A Case of Hepatic Encephalopathy With Diffuse Brainstem Signal Changes on Magnetic Resonance Imaging
Hiromu Yurimoto, Taiki Matsubayashi, Isamu Shibata, Misako Furuki, Masato Obayashi

TL;DR
A rare case of liver-related brain changes showed MRI signal changes in the brainstem, which improved with treatment.
Contribution
This case report presents a rare MRI pattern in hepatic encephalopathy with brainstem-specific signal changes and a favorable prognosis.
Findings
MRI showed symmetrical brainstem hyperintensity with DWI and low ADC values in a patient with hepatic encephalopathy.
Brainstem MRI changes resolved within 10 days following branched-chain amino acid therapy.
Hyperintensity on DWI with low ADC values may indicate an acute phase of hepatic encephalopathy.
Abstract
Signal changes on brain MRI have been reported in hepatic encephalopathy; however, no specific findings have been established. Moreover, cases of hepatic encephalopathy presenting with MRI signal changes confined to the brainstem are rare. A 75-year-old woman was admitted to our hospital with a one-day history of impaired consciousness. Blood tests revealed elevated ammonia and gamma-glutamyl transpeptidase levels, along with positive anti-mitochondrial M2 antibodies. Brain MRI on admission demonstrated diffuse and symmetrical hyperintensity in the midbrain and pons on fluid-attenuated inversion recovery (FLAIR) imaging, with corresponding hyperintensity on diffusion-weighted imaging (DWI) and low values on the apparent diffusion coefficient (ADC) map. No signal abnormalities were observed in the globus pallidus on T1-weighted imaging (T1WI). Whole-body CT revealed an irregular hepatic…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
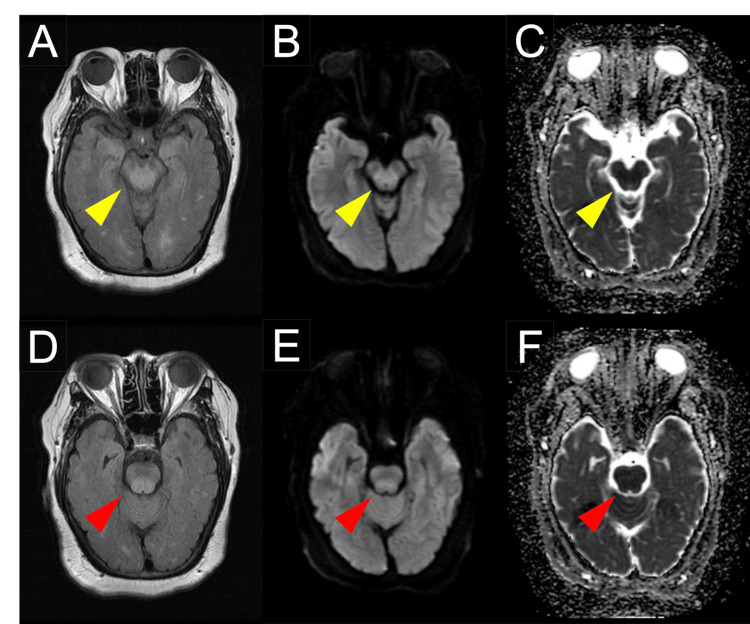 Figure 1
Figure 1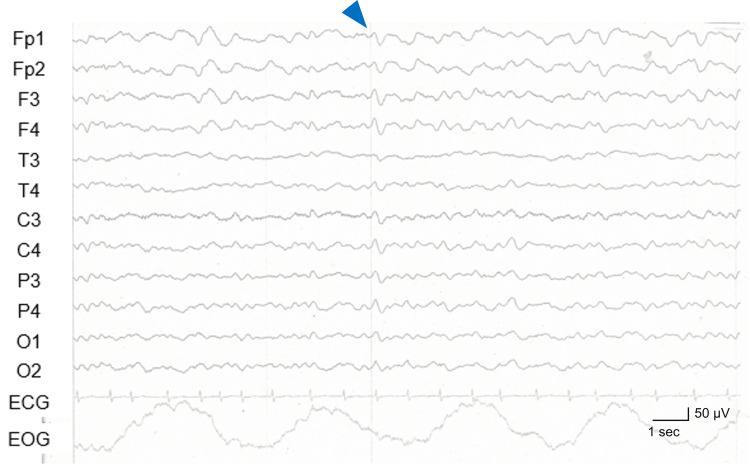 Figure 2
Figure 2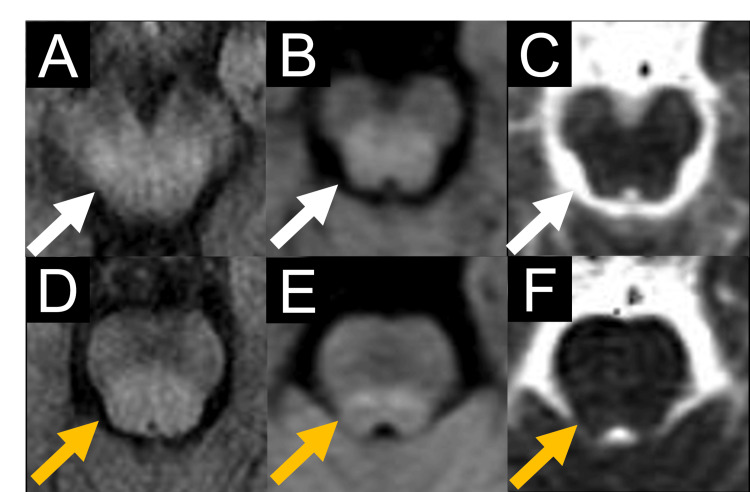 Figure 3
Figure 3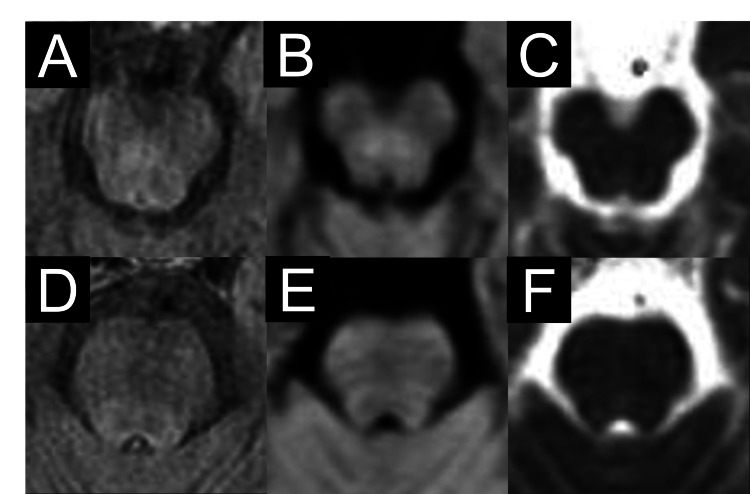 Figure 4
Figure 4| Laboratory parameters | Value (units) | Reference value | |
| Ser | White blood cell | 1,1000/μL | 4,000-10,000 |
| Neutrophils | 64.0% | 40-70 | |
| Hemoglobin | 11.6 g/dL | 11.6-14.8 | |
| Platelet count | 12.7 × 10⁴/μL | 15.8-34.8 × 10⁴ | |
| Prothrombin time | 63% | 70-130 | |
| Albumin | 3.3 g/dL | 4.1-5.1 | |
| Aspartate aminotransferase | 29 U/L | 13-30 | |
| Alanine aminotransferase | 15 U/L | 7-23 | |
| Alkaline phosphatase | 35 U/L | 38-113 | |
| Gamma-glutamyl transpeptidase | 56 U/L | 9-32 | |
| C-Reactive Protein | 0.09 mg/dL | <0.5 | |
| HBs antigen | Negative | Negative | |
| Anti-HCV antibodies | Negative | Negative | |
