A Case of Adult-Onset Atypical Teratoid/Rhabdoid Tumor With Extracranial Metastasis
Kengo Hirayama, Hirofumi Oyama, Kenichi Wakabayashi

TL;DR
A 47-year-old woman was diagnosed with a rare adult-onset atypical teratoid/rhabdoid tumor that spread to the lungs and spine, highlighting the challenges in treating this condition in adults.
Contribution
This paper reports a rare case of adult-onset atypical teratoid/rhabdoid tumor with extracranial metastasis to aid in understanding and treating this condition.
Findings
The tumor was diagnosed in the sellar region and showed rapid growth despite chemotherapy.
The patient developed metastases in the brain, spinal cord, and lungs, and treatment was ineffective.
Adult-onset AT/RT with extracranial metastasis is extremely rare and lacks standardized treatment protocols.
Abstract
A 47-year-old woman visited a hospital with complaints of headache and epistaxis. A mass lesion was found in the sellar region, and the patient underwent partial removal via transsphenoidal surgery at the hospital. Pathological diagnosis revealed an atypical teratoid/rhabdoid tumor (AT/RT), and she was referred to our hospital for postoperative adjuvant therapy. Although chemotherapy with ifosfamide, carboplatin, and etoposide (ICE regimen) was administered, the residual tumor rapidly grew, and the patient presented with visual disturbance. Irradiation significantly reduced the tumor size. She was stable for 17 weeks; however, dissemination occurred in the left frontal lobe and lumbar spinal cord, and multiple metastases to the lungs occurred. The patient was treated with additional irradiation, oral temozolomide, intrathecal methotrexate, and intrathecal cytarabine; however, these…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
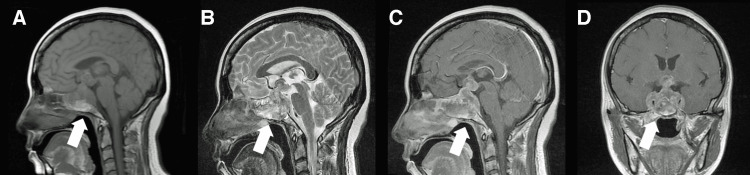 Figure 1
Figure 1 Figure 2
Figure 2 Figure 3
Figure 3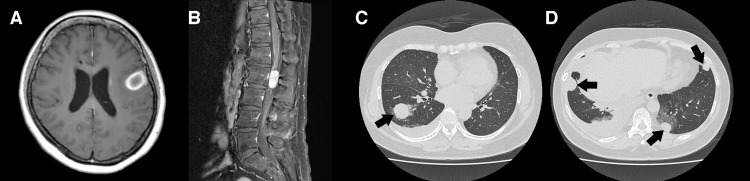 Figure 4
Figure 4| Parameters | Unit and value | Reference range |
| Total protein | 7.4 g/dL | 6.2-8.0 g/dL |
| Total bilirubin | 0.7 mg/dL | 0.2-1.0 mg/dL |
| Urea nitrogen | 6.4 mg/dL | 7-20 mg/dL |
| Creatinine | 0.61 mg/dL | 0.6-1.2 mg/dL |
| LDH | 240 U/L | 115-245 U/L |
| C-reactive protein | 2.31 mg/dL | 0-0.5 mg/dL |
| Sodium | 136 mEq/L | 133-145 mEq/L |
| Potassium | 3.9 mEq/L | 3.3-5.0 mEq/L |
| Chloride | 97 mEq/L | 98-109 mEq/L |
| White blood cell count | 4,900/µL | 3,500-9,000/µL |
| Hemoglobin | 14.7 g/dL | 11.3-14.9 g/dL |
| Platelet count | 226,000/µL | 100,000-380,000/µL |
| GH | 1.28 ng/mL | 0.13-9.88 ng/mL |
| TSH | 0.036 μIU/mL | 0.541-4.261 μIU/mL |
| ACTH | 6.8 pg/mL | 7.2-63.3 pg/mL |
| LH | 0.22 mIU/mL | 0.5-15.0 mIU/mL |
| FSH | 4.34 mIU/mL | 0.5-5 mIU/mL |
| Prolactin | 169 ng/mL | 0-15 ng/mL |
| ADH | 0.6 pg/mL | 0-2.8 pg/mL |
| Parameters | Number (%) | ||
| Number of cases | 73 | ||
| Age, median (range) | 38 (15-73) | ||
