Treatment-seeking practices of caregivers for children aged less than five years old with diarrhoea in low- and middle-income countries: a systematic review and meta-analysis
Gedefaw Abeje Fekadu, Muluemebet Abera Wordofa, Firmaye Bogale Woldie, Robera Olana Fite, Kassahun Alemu, Alemayehu Worku, Lisanu Taddesse, Delayehu Bekele, Getachew Tolera, Grace J Chan, Damen Hailemariam

TL;DR
This study reviews how often caregivers in low- and middle-income countries seek medical help for young children with diarrhea, finding that treatment-seeking practices remain low.
Contribution
The study provides a comprehensive meta-analysis of treatment-seeking practices for childhood diarrhea in low- and middle-income countries.
Findings
The overall treatment-seeking practice was 52.84% across low- and middle-income countries.
No significant difference was found in treatment-seeking practices between different income-level countries.
Treatment-seeking varied by location, with the lowest rates in peri-urban areas.
Abstract
Diarrhoeal diseases in children aged <5 years require immediate medical attention. However, previous studies conducted on treatment-seeking practices of caregivers for children aged <5 years with diarrhoea in low- and middle-income countries (LMICs) were inconsistent and inconclusive. We aimed to estimate the pooled treatment-seeking practice of caregivers for children aged <5 years with diarrhoea in LMICs. We used the 2020 PRISMA guidelines to conduct this systematic review and meta-analysis. We included both published and unpublished articles in English that reported treatment-seeking practices from health facilities in LMICs between 2010–22. We searched CINAHL, Medline/PubMed, Web of Science, Embase, and grey literature sources. We assessed the eligible articles using the Newcastle-Ottawa Scale quality appraisal checklist and Begg’s test for the presence of publication bias.…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
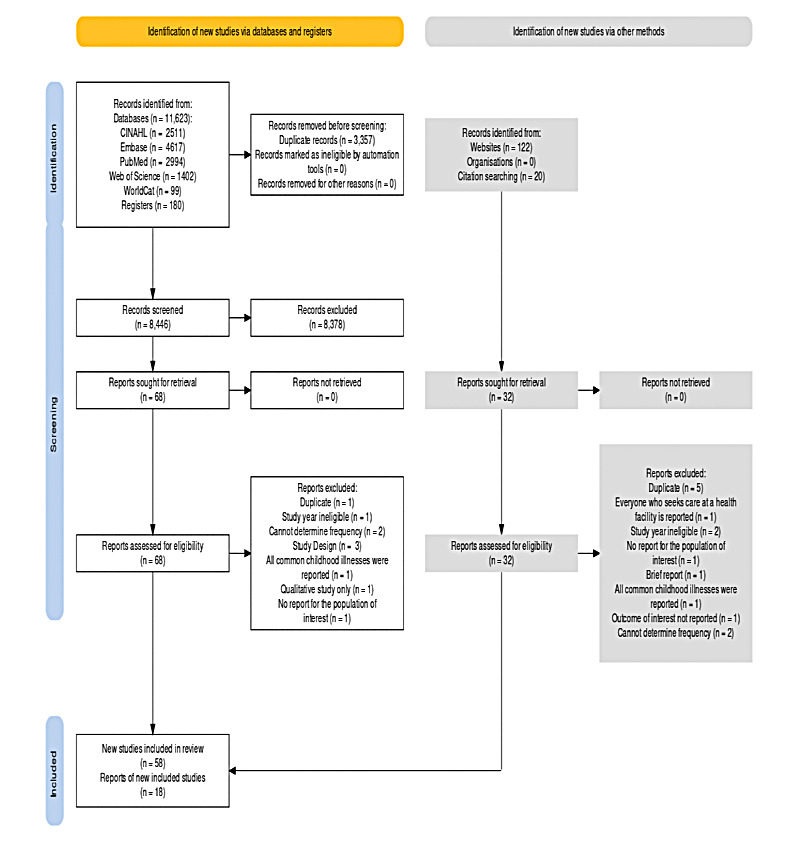 Figure 1
Figure 1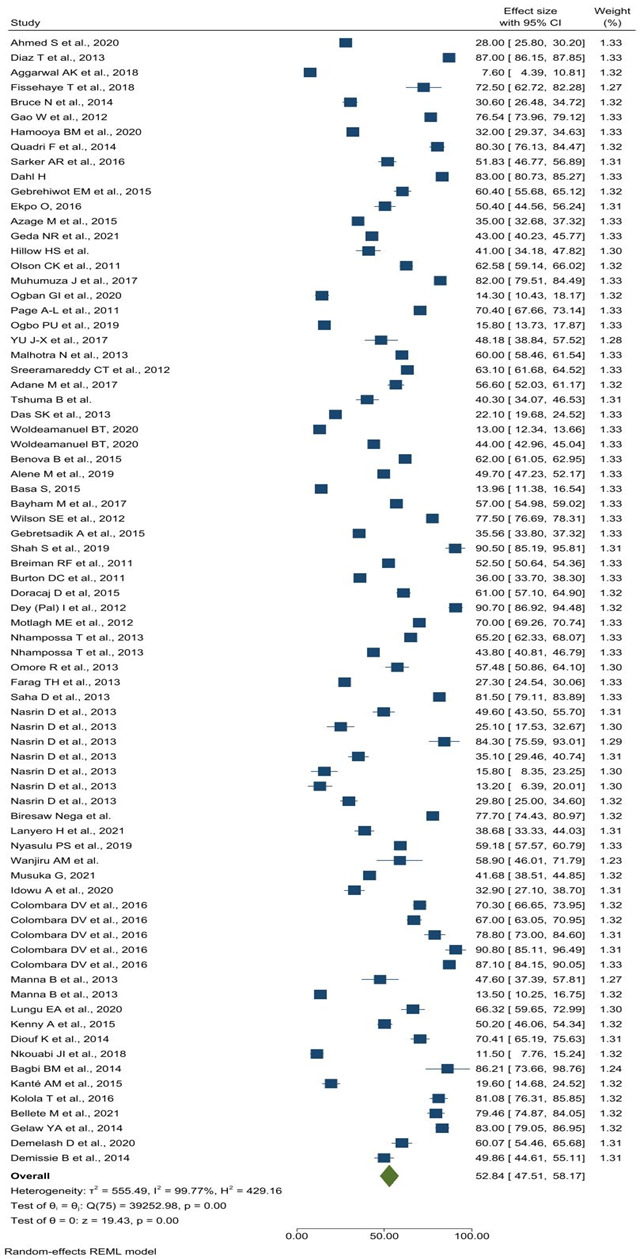 Figure 2
Figure 2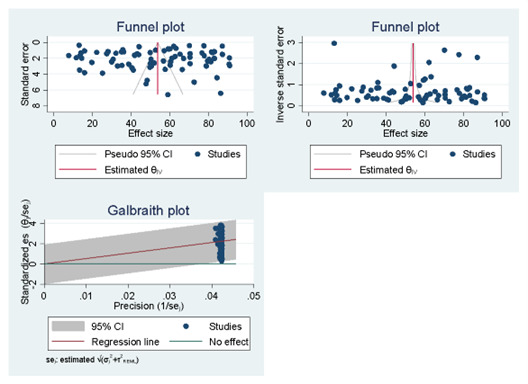 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsChild Nutrition and Water Access · Child Nutrition and Feeding Issues · Global Maternal and Child Health
Although preventable and treatable, diarrhoea is the leading cause of morbidity and mortality among children aged <5 years globally [1]. In 2019, diarrhoea was responsible for the deaths of 370 000 children aged <5 years worldwide [2–5]. Diarrhoea is widespread in low- and middle-income countries (LMICs). Children aged <5 years in low-income countries experience an average of three episodes of diarrhoea each year [6].
