Low Vitamin K Status and Risk of Chronic Obstructive Pulmonary Disease
Daniel Alexander Ackermann, Allan Linneberg, Ema Rastoder, Anna Kubel Vognsen, Anne Ahrendt Bjerregaard, Lennart Friis-Hansen, Niklas Rye Jørgensen, Caroline Emma Hedsund, Niklas Dyrby Johansen, Daniel Modin, Maria Dons, Mats C. Højbjerg Lassen, Kristoffer Grundtvig Skaarup

TL;DR
Low vitamin K levels are linked to a higher risk of COPD, but not to its severity or mortality.
Contribution
This study identifies a novel association between low vitamin K status and COPD risk.
Findings
Low vitamin K status was associated with a 9.7-fold higher odds of having COPD.
No significant associations were found between low vitamin K and COPD severity or mortality.
Vitamin K status was not linked to smoking exposure in COPD patients.
Abstract
Background: Vitamin K is a cofactor necessary for the biological activity of proteins like Matrix Gla Protein (MGP), which reduce calcification and help preserve lung function. This study aims to determine, first, whether low vitamin K status is associated with chronic obstructive pulmonary disease (COPD), and secondary, whether the level of vitamin K is associated with COPD severity, smoking exposure, or mortality. Methods: The plasma concentration of dephosphorylated uncarboxylated (dp-uc) MGP was used as an inverse biomarker for vitamin K in 98 COPD patients from the CODEX-P COPD study and 986 controls from the DanFunD study. Low vitamin K status was defined as the upper quartile of dp-ucMGP (>589 pmol/L). Using a logistic regression model, we examined whether low vs. high/moderate vitamin K status increased the odds ratio (OR) of having COPD. Secondary analyses, in the COPD cohort…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