| Sex | Male | Female | |
| 26 (35.6%) | 47 (64.4%) | ||
| Location | Total | Male | Female |
| Sellar | 34 (46.6%) | 5 (14.7%) | 29 (85.3%) |
| Pineal | 12 (16.4%) | 6 (50.0%) | 6 (50.0%) |
| Hemisphere | 10 (13.7%) | 7 (70.0%) | 3 (30.0%) |
| Posterior fossa | 8 (11.0%) | 3 (37.5%) | 5 (62.5%) |
| Spinal | 5 (6.8%) | 1 (20.0%) | 4 (80.0%) |
| Others | 4 (5.5%) | 4 (100.0%) | 0 (0.0%) |
| Extent of resection | |||
| Gross total resection | 19 (26.0%) | ||
| Subtotal or partial resection | 30 (41.1%) | ||
| Biopsy | 3 (4.1%) | ||
| Not described | 21 (28.8%) | ||
| Median survival time | Months | ||
| Overall | 73 (100%) | 24 | |
| Surgery alone | 14 (19.2%) | 2.5 | |
| Surgery + chemoradiotherapy | 32 (43.8%) | 33 | |
| Surgery + chemotherapy | 3 (4.1%) | 13 | |
| Surgery + radiotherapy | 16 (21.9%) | 20 | |
| Adjuvant therapy: details unknown | 8 (11.0%) | 6 | |
| Chemotherapeutic agents | |||
| Etoposide | 21 (28.8%) | ||
| Cisplatin | 16 (21.9%) | ||
| Ifosfamide | 14 (19.2%) | ||
| Vincristine | 12 (16.4%) | ||
| Cyclophosphamide | 11 (15.1%) | ||
| Carboplatin | 9 (12.3%) | ||
| Temozolomide | 9 (12.3%) | ||
| Others | 13 (17.8%) | ||
| Authors, year | Age/sex | Location | Initial treatment | Time from surgery to metastasis | Metastasis | Treatment after metastasis | Outcome |
|
Moretti et al. (2013) [ | 60/female | Sellar | Surgery alone | 5 months | Lung | RT, CT | Death after 30 months |
|
Johann et al. (2019) [ | 20/female | Sellar | Surgery, HD-CT | 120 months | Peripheral nerve | NA | Death after 120 months |
|
Fukuda et al. (2022) [ | 45/female | Sellar | Surgery, RT, CT | NA | Lung, L4-5 spinous process | RT, CT | Death after 5 months |
| Present case | 47/female | Sellar | Surgery, RT, CT | 29 weeks | Lung | RT, CT | Death after 8 months |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsChromatin Remodeling and Cancer · Cancer Mechanisms and Therapy
Introduction
Atypical teratoid/rhabdoid tumors (AT/RTs) are rare, accounting for 6.1% of malignant central nervous system tumors in children. These are highly malignant embryonal tumors, and 68.4% of them occur in infants and children under three years of age [1]. From a molecular genetic perspective, nearly all cases exhibit biallelic inactivation (deletion or mutation) of the INI1 (hSNF5, SMARCB1) gene located on chromosome 22q11.2, and this loss of function is considered the primary driver of tumor development. In extremely rare cases, mutations in SMARCA4/BRG1 have also been reported. Histologically, rhabdoid cells with eosinophilic cytoplasm and inclusion-like structures are characteristic. However, when these distinctive features are not well-developed, differentiation from medulloblastoma and other tumors can be challenging. Immunohistochemically, SMARCB1/INI1 staining is negative in tumor cells, which can lead to a diagnosis of AT/RT.