Diarrheal diseases in children aged <5 years require immediate medical attention. However, in LMICs, the diagnosis and treatment for children aged <5 years with diarrhoea are limited [5]. In addition, the use of health care services by caregivers of children aged <5 years with diarrhoea is determined by caregivers' age, residence, marital status, exposure to media, household wealth index, perceived severity of illness, knowledge of caregivers, educational status, distance from health facilities, geographical barriers to health care access, overall community level literacy, and place of delivery [7–10]. Medical treatment costs are also a burden in some LMICs. When receiving treatment for paediatric diarrhoea, 79% of all costs incurred are direct expenses [11–15].
Previous studies have been conducted in LMICs reporting treatment-seeking behaviour for children aged <5 years with diarrhoea [16–18]. However, the findings reported were inconsistent and inconclusive and did not provide practical recommendations. For example, the treatment-seeking practice ranged from 11.5% in a study conducted in Tanzania [19] to 87% in a study conducted in Niger [20]. The World Health Organization (WHO) recommends gathering evidence on caregivers’ treatment-seeking behaviour, which is critical in informing policy and programs aimed at lowering mortality due to diarrhoea among children aged <5 years [15]. The evidence from this systematic review and meta-analysis can be used by stakeholders, including policymakers and program planners, to improve treatment-seeking practices. Therefore, we aimed to estimate the pooled treatment-seeking practice for diarrhoea among children aged <5 years in LMICs.
METHODS
Study design
We used the 2020 PRISMA guidelines [12] while writing this systematic review and meta-analysis. We searched studies using a combination of condition, context, and population criteria. We included research that reported treatment-seeking practices of caregivers for children aged <5 years with diarrhoea from health facilities (public or private hospitals, health centres, health posts, clinics, sentinel health centres) in LMICs. We included articles that originated from LMICs based on the World Bank country and lending groups classification based on gross national income for the fiscal year 2022. We included both quantitative and mixed-method observational studies (cross-sectional, case-control, and cohort studies) based on caregivers’ reports or from health facility records. We searched both published and unpublished articles or reports in English between 2010–22. We excluded articles published before 2010 because of the availability of published systematic reviews between 1990–2010.
Search strategy and searching sources
We searched multiple databases, including CINAHL, Medline/PubMed, Web of Science, and Embase to access published articles. We searched unpublished articles (grey literature) from Google Scholar, WorldCat, OpenGrey, and online thesis/dissertation repositories. We also screened references of identified articles to identify potential articles that were not found by searching databases. Three independent reviewers (GA, FB, and RO) searched the articles in the databases. We used MeSH keywords and free text search terms to identify the articles. We used the following search terms: diarrh (o)ae, treatment, treatment-seeking, health care seeking, health-seeking behaviour/practice(s), child/children, childhood, under-five, mother, caregiver, developing countries, low-income, middle-income, and the name of each country and combined them with Boolean operators ‘OR’ and ‘AND’ to either broaden or narrow the search (Table S1 in the Online Supplementary Document).
Study selection
We exported all articles to EndNote, version 20.0 (Clarivate Analytics, London, UK) to remove the duplicates and archive. Three authors (GAF, FB, and ROF) reviewed these based on the inclusion and exclusion criteria. Any disagreements between authors were resolved by discussion or by a fourth reviewer (KA).
Data extraction and processing
We used a standardised pretested data extraction tool that gathered information on author, publication status, study setting, country, LMIC status, study period, urban/rural, study design, sample size, treatment-seeking practice for diarrhoea, sampling methods and methodology. Three independent reviewers (GAF, FB, and ROF) extracted the data. The extracted data was exported to Excel, version 2013 (Microsoft Corporation, Redmond, Washington, USA). We thoroughly checked the data for completeness, and we linked the references to the articles using the unique identifiers provided. We checked the missing data from the articles using the identifier. The clean version of this Excel file was imported into Stata, version 17.0 (StataCorp, College Station, Texas, USA).
