Prediction of Positive Angiogram Using Enhanced Computed Tomography in Postpartum Hemorrhage: A Retrospective Multicentered Study
Makoto Aoki, Hiroyuki Tokue, Hisao Yajima, Masazumi Tani, Terutaka Yoshihara

TL;DR
This study shows that enhanced CT scans can accurately predict the need for embolization in postpartum hemorrhage patients.
Contribution
The study demonstrates that CT-detected active arterial hemorrhage is a strong predictor for embolization in postpartum hemorrhage.
Findings
Enhanced CT had 95.6% sensitivity and 98.0% negative predictive value for predicting embolization.
AAH on CT was an independent predictor of embolization (odds ratio=9.31).
Bleeding sites identified on CT included the vagina, intraperitoneal, and abdominal wall.
Abstract
Aim: This study aimed to determine the accuracy of active arterial hemorrhage (AAH) on computed tomography (CT) in predicting the need for embolization in postpartum hemorrhage (PPH). Methods: In a multicentered retrospective observational study, we reviewed the medical records of PPH patients between April 2010 and May 2020. We included patients who initially underwent enhanced CT and were subsequently classified as AAH+ or AAH- on CT. AAH+ on angiogram and embolization was used as a positive reference standard. A multiple logistic regression model evaluated AAH on CT as a predictor for embolization. We assessed AAH+ on CT supplied by extrauterine arteries. Results: Of 231 PPH patients, 94 underwent enhanced CT. AAH+ and AAH- on CT consisted of 44 and 50 patients, respectively. Of AAH+ on CT patients, 32 (72.7%) underwent angiography and embolization. The sensitivity, specificity,…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
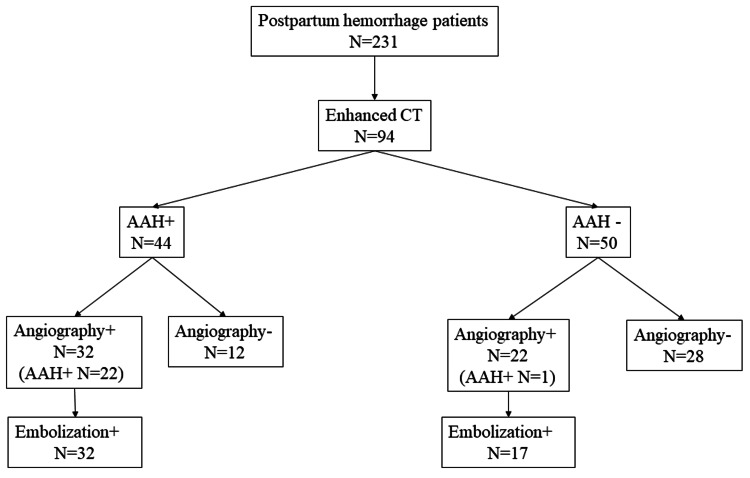 Figure 1
Figure 1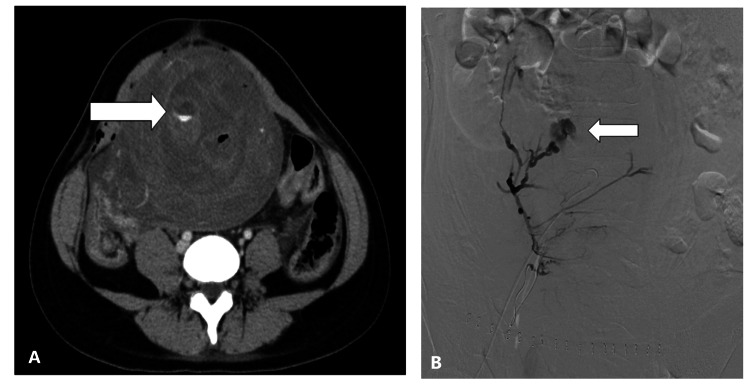 Figure 2
Figure 2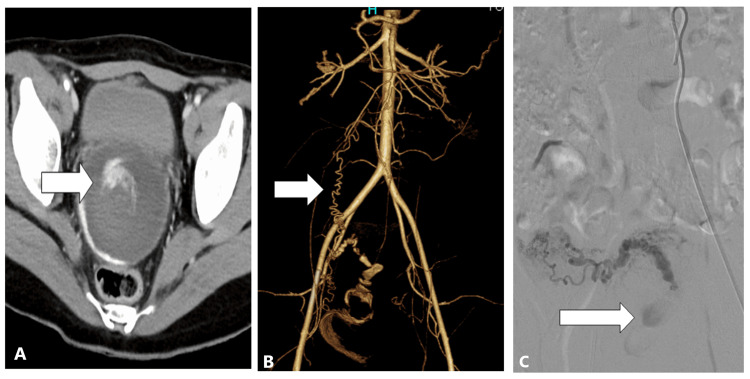 Figure 3
Figure 3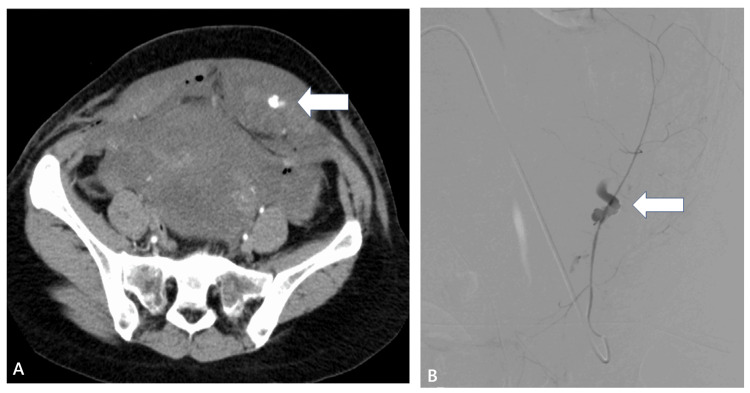 Figure 4
Figure 4| Variables | AAH+ on CT, n=44 | AAH- on CT, n=50 | p-Value |
| Demographics | |||
| Age, years (median) | 33 (31-35) | 34 (30-36) | 0.96 |
| Mode of conception, n (%) | |||
| Spontaneous | 32 (76.2) | 31 (64.6) | 0.25 |