Currently, there is no established standard treatment. Depending on the case, multimodal therapies such as the Medical University of Vienna (MUV)-ATRT protocol or European Rhabdoid Registry (EU-RHAB) protocol are employed. However, the prognosis remains extremely poor, with a five-year survival rate of only 39.5% [1]. Adult-onset AT/RT is extremely uncommon, with a limited number of reported cases. Extracranial metastases of adult-onset AT/RT are even more uncommon, and only three cases of extracranial metastases have been documented. There is also no established standard treatment for adult cases, so the accumulation of additional cases is necessary. Herein, we report a case of adult-onset AT/RT, describe its clinical course, and discuss the characteristics based on a literature review.
Case presentation
A 47-year-old woman visited a hospital complaining of a three-week progressive headache and epistaxis that she had experienced a week earlier. Additionally, she experienced irregular menstruation for one year. To date, no remarkable family history has been reported. Magnetic resonance imaging (MRI) revealed a 20 × 15 × 13 mm tumor extending from the sphenoid sinus to the suprasellar region (Figure 1). Laboratory data indicated an elevated prolactin level of 169 ng/mL and a low thyroid-stimulating hormone level of 0.036 μIU/mL (Table 1), whereas the levels of other pituitary hormones remained normal. The visual function also remained intact. The patient presented with diplopia due to right oculomotor and abducens nerve palsy. Three weeks later, she developed right facial numbness and left oculomotor nerve palsy. On the 23rd day after her first visit, the patient underwent partial tumor resection using the transsphenoidal approach. Histopathological examination revealed rhabdoid cells with an eosinophilic cytoplasm and inclusion-like structures. Moreover, immunohistochemical staining demonstrated the absence of SMARCB1/INI1 expression (Figure 2), confirming the diagnosis of AT/RT. The patient was referred to our institution on postoperative day 8 for adjuvant therapy. Upon admission, she was diagnosed with diabetes insipidus. Additional MRI revealed no evidence of spinal lesions, and cerebrospinal fluid cytology was negative. However, the rapid growth of the residual tumor in the suprasellar region (Figure 3A) led to progressive bilateral visual impairment.
Preoperative MRIA and B: T1-weighted (A) and T2-weighted (B) sagittal MRI scans showing a mass lesion extending from the sphenoid sinus to the suprasellar region (arrows). C and D: Gadolinium-enhanced sagittal (C) and coronal (D) MRI scans showing increased mass enhancement with cavernous sinus invasion (arrows).MRI: magnetic resonance imaging
Histopathological FindingsA and B: Hematoxylin and eosin staining showing scattered rhabdoid cells with acidophilic cytoplasm and inclusion body-like structures. C: Immunostaining revealing negativity for SMARCB1/INI1. D: MIB-1 index is 50%-60%.
MRI During Chemotherapy and Radiation TherapyA: Gadolinium-enhanced MRI just before chemotherapy revealing regrowth of the residual tumor. B: Gadolinium-enhanced MRI 37 days after the induction of chemotherapy demonstrating rapid progression of the tumor. C: Gadolinium-enhanced MRI after radiation therapy showing a significant reduction in tumor size.MRI: magnetic resonance imaging
Chemotherapy with ifosfamide (1,900 mg/m^2^), carboplatin (400 mg/m^2^), and etoposide (130 mg/m^2^) (ICE regimen) was administered at this time. An MRI performed 10 days after the initiation of chemotherapy revealed tumor shrinkage, accompanied by improvement in symptoms. However, rapid tumor regrowth was observed 37 days after the initiation of chemotherapy (Figure 3B), resulting in bilateral visual impairment and right external ophthalmoplegia.
The second course of ICE chemotherapy (80% dose due to bone marrow suppression) was administered concurrently with irradiation (54 Gy/30 fractions) targeting the sphenoid sinus and suprasellar regions. Following radiotherapy, significant tumor shrinkage was noted (Figure 3C), and visual impairment improved. The third course of ICE chemotherapy (60% dose for the same reason) was administered. The patient remained progression-free for some time; however, 191 days after the initial chemotherapy, she developed dysarthria and pain in the right lower limb. MRI revealed dissemination to the left frontal lobe and lumbar spinal cord (Figures 4A, 4B); meanwhile, whole-body computed tomography confirmed the presence of multiple pulmonary metastases (Figures 4C, 4D). Radiotherapy was administered to the left frontal lobe (35 Gy/5 fractions) and lumbar lesions (39 Gy/13 fractions), along with oral temozolomide (90 mg/m²) and intrathecal delivery of methotrexate (9 mg/m²) and cytarabine (30 mg/m²). Radiotherapy was also administered to the rapidly enlarging lesion in the right lower lobe of the lung but was discontinued at 33 Gy/11 fractions due to worsening pleural effusion. Subsequently, tumor progression could not be controlled. The patient died 254 days (36 weeks) after the introduction of the ICE regimen.
