Left ventricular abscess with native mitral valve endocarditis diagnosed by cardiac computed tomography
Ryosuke Honda, Yuya Masuda, Shoichi Matsukage, Akiyoshi Ogimoto

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
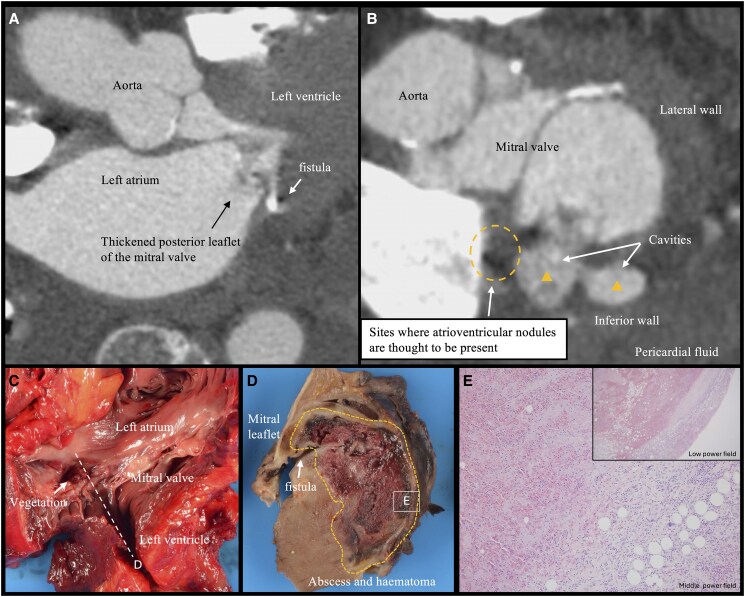 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsInfective Endocarditis Diagnosis and Management · Cardiac Structural Anomalies and Repair · Cardiac Valve Diseases and Treatments
Case description
An 87-year-old woman with a history of Type 2 diabetes mellitus was admitted with fever. During her hospitalization, she developed cerebellar infarction and complete atrioventricular block. Transthoracic echocardiography (TTE) revealed a mobile structure on the posterior leaflet of the mitral valve (MV). As transoesophageal echocardiography was contraindicated due to dyspnoea, a cardiac computed tomography (CT) was performed. It demonstrated thickened leaflet of the MV and cavities within the inferior-posterior wall of the left ventricle (Figure 1). Blood cultures identified Staphylococcus aureus. The heart team recommended cardiac surgery, but the patient declined due to advanced age. Palliative care was initiated, with bedside follow-up conducted through TTE. She succumbed to her illness on the 12th day of hospitalization.
Cardiac computed tomography revealed thickened posterior leaflet of the mitral valve and an abscess within the left ventricular posterior wall in the long-axis view (A) and short-axis view (B). Gross examination of the left heart (C and D) demonstrated fistula formation in the lower portion of the posterior apex of the mitral valve and an abscess in the posterior wall. Haematoxylin and eosin staining of the left ventricular free wall (E) showed evidence of necrosis and inflammatory infiltration into the myocardial tissue, without clear rupture of the left ventricular wall.
Autopsy revealed a 16 × 9 mm vegetation confined to the posterior leaflet of the MV, accompanied by a left ventricular posterior wall abscess with inflammatory cell infiltration extending to the surrounding tissue, including the atrioventricular node (Figure 1). We hypothesized that inflammatory spillover into the conduction system resulted in severe atrioventricular block, while spillover into the pericardial space led to cardiac tamponade.
While transoesophageal echocardiography is strongly recommended for the diagnosis of extravalvular complications of infective endocarditis, it is difficult to perform in high-risk patients in the acute phase.^1,2^ In this case, cardiac CT a high-sensitivity, non-invasive, and rapid modality effectively overcame this limitation and provided an accurate diagnosis.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Delgado V, Ajmone Marsan N, de Waha S, Bonaros N, Brida M, Burri H, et al 2023 ESC guidelines for the management of endocarditis. Eur Heart J 2023;44:3948–4042.37622656 10.1093/eurheartj/ehad 193 · doi ↗ · pubmed ↗
- 2Wang A, Gaca JG, Chu VH. Management considerations in infective endocarditis: a review. JAMA 2018;320:72–83.29971402 10.1001/jama.2018.7596 · doi ↗ · pubmed ↗