| Assisted reproductive technology | 10 (23.8) | 17 (35.4) | |
| Parity, n (%) | |||
| Primiparous | 23 (52.3) | 28 (56.0) | 0.83 |
| Multiparous | 21 (47.7) | 22 (44.0) | |
| Previous normal vaginal delivery | 17 (80.9) | 17 (77.2) | 1.00 |
| Previous cesarean section | 4 (19.0) | 5 (22.7) | 1.00 |
| Gestational weeks at delivery, week, median (IQR) | 39 (36-40) | 39 (36-40) | 0.60 |
| Mode of delivery, n (%) | |||
| Normal vaginal delivery | 32 (72.7) | 41 (82.0) | 0.32 |
| Cesarean delivery | 12 (27.3) | 9 (18.0) | |
| Interval between delivery and postpartum hemorrhage | |||
| Primary PPH | 27 (61.4) | 28 (56.0) | 0.67 |
| Secondary PPH | 17 (38.6) | 22 (41.5) | |
| Cause of PPH, n (%) | |||
| Atony | 11 (25.0) | 12 (25.0) | 0.41 |
| Placenta accreta | 1 (2.3) | 1 (2.0) | |
| Remnant placenta | 14 (31.8) | 23 (47.9) | |
| Placenta previa | 1 (2.3) | 1 (2.1) | |
| Trauma | 7 (15.9) | 7 (14.6) | |
| Uterus artery aneurysm or AVM | 7 (15.9) | 4 (8.3) | |
| Placental abruption | 3 (6.8) | 0 (0) | |
| Vital signs | |||
| sBP (mmHg) median (IQR) | 117 (100-135) | 112 (103-125) | 0.49 |
| HR (bpm) median (IQR) | 100 (86-117) | 96 (86-110) | 0.71 |
| Shock index, median (IQR) | 0.89 (0.68-1.10) | 0.86 (0.70-1.06) | 0.98 |
| Hemodynamic instability in clinical course, n (%) | 21 (47.7) | 17 (34.0) | 0.20 |
| Laboratory results | |||
| Hemoglobin values (g/dL) median (IQR) | 8.2 (6.0-9.7) | 8.0 (6.5-9.5) | 0.81 |
| Coagulopathy | 18 (40.9) | 4 (8.0) | <0.01 |
| Fibrinogen levels (mg/dL) median (IQR) | 186 (91-256) | 256 (194-297) | <0.01 |
| Outcomes | AAH+ on CT, n=44 | AAH- on CT, n=50 | p-Value |
| CT findings, n (%) | |||
| Ovarian artery visualization | 18 (41.9) | 11 (22.4) | 0.07 |
| Sites of AAH on CT | |||
| Intrauterine | 31 (70.4) | NA | - |
| Vagina | 7 (15.9) | NA | - |
| Intraperitoneal | 3 (6.8) | NA | - |
| Abdominal wall | 3 (6.8) | NA | - |
| Angiography | 32 (72.7) | 22 (44.0) | <0.01 |
| AAH on angiogram | 22 (68.8) | 1 (2.0) | <0.01 |
| Sites of extravasation on angiogram | |||
| Intrauterine | 17 (77.3) | 1 (100.0) | 1.00 |
| Vagina | 2 (9.1) | 0 (0) | |
| Intraperitoneal | 2 (9.1) | 0 (0) | |
| Abdominal wall | 1 (4.5) | 0 (0) | |
| Angioembolization | 32 (72.7) | 17 (34.0) | <0.01 |
