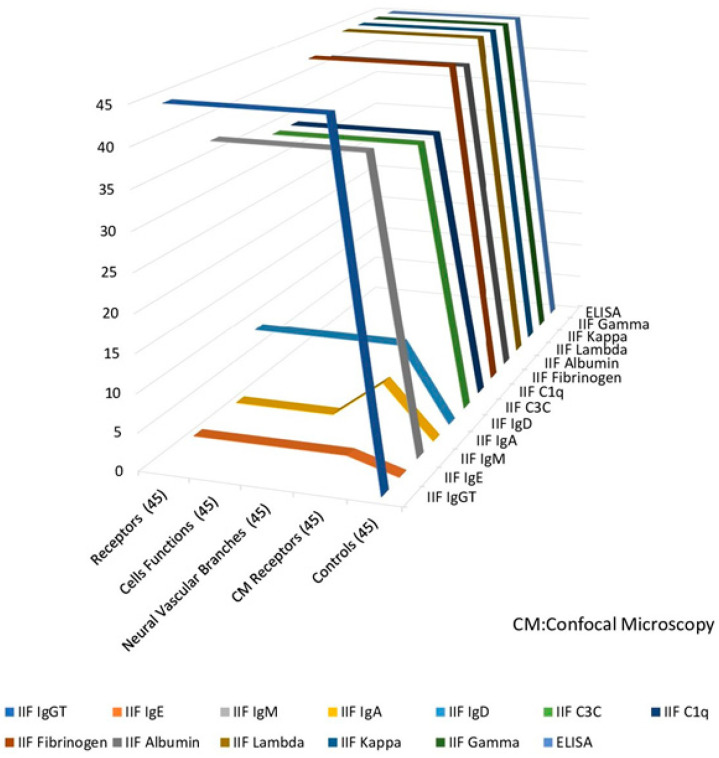 Figure 1
Figure 1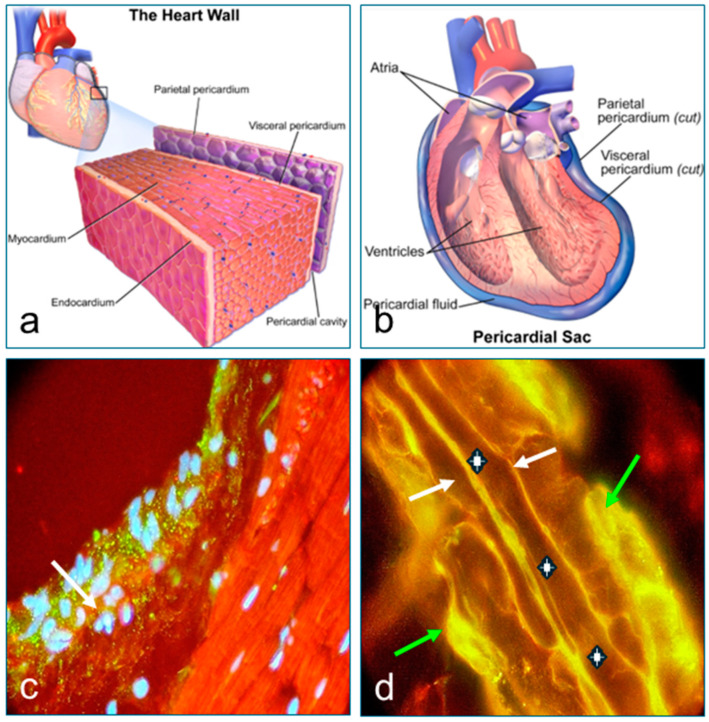 Figure 2
Figure 2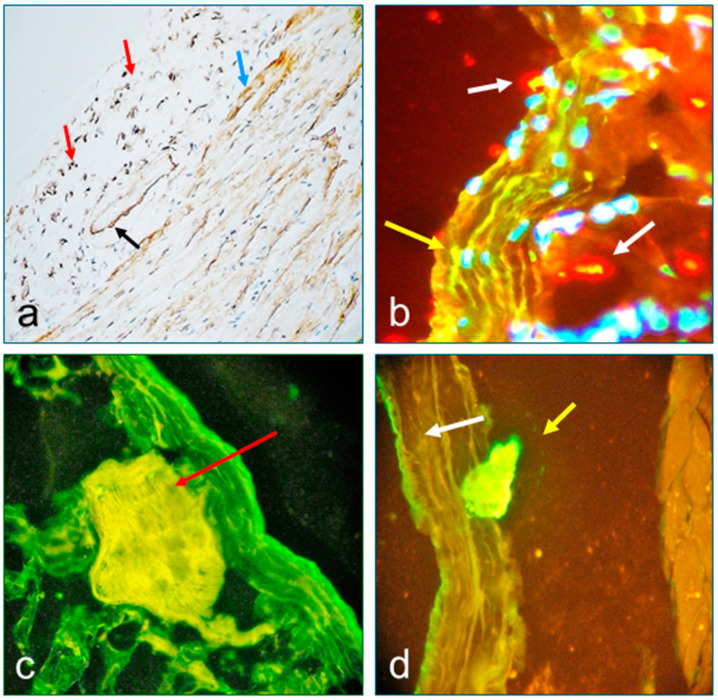 Figure 3
Figure 3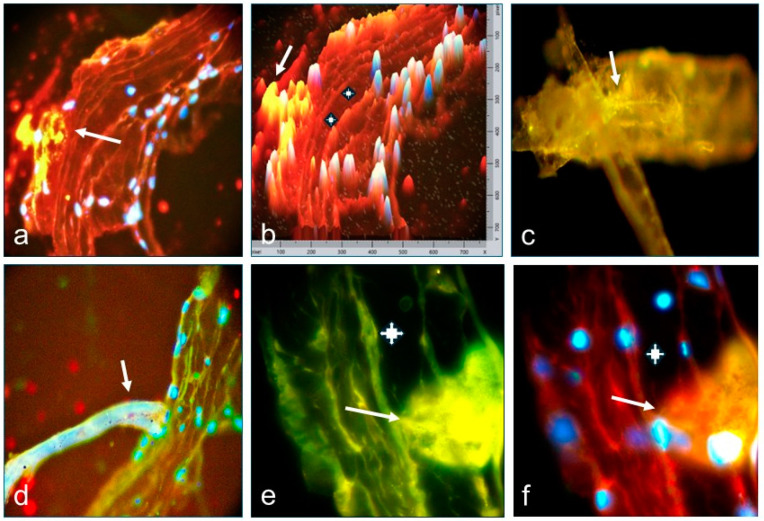 Figure 4
Figure 4- —Georgia Dermatopathology Associates
- —Mineros SA
- —Japan International Cooperation Office (JICA) Colombia Office
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAutoimmune Bullous Skin Diseases · Coagulation, Bradykinin, Polyphosphates, and Angioedema
1. Introduction
Endemic pemphigus foliaceus (EPF) or South American pemphigus foliaceus (A.K.A. Fogo Selvagem, wildfire) is an orphan autoimmune blistering disease, which is considered to be endemic in some areas in Brazil and central and south American countries [1,2,3,4,5]. The occurrence of EPF has also been reported in Africa, particularly in south Tunisia, which raises some concerns due to its apparent association with pregnancy and/or postpartum [5,6,7,8,9].
We identified a new variant EPF in El Bagre, a region of the State of Antioquia (Colombia, South America) and neighboring geographic areas bordering with other states. We denominated this variant as El Bagre-EPF (A.K.A. Pemphigus Abreu-Manu) and performed extensive research to characterize this disease [10,11,12,13].