Quality appraisal
We assessed the quality of the included articles using the Newcastle-Ottawa Scale quality appraisal checklist [12]. The scale has a three-domain system, including study group selection, group comparability, and exposure/outcome determination. These domains are divided into eight items, with a maximum possible score of nine. Articles scoring six to nine were rated as good quality, articles scoring three to seven were rated as fair, and those scoring less than three were rated as poor [12].
Synthesis and analysis
We performed a narrative synthesis to characterise the study participants, study types, study settings, and countries' income classification (Table S2 in the Online Supplementary Document).
We used Stata, version 17.0 (StataCorp, College Station, Texas, USA) to analyse the pooled estimate of treatment-seeking practice for diarrhoea in children aged <5 years using a forest plot. To assess homogeneity of study-specific effect sizes, we used the Cochran Q statistic. We used the Q test statistics-related P-value to identify any significant heterogeneity between the studies [13]. We used I^2^ statistics to quantify how much the heterogeneity between studies contributed to the variability in effect-size estimates. Further, we used a random-effects model to assess the pooled treatment-seeking practice for diarrhoea in children aged <5 years [14]. Moreover, we performed a subgroup analysis considering the articles' publication status, place of residence (urban, rural, peri-urban), World Bank income category, study design and approach, and study setting (facility or community-based). We used the test of group difference (Q_b) and associated P-value to determine if there was a significant difference in the group-specific overall effect sizes among each subgroup. Moreover, we used the funnel plot to assess the small-study effect. To determine the presence of publication bias, we used Begg’s test for small-study effects and the regression-based Egger test for small-study effects [15]. When determining the presence of publication bias and small-study effects, we used a P-value of 0.05.
RESULTS
We identified 11 765 articles, including 2511 from CINAHL, 4617 from Embase, 2994 from PubMed, 1402 from Web of Science, and 99 from WorldCat. We discovered 180 articles from other sources, including registers, Google Scholar, and repositories. We removed 3362 because of duplications. After screening the titles and abstracts, we removed totsal 8397 articles. We included the remaining 76 articles in the systematic review and meta-analysis (Figure 1).
PRISMA 2020 flowchart of article search and selection process to estimate the pooled treatment-seeking practices among caregivers for children aged <5 years with diarrhoea, systematic review and meta-analysis in low- and middle-income countries, 2010–22.
Study characteristics
There were 71 published studies and five unpublished articles among the 76 included studies. Three studies [16–18] were conducted in health care facilities, with the remaining 73 conducted in the community. One study was conducted in Albania [21], four in Bangladesh [22–25], one in Botswana [18], one in Burkina Faso [26], one in Burundi [27], two in China [3,4], one in Egypt [28], one in El Salvador [29], 15 in Ethiopia [30–44], two in Gambia [5,6], two in Guatemala [29,45], seven in India [6–12], one in Iran [46], six in Kenya [6,13–17], one in Liberia [47], two in Malawi [18,19], two in Mali [23,48], one in Mexico [29], three in Mozambique [6,20,21], one in Nepal [49], one in Nicaragua [29], one in Niger [50], five in Nigeria [22–26], two in Pakistan [23,51], one in Panama [29], one in Sierra Leone [52], one in Somalia [53], two in Tanzania [54,55], two in Uganda [56,57], two in Zambia [58,59], and one in Zimbabwe [60].
According to the World Bank's income classification, 33 studies were conducted in low-income countries, 38 in lower-middle-income countries [2,6–17,22–37], and five in upper-middle-income countries [3,4,37–39] (Table S2 in the Online Supplementary Document). The studies used different study periods ranging from a week to years. However, 10 studies [31,32,35,49,53,56,61–64] did not mention their study period (Table S2 in the Online Supplementary Document)
In terms of urban or rural study sites, one study was conducted in peri-urban areas, 21 studies in rural areas [2,5,6,11,15,21,25,34,36-40,45,46,61,65–69], five in semi-urban areas [3,23,24,28,70], 11 in urban areas [24,28,30,42,44,46,48,50,61,71,72], 30 in both urban and rural areas [7-9,13,16-18,20,22,26,27,29,32–35,48–50,63,72–77], and one study in urban, rural, and semi-urban areas [28] (Table S2 in the Online Supplementary Document).