| Quantity of blood transfusion | |||
| Red blood cells, units | 8 (4-12) | 4 (2-6) | 0.01 |
| Hospital length of stay | 8 (6-11) | 8 (6-9) | 0.27 |
| Hysterectomy | 1 (2.3) | 1 (2.0) | 1.00 |
| Variables | AAH on angiogram and required embolization | No angiogram required or negative angiogram |
| AAH+ on CT (n) | True positive (22) | False positive (22) |
| AAH- on CT (n) | False negative (1) | True negative (49) |
| Types of PPH | AAH on angiogram and required embolization | No angiogram required or negative angiogram | |
| Primary | AAH+ on CT (n), n=27 | True positive (10) | False positive (17) |
| AAH- on CT (n), n=28 | False negative (1) | True negative (27) | |
| Secondary | AAH+ on CT (n), n=17 | True positive (12) | False positive (5) |
| AAH- on CT (n), n=22 | False negative (0) | True negative (22) | |
| Variables | OR | CI | p-Value |
| Age | 1.02 | 0.91-1.14 | 0.70 |
| Secondary PPH | 8.00 | 2.41-26.60 | <0.01 |
| Hemodynamic instability | 3.75 | 1.18-11.90 | 0.02 |
| Coagulopathy | 0.47 | 0.12-1.82 | 0.27 |
| AAH on CT | 9.31 | 2.85-30.50 | <0.01 |
| Variables | AAH+, n=32 | AAH-, n=17 | p-Value |
| Embolized arteries | |||
| Uterine arteries | 28 (87.5) | 16 (94.1) | 1.00 |
| Bilateral UAs | 25 (78.1) | 16 (94.1) | 0.23 |
| Unilateral UA | 3 (9.4) | 0 (0) | 0.54 |
| Extrauterine arteries | 10 (31.2) | 2 (11.8) | 0.17 |
| OA | 4 (12.5) | 1 (5.9) | 0.65 |
| IPA | 3 (9.4) | 1 (5.9) | 1.00 |
| IIA | 1 (3.1) | 0 (0) | 1.00 |
| VA | 1 (3.1) | 0 (0) | 1.00 |
| IEA | 1 (3.1) | 0 (0) | 1.00 |
| Embolic materials | |||
| Geratin | 27 (87.1) | 17 (100.0) | 0.28 |
| NBCA | 4 (12.9) | 0 (0.0) | |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsMaternal and fetal healthcare · Traumatic Brain Injury and Neurovascular Disturbances · Trauma and Emergency Care Studies
Introduction
Postpartum hemorrhage (PPH) is a life-threatening condition that is the most important cause of maternal death worldwide [1,2]. A delay in diagnosis and appropriate treatment for PPH is associated with maternal death [3,4]. Therefore, the immediate detection and localization of the bleeding site is vital for rescuing patients with severe PPH [5].