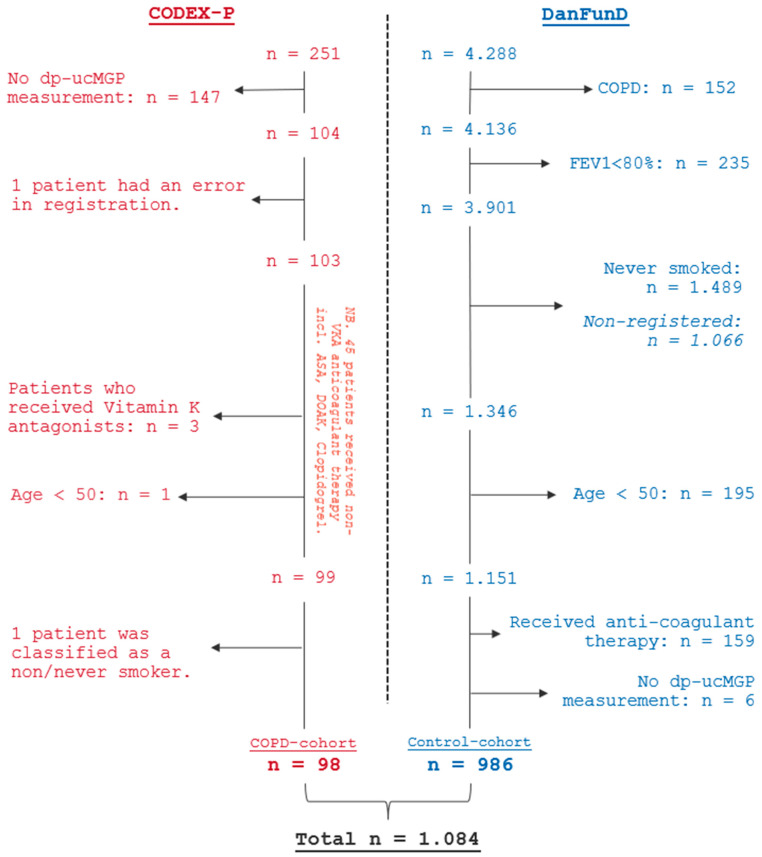 Figure 1
Figure 1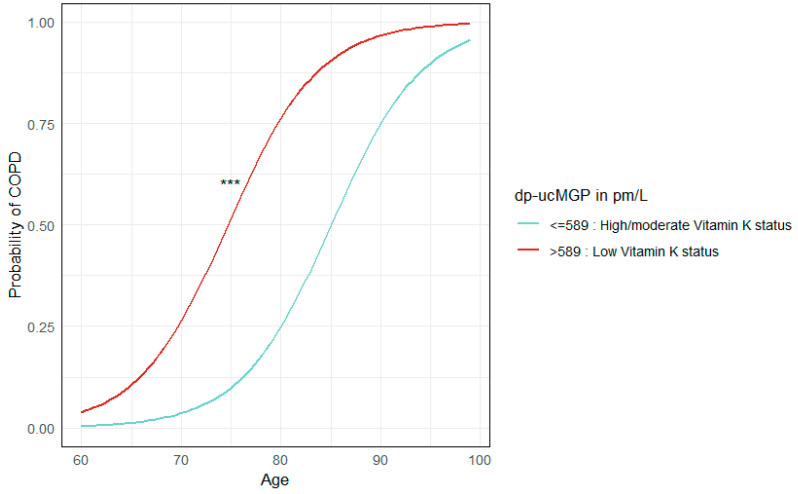 Figure 2
Figure 2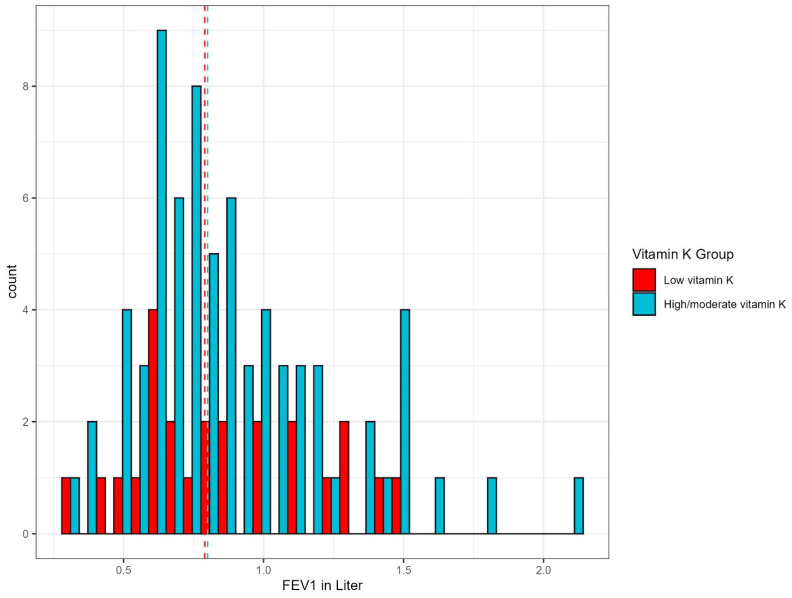 Figure 3
Figure 3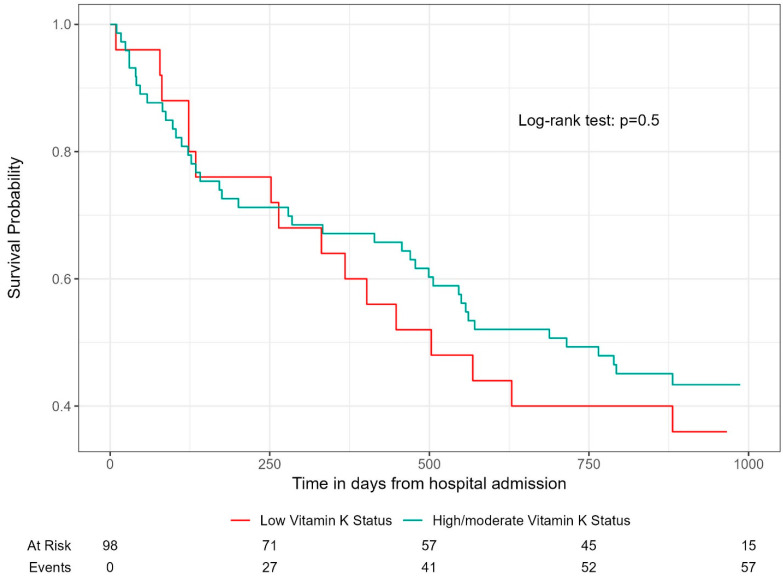 Figure 4
Figure 4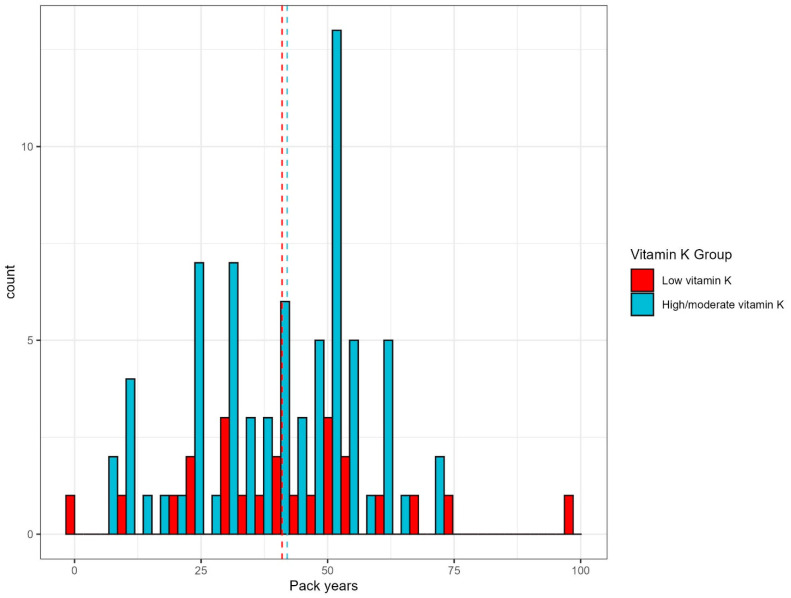 Figure 5
Figure 5- —Herlev Gentofte Hospital Research Funds 2024
- —Novo Nordisk Foundation
- —The Lundbeck Foundation
- —The Tryg foundation
- —Helsefonden
- —The Marilyn Brachman Hoffman Foundation
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsVitamin K Research Studies · Renal function and acid-base balance
1. Introduction
Chronic obstructive pulmonary disease (COPD) is a leading cause of morbidity and mortality with 600 million cases expected by 2050. An urgent need for improved preventive and therapeutic strategies such as reliable biomarkers that are able to predict disease progression is of great need [1,2].
Recent studies have highlighted vitamin K as a possible factor in preventing cardiovascular and respiratory diseases [3] by activating the vitamin K-dependent protein Matrix Gla Protein (MGP).
MGP plays a significant role in inhibiting soft-tissue calcification and elastin degradation, which is crucial in preventing lung tissue calcification. Measuring MGP in its inactive form as dephosphorylated uncarboxylated Matrix Gla Protein (dp-ucMGP) can provide insights into the body’s vitamin K status as it serves as an inverse biomarker of vitamin K levels in peripheral tissues [4].
In COPD, vascular calcification and elastin degradation is accelerated contributing to disease pathogenesis. Therefore, it has been hypothesized, through the “Vitamin K deficit and elastolysis theory”, that lower vitamin K, a deficit, could worsen elastin degradation, implying that vitamin K status could be of importance in preventing pulmonary disease progression [5,6].
Emerging research suggests vitamin K may play a role in managing diseases like COPD, though no direct link has been established. Cohort studies have associated low vitamin K with COPD and elastin degradation, indicating its potential importance in pulmonary pathogenesis [7,8]. A large study in the Danish general population found reduced lung function and a higher risk of self-reported COPD in individuals with low vitamin K levels [4]. Furthermore, low vitamin K status has been linked to increased elastin degradation and higher mortality in COPD patients [7]. While these studies have provided important insights, further research not only exploring the role of vitamin K in elastin degradation but also its impact on disease progression, lung function, and long-term survival in larger and diverse patient populations are of need.
This study aims to determine the association between low vitamin K and spirometry-verified COPD compared to a healthy population and test the impact of vitamin K status on COPD severity and mortality.