In terms of study design, there were three case-control studies [6,12,65], one comparative cross-sectional study [38], and the remaining cross-sectional studies. 71 studies were quantitative, while five were both quantitative and qualitative [2,17,23,45,70].
The mean sample size in these studies was 1500. Study sampling varied with three studies [6,11,14] involving the children. Two studies [19,71] used cluster sampling. One study [16] used consecutive sampling, and one study [27] used convenience sampling. Ten studies [17,25,30,32–35,62,71,76] used multistage sampling. The sampling methods of nine studies [12,19,26,29,35,37,38,61,62] were not specified. One study [73] stated it used proportional allocation. 20 studies used random sampling [2,3,5–7,16,21–23,28,31,32,38,47,61,65,69,70,74,77,78]. Seven studies used stratified cluster sampling [8,9,27,48,49,66,67,72]. Three studies used stratified random sampling [21,30,32] and six studies [13,38,40,45,61,79] used systematic sampling method (Table S2 in the Online Supplementary Document).
Pooled treatment-seeking practice for diarrhoea
The overall estimated treatment-seeking practices among caregivers for children aged <5 years with diarrhoea in LMICs was 52.84% (95% confidence interval (CI) = 47.51–58.17). I^2^ of 99.77 indicated that differences between studies account for approximately 99.77% of the variability in effect-size estimates (Figure 2).
Pooled treatment-seeking practices for caregivers for children aged <5 years with diarrhoea, systematic review and meta-analysis in low- and middle-income countries, 2010–22.
Small study effects and publication bias analysis
Most studies were randomly scattered within the pseudo-95% CI region, and the spread of the observed effect sizes on the estimate of the overall effect size was asymmetric. This indicates the absence of a small-study effect. Similarly, the Galbraith plot indicates that all the effect sizes fall between the no effect and regression lines, indicating that there was no significant heterogeneity because all the studies' effect sizes fall within the 95% CI region (Figure 3).
Funnel and Galbraith plots of meta-analysis of the pooled treatment-seeking practices for caregivers for children aged <5 years with diarrhoea, systematic review and meta-analysis in low- and middle-income countries, 2010–22.
For the null hypothesis test of no small-study effects using the regression-based Egger test and assuming a random-effects model with the residual maximum likelihood estimation method, the magnitude of the small-study effects was 1.17 with a standard error of 2.117 and a Z-score of 0.55 with a P < 0.5814. This demonstrates funnel-plot symmetry.
Subgroup analysis
Treatment-seeking practice was estimated to be 52.45% (95% CI = 46.81–58.10) using published articles and 57.43% (95% CI = 47.81–73.05) using unpublished articles. Using Q statistics revealed that Q = 38 371.88 among published articles and Q = 646.78 among unpublished articles (P < 0.001) indicated significant heterogeneity. Similarly, the I^2^ values for published articles were I^2^ = 99.79 and for unpublished articles I^2^ = 98.96, indicating their respective variability in effect-size estimates. The test of group differences (Q_b = 0.34; P = 0.56) indicated that the group-specific overall effect sizes were not statistically different.
The test of group (Q_b = 174.50; P < 0.001) indicated that the group-specific overall effect sizes among studies were all statistically different: 54.20% in rural areas (95% CI = 44.71–63.7), 47.76% (95% CI = 34.47–61.06) in urban areas, 55.70% (95% CI = 34.47–61.06) in both urban and rural areas, and 62.00% (95% CI = 47.81–63.59) in urban, rural and semi urban areas.