Uterine artery embolization (UAE) has been the standard treatment option for PPH because of its low invasiveness and high success rate [6,7]. However, the following two unresolved problems exist with UAE: first, which patients with PPH should undergo angiography is still debated. Angiography is indicated for patients with PPH who are unresponsive to initial management and in whom specific causes of PPH, such as uterine atony-resistant uterotonics, cervico-uterine hemorrhage, vaginal thrombus or inaccessible to any surgical procedure; however, an accurate and appropriate indication was undetermined [8,9]. Second, PPH may involve active arterial bleeding, except for uterine arteries, and conventional angiography may yield limited information regarding extrauterine bleeding from ovarian and inferior epigastric arteries, as well as the peripheral branches of the internal iliac artery [10,11].
Recently, enhanced computed tomography (CT) was shown to be useful in identifying candidates for angiography and detecting the location of postpartum hemorrhage [8,12-14]. Active arterial hemorrhage (AAH) on CT was an indicator for UAE and the site of the AAH determined which artery needed to be embolized. While negative angiograms may occur in patients with AAH on CT, and because UAE has defined complications, further information is needed as to when angiography should follow the recognition of AAH on CT in patients with PPH.
How often AAH on CT will yield a positive angiogram and the need for embolization is lacking in the literature. Therefore, we evaluated the predictivity of AAH on CT for a positive angiogram and embolization in patients with PPH. Our hypothesis was that AAH on CT had a high sensitivity and positive predictive value; however, the specificity and negative predictive value may be low. Patients with PPH have to undergo UAE because of the other aforementioned clinical characteristics, and we additionally developed a multiple regression model to assess the independent effect of AAH on CT for embolization.
Materials and methods
Study design and patient selection
A multicentered, retrospective, observational study was performed. All methods were performed in accordance with the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines. Three emergency and perinatal medical centers contributed retrospectively and collected clinical imaging data. All participating hospitals had similar availabilities of CT-scanning and interventional radiology, and similar qualities of patient treatment. The study protocol was approved by the Institutional Review Board of Gunma University Hospital (#HS2021-058), with informed consent waived. Data-use agreements were executed between each institution and the host institution. The medical records of patients with PPH in these hospitals between April 2010 and May 2020 were reviewed.
Variables collected for the analysis were patient demographics, mode of conception, parity, gestational weeks at delivery, mode of delivery, types of PPH regarding interval between delivery and PPH, cause of PPH, vital signs at hospital arrival and hemodynamic instability during clinical course, laboratory results, and findings of an enhanced CT and an angiogram. Primary PPH was defined as PPH within 24 hours after delivery, and secondary PPH was defined as PPH from 24 hours to 12 weeks after delivery [8]. Hemodynamic instability was defined as systolic blood pressure <90 mmHg or shock index >1.0 during the clinical course. Coagulopathy by laboratory results was defined as a platelet count <50000/μL, prothrombin time-international normalized ratio of >2.0, or fibrinogen <150 mg/dL. Patients with PPH who underwent an initial enhanced CT examination were included. Positive findings of enhanced CT or angiogram were defined as active arterial hemorrhage (AAH) including arterial extravasation, pseudoaneurysm, or vessel interruption. Our study patients were divided into two groups according to the presence or absence of AAH on enhanced CT (AAH+ or AAH- on CT).
Multidisciplinary approach for PPH
Conventional medical treatments for PPH, including fluid resuscitation, blood transfusion, uterine massage, and administration of uterotonic drugs, were performed using a multidisciplinary approach by obstetricians, emergency physicians, anesthesiologists, and an interventional radiologist [2]. Enhanced CT examinations, angiography, and embolization were performed at the discretion of the multidisciplinary team.