We hypothesize that individuals with low vitamin K status (upper quartile dp-ucMGP) have higher odds of having COPD compared to a healthy control population and that low vitamin K status is associated with lower lung function and increased all-cause mortality.
2. Material and Methods
This is an observational cohort study of a COPD cohort and a healthy control cohort. The COPD cohort derives from the Danish CODEX-P study (“COPD exacerbation and Pulmonary Hypertension”, clinicaltrials.gov: NCT04538976)—a prospective study between 2020 and 2022 comparing transthoracic echocardiographic parameters during hospital-requiring COPD exacerbation and the stable phase. The control group was included from the DanFunD study (“The Danish Study of Functional Disorders”)—a longitudinal population-based study investigating the prevalence of functional disorders or medically unexplained illnesses in the general population. The data was derived from the 5-year follow-up, performed between 2017 and 2020 at the Center for Clinical Research and Prevention and consisted of parameters from both questionnaires and physical examinations [4].
2.1. Outcome
The primary outcome is spirometry-verified COPD. Secondary outcomes, only in the COPD cohort, included FEV_1_ as well as all-cause mortality within 3 years.
2.2. Study Participants and Sample Size
The COPD cohort consisted of patients with a registered diagnosis of COPD (ICD-10: DJ44), who were active or former smokers and had available vitamin K biomarker data (dp-ucMGP). Participants under 50, those with coagulation disorders or receiving vitamin K antagonists, and those with significant bleeding or surgery within 3 months were excluded.
The control cohort comprised participants who were current or ever smokers with available vitamin K data. Exclusions included those under 50, individuals with self-reported COPD or FEV_1_ < 80%, and those using blood-thinners, to avoid including vitamin K antagonist users.
2.3. Measurement of dp-ucMGP Plasma Levels
dp-ucMGP was measured using IDS-iSYS InaKtif MGP ECLIA assay (ImmunoDiagnostic Systems Holdings PLC, East Boldon, UK). Preanalytical sampling and analysis were performed according to manufacturer’s instructions. The intermediary precision was <10%. All dp-ucMGP values below the lower limit of quantitation (300 pmol/L) were set to 299 pmol/L, to determine status with suitable precision and accuracy according to assay instructions [9].
In the control cohort, analysis of dp-ucMGP was performed continuously during data collection when approximately 200 samples had been collected; thus, duration of storage ranged between 0 and 3 months [4]. In the COPD cohort, blood samples were collected at the date of hospitalization due to acute exacerbation of COPD. Analysis of dp-ucMGP was performed in all available samples in April 2023. Average time of −80 °C freezer storage was mean 1.25 years, for which the dp-ucMGP was shown to be stable [10].
2.4. Vitamin K Classification
Vitamin K status was categorized using quartile ranges. The upper 4th quartile of dp-ucMGP levels was defined as “Low vitamin K” status, and levels of dp-ucMGP in the 1st, 2nd, or 3rd quartile were defined as “High/moderate vitamin K” status. See Appendix A Table A1 and Table A2 for more details regarding cut-off levels for dp-ucMGP used in the main and secondary analyses.
2.5. Lung Function Measurement
Data on spirometry were collected from the patients’ electronic medical records up to three years prior to inclusion in the COPD cohort. If unavailable, spirometry results during the exacerbation were used. Spirometry in the control cohort was performed according to standards of the protocol described by Jespersen, et al. [4].
2.6. Statistical Analyses
Descriptive analysis of demographic and clinical characteristics of the study participants was conducted. Categorial variables are presented as counts and percentages, while continuous variables are presented as mean and standard deviation (SD) if normally distributed. Non-normally distributed variables are presented as median and interquartile ranges (IQRs).
2.7. Primary Analysis
The complete cohort was divided into two groups: high/moderate vitamin K or low vitamin K—based on quartile levels of dp-ucMGP in pmol/L (see Appendix A Table A1). A logistic regression was performed to investigate a possible association between low vitamin K status and probability of COPD. The exponential of the model parameters produced the odds ratio (OR). The p-value and confidence interval (CI) of the given estimates were assessed. The analysis was adjusted for sex, age, and body mass index (BMI). To evaluate whether kidney function would impact the association between vitamin K status and COPD, adjustments for the estimated glomerular filtration rate (eGFR) and creatinine were included as sensitivity analyses.