Treatment-seeking practice was estimated to be 58.12% (95% CI = 51.58–64.67) in studies conducted in low-income countries, 48.41% (95% CI = 39.75–57.06) in lower-middle-income countries, and 51.44% (95% CI = 35.47–67.41) in upper-middle-income countries. The presence of between-study heterogeneity was determined using Q statistics, which revealed that Q = 20 892.43 among articles published from low-income countries, Q = 14 887.25 among articles reported from middle-income countries, and Q = 398.61 among articles reported from upper-middle-income countries, with a P < 0.001 indicate a significant heterogeneity. Similarly, the I^2^ values were 99.67 for published articles, 99.81 for articles from lower-middle-income countries, and 98.51 for articles from upper-middle-income countries, indicating that 99.67%, 99.81%, and 98.51% of the variability in effect-size estimates was due to differences in studies between articles in each group, respectively. However, the test of group (Q_b = 3.21; P = 0.2) indicated that the group-specific overall effect sizes were not statistically different.
The test of group (Q_b = 96.09; P < 0.001) indicated that the group-specific overall effect sizes among studies that were case-control (33.44%; 95% CI = 19.89–46.99), comparative cross-sectional (83.00%; 95% CI = 79.05–86.95), and cross-sectional studies (55.32%; 95% CI = 49.81–60.82), were statistically different (P < 0.001). Using the study design of the articles included in this systematic review and meta-analysis, treatment-seeking practices were estimated to be 52.56% (95% CI = 47.12–58.01) using articles that were both qualitative and quantitative and 56.69% (95% CI = 30.11–83.26) using only quantitative studies. The presence of between-study heterogeneity was determined using Q statistics, which revealed that Q = 1453.13 among articles which were both qualitative and quantitative and Q = 31 971.5 among only quantitative studies, with a P < 0.001 in both groups indicate significant heterogeneity. Similarly, the I^2^ values were 99.75 for both groups, indicating that 99.75% of the variability in effect-size estimates is due to differences in studies between articles in each group. However, the test of group differences (Q_b = 0.09; P = 0.766) indicated that the group-specific overall effect sizes were not statistically different.
Using the study setting of the systematic review and meta-analysis articles, treatment-seeking practices were estimated to be 39.74% (95% CI = 12.83–66.65) from articles conducted at health facilities and 53.58% (95% CI = 47.94–58.82) from articles conducted at the community level. The Q = 1373.05 among articles conducted at health facilities and the Q = 37 763.86 among articles conducted at the community level, with a P < 0.001 in both groups, indicate significant heterogeneity. Similarly, the I^2^ values were 99.74 for published articles and 99.76 for unpublished articles, indicating that 99.74% and 98.76% of the variability in effect-size estimates was due to differences in studies between articles in each group, respectively. However, the test of group differences (Q_b = 0.95; P = 0.330) indicate that the group-specific overall effect sizes were not statistically different.
DISCUSSION
The estimated pooled proportion of treatment-seeking practices of caregivers for children aged <5 years with diarrhoea in LMICs was 52.84%. Disaggregated by income levels, the difference in caregiver health care-seeking practices in low-income countries (58.12%), in lower-middle-income countries (48.41%), and in upper-middle-income countries (51.44%) was not statistically different.
In LMICs, caregivers of just over half (52.84%) of children aged <5 years with diarrhoea sought treatment at health facilities. This figure is expected in LMICs due to the inaccessibility of health facilities [44,80,81], lower level of integrated primary care services [82], limitations in the implementation of child health education and social services [83], use of traditional medicines and practices [84,85], and use of dietary management of diarrhoea [86]. The overall effect size was statistically significant in the analysis, which implies the presence of significant heterogeneity between the studies. Additionally, the Q test also indicated the presence of significant heterogeneity between the studies included in this systematic review and meta-analysis. The heterogeneity may be due to the difference in the time the surveys were conducted and the difference in the study design.
The group-specific overall effect sizes among studies that were conducted in rural, urban, both urban and rural, and urban, rural, and semi-urban areas were statistically different. A study identified that the site of the study was shown to have an impact on the treatment-seeking practices for childhood diarrhoea [87]. The caregivers' economic status has also been reported to be related to the residential area, which influences the use of health care services [88]. Furthermore, geographic factors have been known to influence access to health care and the number of health providers available to care for children in various communities [89].