Enhanced CT technique and interpretation
In the emergency department at participating hospitals, CT examinations were performed with a 64-slice multi-detector CT scanner. Dynamic phase CT was performed in the plain, arterial, and portal venous phases. Monitor scanning was initiated 10 s after the start of contrast media. Breath-hold dual-phase diagnostic scanning was performed 10 s (arterial phase) and 110 s (portal venous phase) after aortic enhancement in monitoring images that reached bolus-tracking threshold attenuation (220 HU). Active arterial hemorrhage on CT was defined as extravascular high-attenuating regions with attenuation similar to or greater than that of the aorta on arterial phase images and was analyzed by at least one radiologist. The site of AAH on CT was classified into four regions as follows: uterine body, vagina, intraperitoneal (extrauterine), and abdominal wall. Whether AAH was present on enhanced CT images was recorded for a total of four locations for each patient. Additionally, we corrected information on the visualization of the ovarian artery in the arterial phase during enhanced CT. Visualization of the ovarian artery was defined as obvious blood flow from the ovarian artery to the uterus and confirmed by two independent interventional radiologists.
Details of angiography and embolization
Angiography was performed on patients with unstable hemodynamics, AAH on enhanced CT, and/or continuous vaginal bleeding. A 5-Fr sheath was inserted into the right common femoral artery. First, the initial aortography was performed at the level of renal arteries with a 4-Fr pigtail catheter (Gifu, Japan: Terumo Clinical Supply Co. Ltd.) to identify the uterine artery and/or other potential bleeding sites. Regarding AAH+ on CT patients, we first tried to embolize any suspected bleeding artery and subsequently embolized bilateral uterine arteries if a patient’s vital signs did not improve or vaginal bleeding did not cease after embolization of the suspected bleeding artery. For AAH- on CT patients, bilateral uterine arteries were basically selected and embolized. A 5-Fr Cobra catheter (Tokyo, Japan: Medikit Co. Ltd.) was introduced over a 0.035-inch guidewire (Gifu, Japan: Terumo Clinical Supply Co., Ltd.) to assess internal iliac arteries and their branches, such as uterine arteries. Bilateral uterine arteries were selected with a 5-Fr Cobra catheter or a microcatheter (Estream 2.0; Tokyo, Japan: Toray Medical Co. Ltd.) and embolized with gelatin sponge particles (Serescue; Tokyo, Japan: Nippon Kayaku Co. Ltd.). We basically used absorbable and nonpermanent embolic materials. After completing the embolization of uterine arteries, we again performed aortography to search for other bleeding arteries such as ovarian arteries, inferior epigastric arteries, internal pudendal arteries, and vaginal arteries. Ovarian artery embolization was performed based on the physiological findings of the patient and radiological findings [2]. When the cessation of bleeding on the post-embolization angiogram and cessation of vaginal bleeding at speculum inspection, performed immediately after embolization, were confirmed, an angiography procedure was completed.
Statistical analysis
Continuous variables were reported as medians with interquartile ranges, and categorical variables were reported as counts with percentages. Basic and maternal characteristics were compared between AAH+ and AAH- on CT groups. Chi-squared and Mann-Whitney U tests were used for categorical and continuous variables, respectively. First, we calculated the sensitivity, specificity, and positive (PPV) and negative predictive values (NPV) of AAH on CT for AAH on angiogram. Embolization was set as the reference standard. Additionally, we calculated the predictivity of AAH on CT for AAH on angiogram and embolization between primary and secondary PPH. Second, a multiple logistic regression model was created to assess the independent effect of AAH on CT for embolization. Adjusted confounders were selected according to scientific rationale; age, types of PPH, and coagulopathy were selected. Third, we performed univariate analysis of outcomes between AAH+ and AAH- on CT. The following outcomes were evaluated: ovarian artery visualization on CT findings, sites of AAH on CT, sites of AAH on angiogram, quantity of blood transfusion, hospital length of stay, and hysterectomy rates. Finally, we descriptively examined embolized arteries and embolic materials between AAH+ and AAH- on CT. Statistical significance was defined as two-sided p<0.05 or assessed using a 95% confidence interval (CI). All statistical analyses were performed using R software version 4.0.5 (Vienna, Austria: R Foundation for Statistical Computing).