| Ammonia | 210 µmol/L | 9-47 | |
| Vitamin B1 | 156 ng/mL | 24-66 | |
| Glucose | 99 mg/dL | 73-110 | |
| Anti-mitochondrial M2 antibody | 39.5 U/mL | <7.0 | |
| Anti-nuclear antibody | 1:320 | <1:40 | |
| Immunoglobulin M | 348 mg/dL | 50-269 | |
| Mac-2 binding protein glycosylation isomer | 2.82 | <1.0 | |
| CSF | Color | Clear | - |
| White blood cell | 6/3 μL | 0-15 | |
| Lymphocytes | 83% | 40-80 | |
| Protein | 77.4 mg/dL | 15-45 | |
| Glucose | 59 mg/dL | 50-70 |
| Study | Case | Age/Sex | Cause | NH3 (µmol/L) | Symptoms | MRI | Prognosis | ||||
| Inside of brainstem | Outside of brainstem | ||||||||||
| Hyperintensity areas on FLAIR or T2WI | DWI and ADC* | Hyperintensity areas on FLAIR or T2WI | DWI and ADC* | Outcome | Disease duration | ||||||
| McKinney et al. | 1 | 10/F | AHF after acetaminophen overdose | 104 | Confusion | Bilateral pontine tegmentum | n.a | Thalami | DWI: high | Survived without sequela | 13 days after admission |
| Filipović Grčić P et al. | 2 | 43/M | Liver cirrhosis | 85.6 | Asymmetric upper extremity tremor | Crus cerebri, red nuclei | n.a | Corpus callosum, dentate nucleus, periventricular white matter, internal capsule | n.a | Recovered with mild kinetic and postural tremor of the left hand | 6 months after liver transplantation |
| U-King-Im et al. [ | 3 | 48/M | Fulminant AHF due to acetaminophen overdose | 102 | Impaired consciousness, abnormal posturing, seizures | Midbrain without crus cerebri | n.a | Bilateral temporoparietal lobes, thalami, insular, cingulate cortices | DWI: high | Died | 2 days after admission |
| Our case | 4 | 75/F | Liver cirrhosis due to primary biliary cholangitis | 210 | Impaired consciousness | Bilateral tegmentum of midbrain and pons | DWI: high, ADC: low | None | - | Survived without sequela | 4 days after admission |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsLiver Disease and Transplantation · Liver Disease Diagnosis and Treatment · Infectious Encephalopathies and Encephalitis
Introduction
Hepatic encephalopathy occurs in 30-50% of cirrhotic patients undergoing transjugular intrahepatic portosystemic shunting [1]. Clinically, it presents with altered consciousness and various neuropsychiatric symptoms, including asterixis, delirium, convulsions, and coma [1]. The condition arises due to hepatic dysfunction, which impairs ammonia detoxification via the urea cycle, leading to elevated blood ammonia levels and disrupted neurotransmission in the brain [2]. Typically, compensatory mechanisms are activated to mitigate hyperammonemia; however, conditions such as gastrointestinal bleeding, infection, and constipation can precipitate an acute rise in blood ammonia levels, overwhelming these compensatory pathways [3].