It is currently accepted that EPF is an organ-specific skin disease. Nevertheless, accumulating evidence revealed systemic involvement in patients affected by both variants of EPF in Brazil (AKA fogo selvagem) and El Bagre-EPF [2,3,4,5,14,15,16]. In the El Bagre-EPF variant, the autoantibodies recognize various proteins, particularly, cell-junction proteins in the skin in frustre form (localized only in the seborrheic areas of the face and chest) and proteins in non-skin organs in the intermediate form between the frustre form and Senear–Usher-like systemic (resembles a mix of pemphigus and lupus) generalized form, affecting more than 70% of the skin. The systemic generalized form shows erythrodermic, bullous, exfoliative, and hyperkeratotic skin lesions, and also affects various endocrine glands, the cardiovascular system, muscles, kidneys, and other organs [10,11,12,13,16]. Furthermore, clinical evidence suggested that some chest organs are also affected in El Bagre-EPF patients. In fact, many patients show episodes of sudden chest pain, dyspnea, hiccups, dysphagia, palpitations, fatigue, anxiety, confusion, and syncope. Therefore, the present study was designed to investigate whether the pericardium and its neurovascular system are also targets for the autoantibodies in El Bagre-EPF patients and whether the autoantibodies of these patients are at the basis of the etiopathogenesis of the pericardial manifestations of the disease.