Results
A total of 231 patients with PPH were enrolled during the study period. Of these, 94 patients underwent dynamic enhanced CT at initial evaluation. The number of AAH+ and AAH- patients on CT was 44 and 50, respectively (Figure 1). The characteristics of these two groups are compared in Table 1.
Patient clinical course and flowchart.AAH: active arterial hemorrhage; CT: computed tomography
Table 1: Clinical characteristics of AAH+ and AAH- patients on CT.AAH: active arterial hemorrhage; AVM: arterio-venous malformation; CT: computed tomography; HR: heart rate; IQR: interquartile range; PPH: postpartum hemorrhage; sBP: systolic blood pressureHemodynamic instability in the clinical course was defined as sBP <90 mmHg or shock index >1. Coagulopathy was defined as a platelet count of <50000/μL, prothrombin time-international normalized ratio of >2.0, or fibrinogen <150 mg/dL.
Spontaneous conception was 67.0% (63/94), and primiparous was 54.2% (51/94). Cesarean delivery for conception accounted for 22.3% (21/94). Primary PPH and secondary PPH were approximately 60% and 40%, respectively. Causes of PPH included the following: remnant placenta (39.3%), atony (24.4%), and trauma including vaginal or perineal laceration (14.8%), in descending order. Angiography was performed in 54 patients (57.4%) and embolization was performed in 49 patients (52.1%). Four patients required vaginal sutures for trauma and two patients underwent hysterectomy.
No significant difference between the two groups was observed in terms of the following: demographics, mode of conception, parity, mode of delivery, and cause of PPH. Additionally, vital signs on hospital arrival and the proportions of hemodynamic instability in clinical course did not significantly differ between the two groups. Regarding laboratory results, patients in the AAH+ on CT group had significantly more coagulopathy (40.9% vs. 8.0% between AAH+ and AAH- on CT), and fibrinogen values were significantly lower in the AAH+ on CT group (p<0.01). Univariate analyses of outcomes are shown in Table 2.
The AAH+ on CT group of patients showed significantly more AAH on angiogram (68.8% vs. 4.5%; p<0.01) and underwent significantly more embolization (72.7% vs. 34.0%; p<0.01) compared with patients of the AAH- on CT group. The sensitivity, specificity, PPV, and NPV of AAH on CT were 95.6%, 69.0%, 50.0%, and 98.0%, respectively (Table 3). Additionally, specificity and PPV were higher in secondary PPH (Table 4).
A multiple logistic regression model showed secondary PPH (odds ratio {OR}=8.00; 95% CI=2.41-26.60; p<0.01), hemodynamic instability during clinical course (OR=3.75; 95% CI=1.18-11.90; p=0.02) and AAH+ on CT (OR=9.31, 95% CI=2.85-30.50, p<0.01) were independent predictors of angioembolization (Table 5).
The ovarian artery was more visualized on enhanced CT in the AAH+ compared with AAH- on CT group (41.9% vs. 22.4%; p=0.07). Sites of AAH on CT were the intrauterine (70.5%), vagina (15.9%), intraperitoneal location (6.8%), and abdominal wall (6.8%), respectively (Table 2, Figures 2A, 2B, 3A-3C, 4A, 4B).
Radiologic images of a 25-year-old woman with bleeding within 24 hours after vaginal delivery.(A) A contrast-enhanced CT image shows active contrast extravasation in the uterus (arrow). (B) A right uterine arteriogram shows active contrast extravasation from the right uterine artery (arrow).
CT, CTA, and ovarian arteriogram of 23-year-old woman with postpartum bleeding within 24 hours of vaginal delivery.(A) A contrast-enhanced CT image shows active contrast extravasation in the uterus (arrow). (B) A computed tomography angiogram reveals a visible right ovarian artery (arrow). (C) A right ovarian arteriogram shows active contrast extravasation from the right ovarian artery (arrow).
Radiologic images 38-year-old woman with bleeding within 24 hours after a cesarean delivery.(A) A contrast-enhanced CT shows active contrast extravasation in the left abdominal wall (arrow). (B) A left inferior epigastric artery angiogram shows active contrast extravasation in the abdominal wall (arrow).
