Familial non-inflammatory, non-atherosclerotic vasculopathy presented with acute coronary syndrome
Hikaru Masuda, Riku Arai, Yuki Nakajima, Yutaka Koyama, Nobuhiro Murata, Yasuo Okumura, Masashi Tanaka, Hiroyuki Hao

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
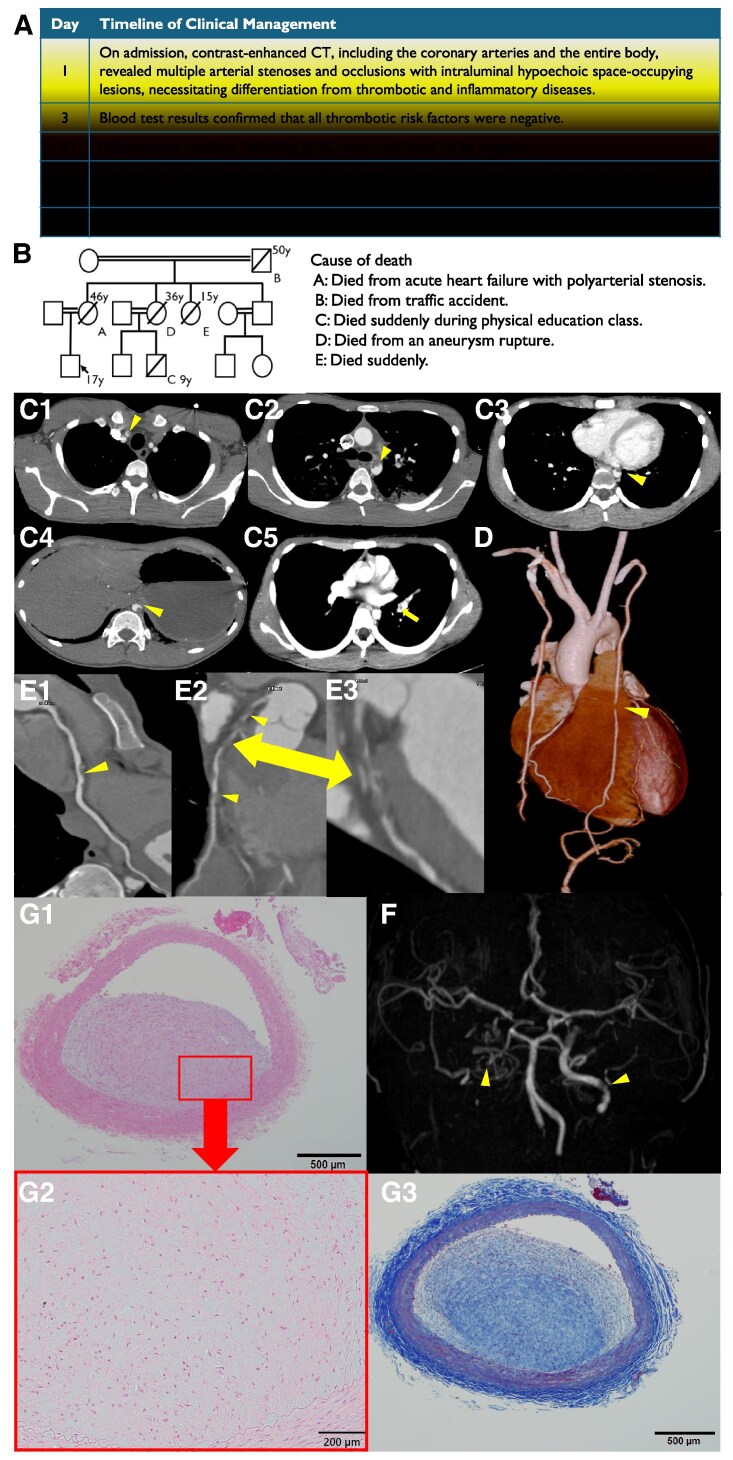 Figure 1
Figure 1 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAtherosclerosis and Cardiovascular Diseases · Cell Adhesion Molecules Research · Protein Tyrosine Phosphatases
A 17-year-old male presented to our hospital after experiencing transient loss of consciousness during exercise. Elevated cardiac markers and ST-segment changes on the electrocardiogram led to a diagnosis of non-ST elevation myocardial infarction (Figure 1, A). His family history revealed multiple sudden deaths due to cardiovascular causes (Figure 1, B). His renal, hepatic, and lipidic profiles were within normal limits. Enhanced whole-trunk computed tomography and magnetic resonance angiography revealed multiple vascular stenoses in brachiocephalic artery (Figure 1, C1), aortic arch (Figure 1, C2), descending aorta (Figure 1, C3), abdominal aorta (Figure 1, C4), left pulmonary artery (Figure 1, C5), left internal thoracic artery (LITA) (Figure 1, D), mid-right coronary artery (Figure 1, E1), left main trunk, proximal and mid-left anterior descending artery (Figure 1, E2, E3), and bilateral internal carotid arteries (Figure 1, F). Blood tests showed no evidence of inflammatory, collagen, coagulation or malignant disorders and genetic tests account for hereditary conditions such as PHACTR1, RNF213 were negative, so we ruled out active inflammatory or thrombotic diseases. Coronary artery bypass graft surgery was performed using the left and right internal thoracic arteries as free grafts, along with saphenous vein grafts. The stenotic lesion of the LITA was resected and submitted for pathological examination, while a healthy segment was used as the graft. Warfarin and aspirin were prescribed for post-operative medication. Pathological examination of LITA revealed non-inflammatory, non-atherosclerotic, and non-thrombotic lesions characterized by collagen and smooth muscle cell proliferation, suggesting intimal fibromuscular dysplasia (FMD) in Hematoxylin–Eosin stain (Figure 1, G1, G2) and Masson trichrome stain (Figure 1, G3).
This case was ultimately diagnosed as acute myocardial infarction caused by the intimal FMD.