A visualization of the probability of COPD stratified by vitamin K status was performed using a logistical regression curve.
2.8. Secondary Analyses
Secondary statistical analyses were performed in only the COPD cohort to examine the association between low vitamin K status and COPD severity, measured as FEV_1_. New dp-ucMGP quartiles were defined only from participants with COPD and were then divided into low or high/moderate vitamin K status (see Appendix A Table A2). A histogram was made to visualize the distribution of lung function in FEV_1_ stratified by vitamin K status. If the groups had same variance, a standard t-test was performed—otherwise, a Welch Two-Sample t-test was performed. Additionally, the same analyses, a histogram and a Welch Two-Sample t-test, were used to determine whether smoking exposure in packyears in the COPD cohort had any significant association with levels of vitamin K (see Appendix A Figure A1). A single packyear was defined as smoking 20 cigarettes a day for a year.
To examine if low vitamin K status and all-cause mortality in the COPD cohort were associated, a Kaplan–Meier curve was fitted. Date of hospital admission was used as start of observation, while the end of observation was set to 30 September 2024. Events was defined as all-cause mortality within this period and were collected from the patients’ electronic medical records. A log-rank test was performed to examine significance.
2.9. Data Analysis
All analyses and illustrations were performed using “RStudio”, R version 4.4.1 (14 June 2024 ucrt)—“Race for Your Life”. Copyright © 2024. The R Foundation for Statistical Computing. Platform: ×86_64-w64-mingw32/×64. We considered a p-value ≤ 0.05 as statistically significant.
3. Results
The flowchart (Figure 1) visualizes the selection of study participants to the COPD cohort and control cohort. In total, 1084 participants were included: 98 in the COPD cohort and 986 in the control cohort.
The COPD cohort consists of 65.3% female participants, while the control population has 56.9%, with a mean age difference of approximately 10 years (COPD: 74 [8.1], Control: 63 [7.5]). The COPD cohort has lower lung function compared to the control population with a mean (SD) FEV_1_ of 39.96% (16.29) and 101.54% (12.26), respectively. Weekly alcohol use is higher in the COPD cohort (15.87 [17.86] though 84 had missing data) compared to the control population (9.28 [7.92], 32 has missing data), and more participants among the COPD cohort are also active smokers, 33.7% compared to 17.7% in the control population. The majority of participants in the control population have a high/moderate vitamin K status (80.2%), while 19.8% has a low vitamin K status. The median dp-ucMGP level is 485 pmol/L, IQR (409, 570). In the COPD cohort, the median dp-ucMGP level is 734 pmol/L, IQR (591.5, 1.065.5), and 75.5% of participants have a low vitamin K status. (See Table 1)
3.1. Odds Ratio of COPD in Low Vitamin K Group
We found an increased odds of having COPD among participants with low vitamin K status compared to those with high/moderate status with an OR of 9.4 (95% CI: 5.4–17.0), p < 0.001, (See Table 2) when adjusted for sex, age, and BMI. Two observations were deleted due to missing values of BMI in the COPD cohort. Sensitivity analysis adjusting for creatinine and eGFR separately did not change the association (p > 0.05).
The probability of COPD according to vitamin K status, stratified by age, was visualized using a logistic regression curve (See Figure 2).
3.2. Association with Low Vitamin K and COPD Severity and Mortality
Figure 3 visualizes the distribution of lung function measures by FEV_1_ (liter), to approximate COPD severity, stratified by vitamin K status.
A total of 28 participants had no previous lung function measurements in the stable phase prior to inclusion in CODEX-P, and three had no lung function data at all.
There was a difference in variance, with overlapping confidence intervals: the median FEV_1_ for the COPD group with low vitamin K status (dp-ucMGP > 1065.5 pmol/L) was 0.79 L, and 0.8 L for those with high/moderate vitamin levels. Using a Welch Two-Sample t-test there was no association between low vitamin K status and the severity of COPD est. −0.03 (p = 0.7; CI: [−0.2:0.1]).
