Non-infectious inflammation in atrial septum after GORE® CARDIOFORM septal occluder implantation
Ryotaro Maeda, Takeshi Nakamura, Michiyo Yamano, Satoaki Matoba

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
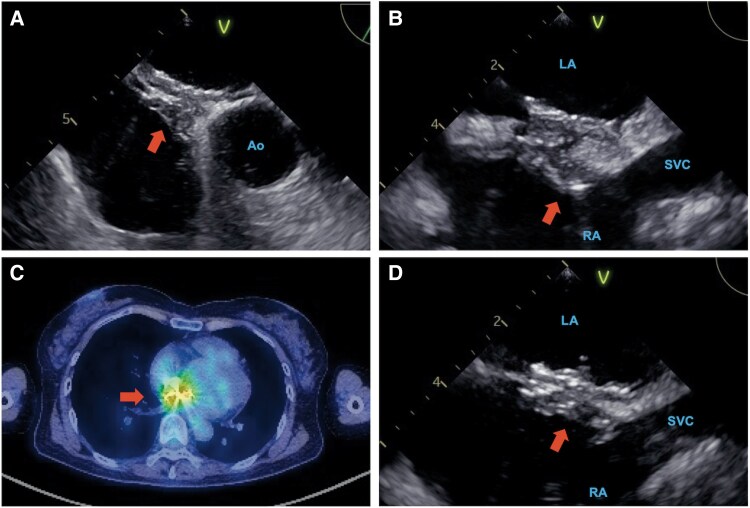 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCardiovascular and Diving-Related Complications · Atrial Fibrillation Management and Outcomes · Infective Endocarditis Diagnosis and Management
Case description
A 56-year-old female patient was admitted to our institution with fever 5 days after uncomplicated implantation of a 25-mm GSO device for patent foramen ovale which caused paradoxical cerebral infarction. Although the laboratory test showed a high level of inflammatory reaction (C-reactive protein: 9.45 mg/dL), repeated blood cultures and procalcitonin were all negative. Transoesophageal echocardiography demonstrated marked wall thickening of the atrial septum at and around the site of the GSO implantation (Figure 1A and B), though no other abnormal findings such as vegetation, intracardiac thrombus, pericardial effusion, or erosion were detected. An ^18^F-fluorodeoxyglucose positron emission tomography (FDG-PET) revealed a high level of FDG accumulation at the site of the GSO implanted in the atrial septum (Figure 1C). A patch testing for components of GSO [nickel, titanium, and expanded polytetrafluoroethylene (ePTFE)] was all negative. Her fever gradually subsided within 7 days of admission, and the laboratory test showed that her inflammatory response was decreasing day by day. The second TEE, 1 week after the first, demonstrated a spontaneous remission of the atrial septal wall thickening (Figure 1D). She was discharged after careful observation and had no recurrence of symptoms at her 1-month follow-up. Based on the results of each examination, the origin of the fever was considered to be a non-infectious, non-allergic inflammation caused by excessive healing process of the atrial septum. Patent foramen ovale closure using a percutaneous occluder is a well-established procedure, and complications requiring surgical explantation of a device due to infection, erosion, and allergy are rarely reported.^1,2^ However, the development of fever and inflammation after the procedure is sometimes observed, which resolves spontaneously.^3^ The present case suggests that close observation should be sought first instead of hasty explantation after exclusion of device infection, erosion, thrombosis, and allergic reaction.
(A and B): (A) Mid-oesophageal aortic valve short-axis view, (B) mid-oesophageal bicaval view. The first transoesophageal echocardiography shows marked thickening of the atrial septal wall at the site of GORE CARDIOFORM septal occluder (GSO) implantation (arrow). (C) An 18F-fluorodeoxyglucose (FDG) positron emission tomography shows a high level of 18F-fluorodeoxyglucose accumulation at the site of the GORE CARDIOFORM septal occluder implanted in the atrial septum (arrow). (D) Mid-oesophageal bicaval view. The second transoesophageal echocardiography shows a remission of the atrial septal wall thickening at the site of the GORE CARDIOFORM septal occluder implantation (arrow). Ao, aorta; LA, left atrium; RA, right atrium; SVC, superior vena cava.
Consent: The authors confirm that written consent for the submission and publication of this case report has been obtained from the patient in line with the Committee on Publication Ethics guidance.
Funding: None declared.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Verma SK, Tobis JM. Explantation of patent foramen ovale closure devices: a multicenter survey. JACC Cardiovasc Interv 2011;4:579–585.21596333 10.1016/j.jcin.2011.01.009 · doi ↗ · pubmed ↗
- 2Taggart NW, Reeder GS, Lennon RJ, Slusser JP, Freund MA, Cabalka AK, et al Long-term follow-up after PFO device closure: outcomes and complications in a single-center experience. Catheter Cardiovasc Interv 2017;89:124–133.27027873 10.1002/ccd.26518 · doi ↗ · pubmed ↗
- 3Galasso F, Wassenaar F, Barry T, Baqal OJ, Hagler DJ, Sweeney JP, et al A retrospective analysis of self-limiting fever following percutaneous patent foramen ovale and atrial septal defect closure. Cardiol Res Pract 2024;2024:5562208.39421324 10.1155/2024/5562208 PMC 11483646 · doi ↗ · pubmed ↗