AAH on angiogram was confirmed in the intrauterine (78.2%), vagina (8.6%), intraperitoneal location (8.6%), and abdominal wall (4.3%). The median quantity of red blood cells transfused was significantly higher in patients of the AAH+ on the CT group (8 {4-12} units vs. 4 {2-6} units; p=0.01). The hospital length of stay and hysterectomy rates did not significantly differ between the groups. Details of embolized arteries and embolic materials are shown in Table 6. AAH+ on CT patients tended to have other arteries embolized except for uterine arteries (31.2% vs. 11.8%; p=0.17).
Discussion
The findings from this study are as follows: (1) the sensitivity and NPV of AAH in CT group of patients were high (95.6% and 98.0%, respectively) while the specificity and PPV were low (69.0% and 50.0%, respectively). (2) A multiple logistic regression model showed that AAH on CT was an independent predictor of angioembolization. (3) Enhanced CT revealed the blood supply from extrauterine arteries. The high sensitivity and NPV of an AAH on CT were similar to previous literature [8,15].
Previous literature from Japan demonstrated high sensitivity (100%) and NPV (100%) to detect AAH on angiograms [15]. Additionally, literature from Korea showed that AAH on CT had a high sensitivity (100%) in detecting location-based AAH on angiograms. However, both studies were single-centered retrospective studies and the number of cases was small, therefore, their general validity was low.
The specificity and PPV were low compared with high sensitivity and NPV for patients in the AAH on CT group. The values of specificity and PPV in this study were also found to be similar to previous literature (specificity 28.6% and PPV 75%) [15]. On the other hand, the specificity and PPV were not so high compared with sensitivity and NPV. This was because the quality of CT examinations had improved over time, and the visualization of minor AAH on CT was enhanced [15]. Additionally, even if AAH+ on CT was confirmed, such patients did not have to undergo an angiogram and embolization. Especially in primary PPH patients, the PPV was low, and hemostasis could be achieved without embolization.
We additionally developed a multiple logistic regression model. The predictors for UAE were secondary PPH, hemodynamic instability, and AAH on CT. This result meant the significance of AAH on CT differed according to the existence of a primary or secondary PPH. The specificity and positive predictive value were higher in secondary PPH (Table 4). Regarding secondary PPH, the major causes for this were remnant placenta and a uterine artery aneurysm; the evaluation of enhanced CT may be associated with higher predictivity. Additionally, hemodynamic instability during the clinical course was one of the predictors of embolization and if the patients did not have AAH on CT, the patients may subsequently require embolization because of hemodynamic instability.
Finally, we evaluated the efficacy of enhanced CT for determining the supplying extrauterine arteries (Figure 2). Among the AAH+ on CT group of patients, more patients had supply from the ovarian arteries and tended to undergo embolization of an ovarian artery (Figure 3). AAH+ patients on CT underwent embolization of their extrauterine arteries, but this was not statistically significant (Table 6). Reports in the literature similarly described the efficacy of enhanced CT for the localization of AAH in extrauterine arteries such as ovarian arteries, vaginal arteries, or epigastric arteries (Figure 4) [8,13]. The usefulness was reported in the Cardiovascular and Interventional Radiological Society of Europe (CIRSE) standards on practice [14].
The high sensitivity of AAH on CT indicated that if a PPH patient did not have an AAH on CT, the necessity of angiogram and embolization for that patient could be ruled out. Low invasiveness was one of the features of embolization. Complications were not associated with angiography and embolization in this study, while the literature reported that angioembolization may induce procedure-related complications [16,17]. Enhanced CT obviated unnecessary angiogram and embolization, and may contribute to a decreased radiation dose and complications [12]. Considering the low specificity, the information of AAH on CT was not enough to conduct angiography and embolization, especially in primary PPH. As our logistic regression model showed, we may predict a patient requiring an angiogram and embolization by incorporating the information of AAH on CT into clinical practice.