Since hepatic encephalopathy lacks established diagnostic criteria, its diagnosis relies on a comprehensive assessment of clinical factors such as liver cirrhosis, clinical history, and elevated blood ammonia levels [4]. However, grading systems such as the West Haven criteria and the Hepatic Encephalopathy Scoring Algorithm have been proposed to classify its severity [5].
Brain MRI findings in hepatic encephalopathy often include hyperintensity in the globus pallidus on T1-weighted imaging (T1WI), though this is not specific and is also seen in chronic liver injury [6,7]. Other reported findings include hyperintensity along the white matter or corticospinal tract on fluid-attenuated inversion recovery (FLAIR) or T2-weighted imaging (T2WI) and diffuse cortical edema, particularly symmetrically involving the cingulate gyrus and insular cortex [8]. However, definitive MRI markers for hepatic encephalopathy remain unestablished, and cases with isolated brainstem signal changes are rarely recognized.
Here, we present a case of hepatic encephalopathy with a favorable prognosis, characterized by diffuse yet reversible symmetric brainstem signal changes on MRI. This case underscores the importance of considering hepatic encephalopathy in such MRI patterns and suggests that brainstem-limited changes may be associated with a better prognosis.
Case presentation
A 75-year-old woman presented with black stools two days prior and a one-day history of cognitive impairment and decreased consciousness. She was brought to our hospital due to persistent impaired consciousness. Her medical history included postoperative breast cancer with bilateral mastectomy 10 years earlier, hypertension, cellulitis, stasis dermatitis, knee osteoarthritis, and lumbar spondylosis. She had no history of alcohol consumption. On admission, she exhibited a corpulent body, with a height of 159 cm, weight of 120 kg, and BMI of 47.5 kg/m^2^. Physical examination revealed as follows: body temperature, 37.4°C; blood pressure, 165/95 mmHg, heart rate, 76 beats/min; respiratory rate, 16 breaths/min; and oxygen saturation, 100 % on 3 L/min supplemental oxygen. A large amount of tarry stools was observed. Neurological examination revealed impaired consciousness with a Glasgow Coma Scale score of E1V1M4. The light reflex was prompt bilaterally, indicating preserved brainstem reflexes. No motor paralysis or involuntary movements, including convulsions, were noted.