Using a Welch Two-Sample t-test, we found no significant association between low vitamin K status and smoking exposure measured in pack-years est. 0.50 (p = 0.6; CI: [−7.5:12.4]). A visualization of the distribution of smoking exposure measured in packyears stratified by vitamin K status can be found in Appendix A Figure A1.
The Kaplan–Meier plot depicting the association between low vitamin K status and all-cause mortality in the COPD cohort showed no statistical difference between low and high/moderate vitamin K status and all-cause mortality (log-rank test p = 0.5). See Figure 4.
Since there was no violation of proportional hazards when using cox regression, p = 0.6, a standard log rank test was deemed sufficient. After the end of observation (30 September 2024), 57 patients were deceased, while 15 were still at risk. The mean time to death was 607 days.
4. Discussion
This study found that low vitamin K status was associated with higher odds of having COPD compared to high/moderate vitamin K status. However, no significant association was found between low vitamin K status and COPD severity or all-cause mortality.
These findings align with previous studies [4,7], although Jespersen et al. found an association between low vitamin K status and reduced ventilatory capacity in the general population, which differs from our findings using spirometry-verified COPD [4]. Our findings correlate with those from Piscaer et al. who found an association between vitamin K status and COPD, and even proposed a biological mechanism of the association in the form of increased elastin degradation due to vitamin K deficiency [7,11].
Regarding the potential directionality of the association between low vitamin K status and COPD, our study suggests that low vitamin K may be a contributing factor to the development of COPD rather than a consequence of the disease itself. The higher odds of COPD in individuals with low vitamin K status and the significantly greater proportion of low vitamin K status among COPD patients support this hypothesis. However, as our study is observational, we acknowledge that interventional studies are needed to fully determine whether low vitamin K status is a predisposing factor for COPD or whether COPD leads to vitamin K deficiency.
We found no associations between vitamin K status and COPD severity, consistent with previous findings [7]. However, we did not collect data on diffusing capacity for carbon monoxide nor data on the degree of emphysema, which may provide valuable insights into the association between vitamin K status and COPD severity. It is important to note that, once COPD is established, other factors such as airway inflammation, oxidative stress, and structural lung changes (e.g., emphysema) may become more influential in disease progression. It is possible that the effects of vitamin K on elastin degradation and vascular health are more prominent in the early stages of the disease, whereas, in more advanced stages, the overall disease burden may overshadow the impact of vitamin K status on disease severity.
We also observed no difference in mortality, which is in contrast with findings by Piscaer et al. who found an association between low vitamin K and 5-year mortality [7]. We cannot exclude that longer observation time in our study would have resulted in an increased mortality risk. Further, our study was a post-analysis and not powered for the secondary analyses.
Strengths of our study include the use of a well-defined cohort with spirometry-verified COPD, providing reliable data on disease presence and severity. Additionally, vitamin K status was objectively measured using dp-ucMGP, ensuring precise biomarker data. Finally, this study’s combination of a healthy control group and a large COPD cohort allows for an evaluation of the role of vitamin K in disease development and progression in a realistic clinical context.
Our study specifically examines low vitamin K status and the odds of having COPD in a large control cohort of healthy individuals and a case–cohort diagnosed with severe spirometry-verified COPD. Though we found similar results concordant with previous studies [4,7], following limitations, interactions and possible confounding effects need to be addressed.
First, vitamin K is largely dependent on diet, and individuals with malabsorption disorders are at higher risk of deficiency [12]. Around one in three inpatients and one in five outpatients with COPD are at risk of malnutrition, which worsens after exacerbations [13,14]. However, in the COPD cohort, nearly 75% had low vitamin K status, yet none had known gastrointestinal disorders. Second, the COPD cohort’s average alcohol intake was higher than controls. Excessive alcohol can lead to vitamin K deficiency by disrupting nutrient absorption, potentially affecting our findings [15,16,17,18]. Unfortunately, we were not able to adjust for alcohol intake due to missing data. Third, all COPD participants were hospitalized due to AECOPD and received antibiotics, before vitamin K assessment. Critical illness and antibiotics use may lead to vitamin K deficiency by disrupting gut bacteria and affecting nutrient absorption. These factors, along with inadequate diet and increased metabolic demands, may have influenced vitamin K uptake [19]. Fourth, samples from the COPD cohort had been stored for about a year longer than controls, which may have led to the underestimation of vitamin K differences due to potential degradation.