This study has several strengths. First, this was a multicenter study that included a large number of patients giving the rarity of the use of UAE for PPH. To the best of our knowledge, this study was the largest among previous literature that assessed the accuracy of AAH on CT in predicting the need for embolization. Second, the specificity of AAH on CT was not so high and we first created the multivariable logistic regression model. The result showed that AAH on CT was an independent predictor of positive angiogram and embolization. Third, this study’s theme was a common clinical scenario, and the result of this study could be directly connected to clinical practice.
We also acknowledge several limitations to this study. First, this was a retrospective observational study that used hospital medical records of PPH patients at each hospital, and the definition of PPH was not defined in detail. The classical definition of PPH was cumulative blood loss ≥1000 mL, or bleeding associated with signs/symptoms of hypovolemia within 24 hours of the birth process [18]. Considering the definition of PPH, a few patients may not be included in this study. Second, the management of PPH may have differed between institutions. Whether PPH patients undergo enhanced CT or proceed to angiogram without CT was based on institutional protocol. All participating hospitals were emergency and perinatal medical centers, and the proportion without enhanced CT requiring angiogram was only 3.6% (5/137). Therefore, the patients suspected of continuous bleeding underwent enhanced CT, and similar qualities of treatment for PPH were assumed to be guaranteed. Third, unmeasured confounders such as the amount of blood loss and the hemodynamic status during the clinical course existed in multiple logistic regression models, and these confounders may affect the results.
Conclusions
The sensitivity and NPV of the AAH on the CT group of patients were high, and enhanced CT may be useful for identifying PPH patients who require angiography and embolization. Additionally, enhanced CT revealed blood supply from extrauterine arteries, and AAH on CT may serve as a guide for embolization of these arteries. Incorporating AAH on CT into clinical practice may help predict which patients require angiography and embolization.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1ACOG Practice Bulletin: clinical management guidelines for obstetrician-gynecologists number 76, October 2006: postpartum hemorrhage Obstet Gynecol 1039104710820061701248210.1097/00006250-200610000-00046 · doi ↗ · pubmed ↗
- 2Prevalence and risk factors of severe obstetric haemorrhage BJOG Al-Zirqi I Vangen S Forsen L Stray-Pedersen B 1265127211520081871541210.1111/j.1471-0528.2008.01859.x · doi ↗ · pubmed ↗
- 3Transcatheter pelvic arterial embolisation for control of obstetric and gynaecological haemorrhage J Obstet Gynaecol Ratnam LA Gibson M Sandhu C Torrie P Chandraharan E Belli AM 5735792820081900364810.1080/01443610802273374 · doi ↗ · pubmed ↗
- 4Is selective embolization of uterine arteries a safe alternative to hysterectomy in patients with postpartum hemorrhage?AJR Am J Roentgenol Deux JF Bazot M Le Blanche AF 14514917720011141841610.2214/ajr.177.1.1770145 · doi ↗ · pubmed ↗
- 5Uterine artery embolization in the treatment of postpartum uterine hemorrhage J Vasc Interv Radiol Ganguli S Stecker MS Pyne D Baum RA Fan CM 1691762220112118336010.1016/j.jvir.2010.09.031 · doi ↗ · pubmed ↗
- 6Postpartum hemorrhage: guidelines for clinical practice from the French College of Gynaecologists and Obstetricians (CNGOF)Eur J Obstet Gynecol Reprod Biol Sentilhes L Vayssière C Deneux-Tharaux C 122119820162677324310.1016/j.ejogrb.2015.12.012 · doi ↗ · pubmed ↗
- 7Interventional radiology for critical hemorrhage in obstetrics: Japanese Society of Interventional Radiology (JSIR) procedural guidelines Jpn J Radiol Sone M Nakajima Y Woodhams R 2332403320152569433810.1007/s 11604-015-0399-0 · doi ↗ · pubmed ↗
- 8Identification of bleeding sites in patients with postpartum hemorrhage: MDCT compared with angiography AJR Am J Roentgenol Lee NK Kim S Kim CW Lee JW Jeon UB Suh DS 38339019420102009360010.2214/AJR.09.3073 · doi ↗ · pubmed ↗