2. Materials and Methods
2.1. Patients
The study was approved by the Ethical Committee of the Hospital Nuestra Señora del Carmen, in El Bagre, Antioquia, Colombia, and it was conducted in agreement with the guidelines of the Declaration of Helsinki II. All participants signed informed consent. We examined 45 patients affected by El Bagre-EPF and 45 controls without known autoimmune diseases from the endemic area matched by age, gender, demographics, comorbidities, and work activities. No identifier was presented in the study, nor the data, from each patient, ensuring ethical research practices and building trust. This involves securing information, limiting access, and obtaining informed consent, with exceptions for legal or mandatory reporting. Investigators secure data storage: data, both electronic and physical, is being maintained securely in locked cabinets and with password-protected systems. Additionally, anonymization using alphanumeric codes instead of full names can protect participant identity. Only researchers have access to participant data and all investigators have and retain confidentiality protocols and data security measures. The study was conducted based on the data obtained from the clinical evaluation since no radiological study was available (see justification in the Discussion section).
2.2. Clinical Evaluation
Clinical examinations include the following signs and symptoms: pericardial rub on auscultation, PR depression, ST segment deviation, widespread ST-elevation and PR depression on electrocardiogram (ECG), occurrence of sharp piercing pain over the center or left side of the chest, which was generally more intense at breathing, shortness of breath when reclining, presence of heart palpitations, low-grade fever, an overall sense of weakness, fatigue or feeling sick, cough, and abdominal or leg swelling. For both the patients and controls, we used a nominal scale of positive (zero to five), being zero as no symptoms or no clinical findings, and five as the strongest symptoms. Only a few patients were examined by chest X-ray for an enlarged cardiac silhouette indicating pericardial effusion.
2.3. Histopathology (H&E Stain), Direct Immunofluorescence (DIF), Indirect Immunofluorescence (IIF), Confocal Microscopy (CM) and Immunohistochemical (IHC) Studies
Pericardial tissue samples were obtained from seven El Bagre-EPF patients and the matched controls at necropsies in the local hospital.
Because our previous studies showed that the sera of El Bagre-EPF patients also bind to the intracellular, intranuclear, cytosolic, and membrane-attached proteins, we prefixed the section of cow tissues on the slides with freshly prepared 3.5% paraformaldehyde, washed with phosphate-buffered saline (PBS), permeabilized the tissue by treating the slides with 0.1% Triton X-100 and 5% goat serum in PBS for 10 min. After further washing, the tissue sections were incubated with the patient’s serum for one hour, washed with PBS again, and incubated with the secondary antibody for 1.5 h. For detailed methods see Supplementary Materials. Detailed methods for histopathology (H&E stain), DIF, IIF, CM, and IHC are also described in Supplementary Materials. Table 1 shows the catalog numbers and used dilutions for the antibodies in the IHC study, with IHC stain strength (highest +++ to lowest −), according to the method reported by McCarty et al. [17].
2.4. Statistical Analysis
We used the Fisher exact test to compare two nominal variables (e.g., positive and negative) of antibody response. p < 0.05 with a 95% confidence or more was considered statistically significant. We used the software GraphPad QuickCalcs (version 9.1, GraphPad Software Inc., La Jolla, CA, USA). Additionally, we used autoantibodies in the diagnosis of El Bagre-EPF by assessing using the Chi-square test, and it was found to be statistically significant with a p value ≤ 0.05 (Table 2 and Table 3).