Perspective
Vitamin K measurements in COPD patients are currently not of use clinically, but confirming their diagnostic value and role in risk assessment may be beneficial. Randomized trials on vitamin K supplementation could reveal its impact on COPD management, enabling tailored treatments or aiding early detection in high-risk individuals.
5. Conclusions
In this observational study, we found a marked increase in odds of having COPD in participants with a low vitamin K status. No association was found between low vitamin K status and COPD severity, as measured by FEV_1_, or all-cause mortality.
Our results indicate that vitamin K may be of importance as a biomarker of COPD in high-risk patients. Clinical trials are needed to establish a clear causal relationship and to confirm the potential therapeutic role of vitamin K in COPD, especially in reducing pulmonary calcification, inflammation, or improving overall outcomes.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Boers E. Barrett M. Su J.G. Benjafield A.V. Sinha S. Kaye L. Zar J.H. Vuong V. Tellez D. Gondalia R. Global burden of chronic obstructive pulmonary disease through 2050 JAMA Netw. Open 20236 e 234659810.1001/jamanetworkopen.2023.4659838060225 PMC 10704283 · doi ↗ · pubmed ↗
- 2Safiri S. Carson-Chahhoud K. Noori M. Nejadghaderi S.A. Sullman M.J.M. Heris A.J. Ansarin K. Mansournia M.A. Collins G.S. Kolahi A.A. Burden of chronic obstructive pulmonary disease and its attributable risk factors in 204 countries and territories, 1990–2019: Results from the Global Burden of Disease Study 2019 BMJ 2022378 e 06967910.1136/bmj-2021-06967935896191 PMC 9326843 · doi ↗ · pubmed ↗
- 3Kampmann F.B. Thysen S.M. Nielsen C.F.B. Kofoed K.F. Køber L. Pham M.H.C. Vaag A. Jørgensen N.R. Petersen J. Jacbosen R.K. Study protocol of the Inter Vitamin K trial: A Danish population-based randomised double-blinded placebo-controlled trial of the effects of vitamin K (menaquinone-7) supplementation on cardiovascular, metabolic and bone health BMJ Open 202313 e 07188510.1136/bmjopen-2023-07188537208133 PMC 10201225 · doi ↗ · pubmed ↗
- 4Jespersen T. Kampmann F.B. Dantoft T.M. Jørgensen N.R. Kårhus L.L. Madsen F. Linneberg A. Thysen S.M. The association of vitamin K status with lung function and disease in a general population ERJ Open Res.2023900208-202310.1183/23120541.00208-202337588689 PMC 10423920 · doi ↗ · pubmed ↗
- 5Mecham R.P. Elastin in lung development and disease pathogenesis Matrix Biol.2018736202933133710.1016/j.matbio.2018.01.005PMC 6041195 · doi ↗ · pubmed ↗
- 6Janssen R. Vermeer C. Vitamin K deficit and elastolysis theory in pulmonary elasto-degenerative diseases Med. Hypotheses 2017108384110.1016/j.mehy.2017.07.02929055397 · doi ↗ · pubmed ↗
- 7Piscaer I. van den Ouweland J.M.W. Vermeersch K. Reynaert N.L. Franssen F.M.E. Keene S. Wouters E.F.M. Janssens W. Vermeer C. Janssen R. Low Vitamin K status is associated with increased elastin degradation in chronic obstructive pulmonary disease J. Clin. Med.20198111610.3390/jcm 808111631357639 PMC 6724066 · doi ↗ · pubmed ↗
- 8De Brouwer B. Spanbroek M. Drummen N. Van Den Ouweland J. Zanen P. Vermeer C. Janssen R. Low Vitamin K status is associated with COPD and accelerated degradation of mature elastin Am. Thorac. Soc.2016193 A 4134