MRI and Computed Tomography Six Months After Initial TreatmentA and B: Gadolinium-enhanced MRI six months after initial treatment demonstrating dissemination in the left frontal lobe and the lumbar spinal cord. C and D: Computed tomography six months after initial treatment revealing multiple lung metastases (arrows).MRI: magnetic resonance imaging
Discussion
An AT/RT is a rare and highly malignant embryonal tumor. The predominant age of onset is under three years [1]. In contrast, adult cases accounted for approximately 2% of all cases. Due to the rarity of the tumor, a standard treatment, even for pediatric cases, has not yet been established. Moreover, various chemotherapy regimens using agents such as cisplatin, carboplatin, cyclophosphamide, etoposide, and vincristine, as well as radiation therapy, are utilized. In adults, knowledge and evidence are even more scarce.
We reviewed the literature on adult-onset AT/RTs and identified 80 cases in 48 articles [2-18]. Clinical information, including age, treatment details, and prognosis, was available for 73 of these cases, which we analyzed. The details are summarized in Table 2. The median age of adult-onset AT/RTs was 38 years (range: 15-73 years), with a slight predominance in females (64.4%, n=47). The most common tumor location was the sellar region (46.6%, n=34), followed by the pineal region (16.4%, n=12), cerebral hemisphere (13.7%, n=10), posterior fossa (11.0%, n=8), and spinal canal (6.8%, n=5). Tumors in the sellar region and spinal canal were more common in females (85% and 80%, respectively), whereas those in the cerebral hemisphere were predominantly identified in males (70%). Our case was typical of adult-onset AT/RT in terms of age at onset, sex, and location. The extent of resection was documented in 52 cases in the literature. Gross total resection, subtotal or partial resection, and biopsy were performed in 19 cases (26%), 30 cases (41.1%), and three cases (4.1%), respectively.
The median survival time of the 73 patients was 24 months. Among the post-surgical treatment modalities, excluding eight cases in which the administration of chemotherapy or radiation therapy was unclear in the literature, patients receiving combined chemoradiotherapy (43.8%, n=32) had a relatively long median survival of 33 months, whereas those receiving chemotherapy (4.1%, n=3) or radiation therapy (21.9%, n=16) alone had median survivals of 13 and 20 months, respectively. The most frequently administered chemotherapy regimens included etoposide (28.8%, n=21) or cisplatin (21.9%, n=16). Intrathecal chemotherapy was administered in six patients, and autologous stem cell transplantation (ASCT) was performed in five patients. A cohort study of pediatric AT/RT patients treated with high-dose chemotherapy and ASCT reported a five-year overall survival rate of 100% and a five-year progression-free survival rate of 88.9% [19]. In adults, a case report using ASCT described a 17-month disease-free rate [15]. Therefore, ASCT could be an effective treatment option. In pediatric cases, the effectiveness of Aurora kinase inhibitors and EZH2 inhibitors have been reported. The accumulation of pediatric cases and the potential application of these therapies to adult patients are anticipated.
Our patient was managed primarily with ICE chemotherapy, a regimen employed for pediatric medulloblastoma, due to concerns regarding spinal dissemination. However, ICE alone was insufficient for tumor control, and the addition of radiation therapy resulted in a relatively stable period. Previous reports on pediatric cases have widely acknowledged the effectiveness of radiotherapy. Additionally, early introduction of radiotherapy has been associated with improved survival outcomes [20]. However, further research is needed to determine the optimal timing of radiotherapy. In our case, oral temozolomide and intrathecal administration of methotrexate and cytarabine, which are included in some pediatric treatment protocols, were performed for tumor recurrence and spinal metastasis. However, its effectiveness was limited. The efficacy of intrathecal administration has not been established, and further research is also needed.