Similarly, the group-specific overall effect sizes among different study designs (case-control, comparative cross-sectional, and cross-sectional studies) were statistically different. Methodological heterogeneity is frequently assumed to be one of the factors contributing to heterogeneity among studies included in a meta-analysis [90,91]. We conducted a subgroup analysis to show the variation by study design.
In this systematic review and meta-analysis, we maintained a high quality of study selection and analysis. We evaluated the selected articles using a valid quality assessment tool before including them in the review. The funnel plot revealed a symmetrical distribution, revealing the small-study effect. Furthermore, small-study effects were assessed using the regression-based Egger test. One limitation was that although we included articles from multiple countries, the number of studies from some geographical areas was limited. Therefore, the results of this subgroup analysis should be interpreted with caution. In addition, this review did not address factors associated with treatment-seeking practice.
CONCLUSIONS
Treatment-seeking practice for diarrhoea among children aged <5 years in LMICs remained low. Overall, more efforts are needed to improve treatment-seeking practices. We recommend further studies to identify factors affecting treatment-seeking practices for diarrhoea among children aged <5 years in LMICs.
Additional material
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Hartman RM Cohen AL Antoni S Mwenda J Weldegebriel G Biey J Risk Factors for Mortality Among Children Younger Than Age 5 Years With Severe Diarrhea in Low- and Middle-income Countries: Findings From the World Health Organization-coordinated Global Rotavirus and Pediatric Diarrhea Surveillance Networks. Clin Infect Dis. 2023;76:e 1047–53. 10.1093/cid/ciac 56135797157 PMC 9907489 · doi ↗ · pubmed ↗
- 2World Health Organization. Diarrhoeal disease. Key facts. 2024. Available: https://www.who.int/news-room/fact-sheets/detail/diarrhoeal-disease. Accessed: 17 April 2025.
- 3Fagbamigbe AF Uthman AO Ibisomi L Hierarchical disentanglement of contextual from compositional risk factors of diarrhoea among under-five children in low- and middle-income countries. Sci Rep. 2021;11:8564. 10.1038/s 41598-021-87889-233879839 PMC 8058334 · doi ↗ · pubmed ↗
- 4Wolf J Hubbard S Brauer M Ambelu A Arnold BF Bain R Effectiveness of interventions to improve drinking water, sanitation, and handwashing with soap on risk of diarrhoeal disease in children in low-income and middle-income settings: a systematic review and meta-analysis. Lancet. 2022;400:48–59. 10.1016/S 0140-6736(22)00937-035780792 PMC 9251635 · doi ↗ · pubmed ↗
- 5Bradley SEK Rosapep L Shiras T Where Do Caregivers Take Their Sick Children for Care? An Analysis of Care Seeking and Equity in 24 USAID Priority Countries. Glob Health Sci Pract. 2020;8:518–33. 10.9745/GHSP-D-20-0011533008861 PMC 7541105 · doi ↗ · pubmed ↗
- 6World Health Organization. Health topics: Diarrhoea. 2024. Available: https://www.who.int/health-topics/diarrhoea#tab=tab_1. Accessed: 17 April 2025.
- 7Bogler L Weber AC Ntambi J Simen-Kapeu A Zagre NM Ekpini RE Health-care seeking for childhood diseases by parental age in Western and Central Africa between 1995 and 2017: A descriptive analysis using DHS and MICS from 23 low- and middle-income countries. J Glob Health. 2021;11:13010. 10.7189/jogh.11.1301034484717 PMC 8397328 · doi ↗ · pubmed ↗
- 8Harb A Abraham SO’Dea M Hantosh HA Jordan D Habib I Sociodemographic Determinants of Healthcare-Seeking Options and Alternative Management Practices of Childhood Diarrheal Illness: A Household Survey among Mothers in Iraq. Am J Trop Med Hyg. 2020;104:748–55. 10.4269/ajtmh.20-052933289474 PMC 7866356 · doi ↗ · pubmed ↗