3. Results
3.1. Clinical Symptoms of the El Bagre-EPF Patients
Although the differences in clinical symptoms between the patients and controls were subtle, as demonstrated in Table 2, the patients of El Bagre-EPF predominantly showed episodes of sudden chest pain, dyspnea, hiccups, dysphagia, palpitations, fatigue, anxiety, confusion, hoarseness, and syncope without respiratory infections. One patient had active tuberculosis, which was treated. Active tuberculosis was not seen in the controls. The most common clinical symptom was sharp piercing chest pain over the center of the chest, especially painful when breathing. This was observed in 33/45 patients, and, using the Chi-square test, was found to be statistically significant with a p value ≤ 0.05.
3.2. Results of Immunohistochemistry for Patient Tissues (IHC)
IHC studies showed heterogeneous and polyclonal reactivities in tissue samples from El Bagre-EPF patients and labeled epi-pericardial tissues, both blood and lymphatic vessels, nerves, and pericardial sensory nerve formations. No positive immunoreactivity was detected in disease-free control cadaveric necropsies (Table 1). Strong immunoreactivity in IHC studies was observed by using specific antibodies against human fibrinogen (7/7), kappa chain (7/7), lambda chain (7/7), human albumin (7/7), human IgG (6/7), IgM (6/7), human complement/C3c (5/7), human complement/C3d (5/7), C5b-9 complement (5/7), human IgD (4/7), human C1q (4/7), human IgA (0/7), and human IgE (0/7) in El Bagre-EPF patients. (p < 0.1).
Of interest, most of the patients presented with autoantibodies in a polyclonal way to both the cell junctions as well as those to the neural receptors. This was observed in 42/45 patients, and, using the Chi-square test, was found to be statistically significant with a p value ≤ 0.05.
3.3. Results of Immunofluorescence Tests (DIF and IIF) and Confocal Microscopy (CM)
The results of IIF and CM on cow’s epi-pericardial as antigen source are shown in Supplementary Materials. In both IIF and CM microscopy studies on El Bagre-EPF patients, positive reactivities with epi-pericardial tissues were seen by utilizing antibodies against human fibrinogen (43/45), kappa chain (45/45), lambda chain (45/45), human albumin (42/45), human IgG (43/45), IgM (42/45), human complement C3c (38/45), IgD (25/45), C1q (35/45), IgA (0/45), and IgE (1/45) (p < 0.1). None of the control cadaveric necropsies showed positive reactivity.
In Figure 1, we present a summarized graphic representation of the results of the positive reactivity of each antibody with the epicardium, pericardium, the respective nerve profiles, and associated sensory nerve formations, as well as neurovascular bundles. These antibodies included those against total IgG (IgG T), IgM, IgD, kappa chain, gamma chain, C3c of the complement, C1q, fibrinogen, and albumin (p < 0.1). None of the patients were positive for the layers of the pericardium, the neurovascular branches, or the sensory nerve formations for these antibodies (p < 0.1).
In Figure 2, Figure 3 and Figure 4, we present the results of the commercial antibodies directed to MIZAP, ARVCF, desmoplakin I-II, and p0071, which were perfectly colocalized those with the autoantibodies to El Bagre-EPF autoantibodies, i.e., the membrane receptors were positive in the epicardium, the pericardium, the neurovascular bundles feeding, and their respective cells junctions (p < 0.1).
4. Discussion
The present study was designed to analyze whether the pericardium of El Bagre-EPF patients is a target for the autoantibodies of these patients since they usually present thoracic symptoms. Although the clinical manifestations of the disease El Bagre-EPF are primarily cutaneous lesions, it has been shown that it can also affect other organs, including the cardiovascular system [10,11,12,13]. In the present study, we found that El Bagre-EPF autoantibodies bind to the pericardium (both fibrous and serous), the pericardial vessels and nerves, and structures resembling sensory nerve formations reported in the pericardium of dogs [18,19], which are mechanoreceptors or chemoreceptors [20,21]. Our patient autoantibodies colocalized 100% with the illegally commercialized Progen antibodies, as documented above in methods.
The pericardium is a double-walled membrane (fibrous and serous) that envelops the heart and the origin of the great blood vessels. The fibrous pericardium is a thin membrane that consists of connective tissue cells, large collagen bundles, and elastic fibers and contains abundant vessels and nerves [22,23,24]. On the other side, the serous pericardium is formed by two layers. The inner membrane or epicardium covers the surface of the myocardium and consists of a layer of flattened mesothelial cells [25], while the outer membrane covers the inner surface of the fibrous pericardium, which is formed by a plane layer of mesothelial cells. Both layers of the serous pericardium limit a virtual pericardial space filled with liquid [25].