Our patient developed extracranial metastases, a phenomenon rarely reported in adult patients with AT/RT. To date, three cases of extracranial metastases have been documented in adult patients with AT/RT (Table 3). All cases, including ours, originated in the sellar region. Three cases developed metastases to the lungs (one of which also had metastasis to the lumbar spinous process), and one case involved metastasis to the peripheral nerves. All patients, except for one with unknown details, underwent partial resection. The period from diagnosis to metastasis ranged from three months to 10 years. Long-term survival after the detection of metastasis was achieved in only one case (25 months), while the remaining three cases resulted in death within three months, indicating an extremely poor prognosis. Sellar lesions suggest the potential for hematogenous metastasis due to cavernous sinus invasion [6]. For patients with partially resected sellar lesions, close monitoring is essential for identifying cases of extracranial metastases.
AT/RT is highly challenging to treat in both pediatric and adult cases. The treatment methods for adult AT/RT vary significantly across the literature, and there is no standardized protocol, making it difficult to evaluate detailed clinical courses and treatment efficacy. Further accumulation of these cases is essential, and prospective data collection, collaborative registries, and efforts to standardize treatment strategies are considered to elucidate their pathophysiology and establish effective treatments.
Conclusions
Here, we report a case of adult-onset AT/RT with extracranial metastases. Radiation therapy was deemed to be relatively effective. Partial resection of sellar lesions is likely to result in extracranial metastasis. Further accumulation of adult-onset AT/RT cases is essential, and prospective data collection and collaborative registries are considered to elucidate their pathophysiology and establish effective treatments.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Incidence of atypical teratoid/rhabdoid tumors in children: a population-based study by the Austrian Brain Tumor Registry, 1996-2006 Cancer Woehrer A Slavc I Waldhoer T 5725573211620102073741810.1002/cncr.25540 · doi ↗ · pubmed ↗
- 2Atypical teratoid/rhabdoid tumor of the sellar region in an adult male: a case report Cureus Aldhafeeri W Habelrih F Alshehri LA Abdullah J Alkutbi MM Shah SM 015202310.7759/cureus.36599 PMC 1012253637095822 · doi ↗ · pubmed ↗
- 3Atypical teratoid/rhabdoid tumor in adults: a systematic review of the literature with meta-analysis and additional reports of 4 cases J Neurooncol Broggi G Gianno F Shemy DT 11415720223521794810.1007/s 11060-022-03959-z · doi ↗ · pubmed ↗
- 4A case of an atypical teratoid/rhabdoid tumor with distinctive histology in the pineal region in an adult patient Pathol Int Doi M Koike J Yoshida Y 7777827120213447388310.1111/pin.13159 PMC 9292907 · doi ↗ · pubmed ↗
- 5Primary adult sellar SMARCB 1/INI 1-deficient tumor represents a subtype of atypical teratoid/rhabdoid tumor Mod Pathol Duan Z Yao K Yang S 191019203520223580404110.1038/s 41379-022-01127-2PMC 9708584 · doi ↗ · pubmed ↗
- 6An adult case of sellar atypical teratoid/rhabdoid tumor presenting with lung metastasis, harboring a compound heterozygous mutation in INI 1NMC Case Rep J Fukuda N Ogiwara M Nakata S 267274820213507947410.2176/nmccrj.cr.2020-0128 PMC 8769414 · doi ↗ · pubmed ↗
- 7Atypical teratoid/rhabdoid tumor of the brain in an adult with 22q deletion but no absence of INI 1 protein: a case report and review of the literature Folia Neuropathol Jin S Sun C Yu S Wang Q An T Wen Y 80855320152590987810.5114/fn.2015.49977 · doi ↗ · pubmed ↗
- 8Sellar region atypical teratoid/rhabdoid tumors (ATRT) in adults display DNA methylation profiles of the ATRT-MYC subgroup Am J Surg Pathol Johann PD Bens S Oyen F 5065114220182932447110.1097/PAS.0000000000001023 · doi ↗ · pubmed ↗