To understand the involvement of the pericardium in El Bagre-EPF, it is necessary to explain its structure. The mesothelial pericardial cells have microvilli and scarce cilia in the luminal surface [25] and show numerous junctional cell membrane complexes in the skin (i.e., gap junctions, desmosomes, adherens, and tight junctions) whose structural proteins are targets for El Bagre-EPF autoantibodies [10,11,12,13,16,26]. The results of the present study for the pericardium strongly support that junction cell proteins are targets for El Bagre-EPF autoantibodies independently of their localization in the pericardium. Mesothelial cells in the peritoneum can produce and secrete mixed molecules in response to exterior signals, that regulate inflammatory responses, recruit immune cells into serosal cavities, and present antigens to specialized T cells [27]. They also play a role in removing fibrin from the serosal cavities [26]. Both fibrinogen and albumin are regarded as protectors of tissue damage, independent of the nature of the tissular lesion origin or alteration on those compounds [28]; in addition to cell-junction membrane proteins, further affinity chromatography studies using albumin and or fibrinogen and testing the patient’s sera will be required to study their role in El Bagre-EPF pathogenesis. Due to the lack of examinations by specialized MRI and echocardiogram, only the clinical symptoms, signs, EKG, and chest X-ray for a few cases were examined, which showed a slight positivity to pericardial disease in the patients (Table 3). The small hospital in the endemic area often has an unworking X-ray machine and does not have an echocardiogram or magnetic resonance imager (MRI). In addition, health insurance does not approve of sending patients to cities with those resources.
In general, pericardial heart disease is observed more frequently at necropsy than in live patients [29,30]. Indeed, older literature mentioned that pericarditis is an inflammation of the pericardium. Dr. Pierre Louis Alphée Cazenave, who described pemphigus foliaceus for the first time [31], reported in his seminal book that multiple patients who died before or around the time when corticosteroids were just beginning to be used for pemphigus and pemphigoids. In the same book, in many patients with pemphigus, necropsies presented with serositis, peritonitis, and pericarditis, and also showed the presence of granulation tissue, resembling chronic inflammation, around most of the serous layers in several organs [31]. He also detected multiple old adherences in several organs covered by serous membranes and diaphragm [31]. Similar findings were described by others [32]. Indeed, before the use of corticosteroids for autoimmune skin blistering diseases, serosites, such as pericarditis, pleuritis, and peritonitis, were described in patients with pemphigus vulgaris and dermatitis herpetiformis. Again, most of these findings were shown in post-mortem [31,32,33,34]. Our findings suggest that autoreactivity to endocardial and pericardial components causes pericarditis, which was detected in a few patients with chronic uncontrolled disease, as well as in the necropsies.
Thus, based on our IHC findings, El Bagre-EPF patients may undergo clinical or subclinical pericarditis, as well as symptoms and signs, before and around the implementation of corticosteroids as treatment [31,32,33,34].
Our finding reinforces previous studies indicating that autoantibodies of the El Bagre-EPF patients recognize cell junction proteins present in the endoneurial, perineurial, and epineural sites of the nerves. In the present study, we also demonstrated that encapsulated formations in the sensory nerve formations have some type of small cell junctions recognized by the patient autoantibodies. Indeed, other authors have previously shown the presence of Ruffini-like corpuscles (RLCs) in all pericardia and allocated to three histologic sensory nerve formations depending on the fibrous pericardium layering in precise anatomical sites [35].
The use of paraformaldehyde in our studies as a crosslinker fixative helped to cross-link cell membranes and cytoplasmic proteins [36]. The simultaneous use of Triton X-100 (C_14_H_22_O(C_2_H_4_O)n), a nonionic surfactant (detergent), is useful to solubilize and separate biomembrane components, especially to separate underlying detergent–lipid interactions and “open pores” on the cells membranes, that are bilayers composed mostly of lipids [36]. We noticed that this combination of paraformaldehyde, Triton X-100, and blocking agents, such as goat serum (all very timely, and temperature controlled), is excellent for exposing epitopes on unknown lipid-proteins, which may be glycosylated and phosphorylated and may have other possible conformational posttranscriptional modifications. Detergents interact with biomembranes (cell junction molecules in our study) due to their amphiphilic character to intercalate between lipids [37].
Nevertheless, caution is needed in drawing conclusions from our findings, as they are based solely on clinical findings (and not always complete), and the results of immunofluorescence tests and IHC. One main limitation of our study is the absence of various clinical tests, particularly radiological tests. These tests, except with the chest X-ray (when the machine is working), are not available in the very rural area of El Bagre. Furthermore, the Colombian Health Promoting Entity healthcare system has been broken for years and rarely accepts admissions to hospitals for people in severe poverty.
On the other hand, fibrinogen deposits are a hallmark of tissue damage, despite the triggering nature of such wounds, insults, or infections (by any microorganism and or virus), as well as by immunological causes [28]. Fibrin can curb the properties of an inflammatory response, including attracting leukocytes from the bloodstream [28,38,39]. Therefore, we may hypothesize that the presence of albumin and fibrinogen may play roles as transporters and initial blockers, which try to protect the damaged structures.
5. Conclusions
For the first time in the world literature, we found that ARVCF, MYZAP, desmoplakin, and p0071 are present in the complex perineurium, its membrane, and sensory nerve formations, which are also reacted by the patients’ autoantibodies. Our use of the partial permeabilization of membranes and the use of detergents allowed us to discover these findings. Pericarditis is usually a postmortem diagnosis. At this point, we do not have answers to the functional and/or pathological effects of the autoantibodies on the membrane and chemoreceptors in the pericardium and to any clinical symptoms in the patients. Our study greatly improves the understanding of the field of the pleura and provides a new set of antibodies to study the pericardium and its sensory nerve formations. Material Transfer Agreements should always be signed between researchers, independent of the “trust” between the parties when handling biological materials.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Aguiar Pupo J. Aspectos originais do Pênfigo Foliáceo no Brasil An. Bras. Dermatol.19714653604942105 · pubmed ↗
- 2Aranha Campos J. Pênfigo Foliáceo (Fogo Selvagem): Aspectos Clínicos e Epidemiológicos Melhoramentos São Paulo, Brazil 1942126
- 3Aranha Campos J. Novas observações de casos familiares de pênfigo foliáceo An. Paul. Med. Cirurg.19455073
- 4Heimgartner E. de Heimgartner V. Experiencias en enfermedades dermatológicas endémicas en la selva peruana: Leishmaniasis y pénfigo foliáceo endémico Med. Cut. ILA 1976116135891 · pubmed ↗
- 5Ramos W. Rojas N. Ortega-Loayza A.G. Tello M. Jiménez G. Cuba-Cáceres N. Ronceros G. De La Cruz-Vargas J.A. Vera-Ponce V.J. Guerrero N. Ultrastructural skin alterations of healthy subjects with anti-desmoglein 1 antibodies in endemic areas to pemphigus foliaceus: A case series J. Transl. Autoimmun.2023710020810.1016/j.jtauto.2023.10020837520889 PMC 10372304 · doi ↗ · pubmed ↗
- 6Morini J.P. Jomaa B. Gorgi Y. Saguem M.H. Nouira R. Roujeau J.C. Revuz J. Pemphigus foliaceus in young women. An endemic focus in the Sousse area of Tunisia Arch. Dermatol.1993129697310.1001/archderm.1993.016802200810198420494 · doi ↗ · pubmed ↗
- 7Jerbi A. Hachicha H. Bahloul E. Feki S. Sellami K. Abida O. Bouzid A. Turki H. Masmoudi A. Masmoudi H. South Tunisian pemphigus patients beyond 60 years: Epidemiological profile and evolution Int. J. Dermatol.201958 e 219e 22010.1111/ijd.1459431334831 · doi ↗ · pubmed ↗
- 8Denguezli M. Ben Nejma B. Nouira R. Korbi S. Bardi R. Ayed K. La dermatose bulleuse à Ig A linéaire de l’enfant. Une série de 12 malades tunisiens [Iga linear bullous dermatosis in children. A series of 12 Tunisian patients]Ann. Dermatol. Venereol.19941218888927632006 · pubmed ↗