Laboratory findings revealed mild thrombocytopenia, decreased prothrombin time, low albumin levels, and markedly elevated blood ammonia levels (210 µmol/L; reference range: 9-47 µmol/L). An elevated gamma-glutamyl transpeptidase level (56 U/L) was observed. There was no deficiency of vitamin B1 or hyponatremia. Immunological tests revealed positive results for the anti-mitochondrial M2 antibody (39.5 U/mL) and anti-nuclear antibody with speckled pattern and elevated results for immunoglobulin M and mac-2 binding protein glycosylation isomer. A cerebrospinal fluid (CSF) examination showed normal white blood cell count (6/3 µL), slightly elevated protein level (77.4 mg/dL), and normal glucose level. The normal CSF findings, combined with elevated ammonia levels, suggest that the altered consciousness was more likely due to metabolic encephalopathy, including hepatic encephalopathy, rather than meningitis or encephalitis. Laboratory results are summarized in Table 1.
Non-contrast whole-body CT showed an irregular hepatic surface, a blunt liver edge, and splenomegaly, with no evidence of ascites. Findings suggestive of malignancy were not detected on whole-body CT. Brain MRI demonstrated diffuse hyperintensity signals in the brainstem extending from the midbrain to the pons on FLAIR imaging, all symmetrically distributed (Figure 1). The brainstem lesions appeared as hyperintensities on diffusion-weighted imaging (DWI) with corresponding low values on the apparent diffusion coefficient (ADC) map (Figure 1). The symmetrical high signal intensity observed in the medial temporal lobes on DWI and FLAIR was determined to be an artifact. No hyperintensity was observed in the thalamus. The globus pallidus did not exhibit hyperintensity signals on T1WI.
MRI findings on admissionMRI showed hyperintensity in the midbrain tegmentum, sparing the cerebral crus, on FLAIR imaging (A), along with hyperintensity on DWI (B) and low values on the ADC map (C) (yellow arrowheads). Additionally, MRI revealed hyperintensity in the pontine tegmentum on FLAIR (D), with corresponding hyperintensity on DWI (E) and low values on the ADC map (F) (red arrowheads).ADC: Apparent diffusion coefficient; DWI: Diffusion-weighted imaging; FLAIR: Fluid-attenuated inversion recovery
An electroencephalogram (EEG) performed on day 4 after the admission demonstrated slow-wave activity with a basic rhythm of 5-6 Hz and occasional bilaterally synchronous triphasic waves (Figure 2).
EEG findings on day 4 of admissionSlow-wave activity with a basic rhythm of 5-6 Hz and occasional bilaterally synchronous triphasic waves (blue arrowhead) were observed.EEG: Electroencephalogram
Based on the CT findings and laboratory results showing elevated gamma-glutamyl transpeptidase levels and the presence of anti-mitochondrial M2 antibodies, she was diagnosed with liver cirrhosis due to primary biliary cholangitis [9]. The Child-Pugh score was 9 points, corresponding to grade B.
For the treatment of impaired consciousness, intravenous branched-chain amino acids were initiated promptly upon admission due to suspected hepatic encephalopathy. Additionally, acyclovir (1,500 mg/day) and ceftriaxone (2 g/day) were administered simultaneously to address the possibility of an underlying infection. Her consciousness gradually improved after admission, becoming clear by day 4 after admission. She was diagnosed with hepatic encephalopathy based on clinical, laboratory, and imaging findings. Rapid clinical improvement of her altered consciousness with branched-chain amino acid therapy and elevated ammonia levels on laboratory tests were consistent with hepatic encephalopathy. EEG findings of slow waves and triphasic waves, along with the disappearance of brainstem signal changes on MRI following neurological recovery, further supported this diagnosis. Additionally, primary biliary cholangitis with cirrhosis was a plausible underlying condition predisposing her to hepatic encephalopathy. This case was classified as Grade 4 hepatic encephalopathy according to West Haven criteria and the Hepatic Encephalopathy Scoring Algorithm [5]. Blood and CSF cultures were found to be negative. The diagnosis of hepatic encephalopathy led to the discontinuation of acyclovir on day 3 and ceftriaxone on day 5. The abnormal MRI signals in the brainstem persisted until day 3 (Figure 3) but resolved by day 10 (Figure 4). On day 3, the patient exhibited impaired consciousness with a Glasgow Coma Scale score of E4V1M5. However, by day 10, the patient had regained full consciousness. Blood ammonia levels on day 5 decreased compared to the initial laboratory results, measuring 84 µmol/L. Contrast-enhanced brain MRI on day 3 showed no enhancement of the brainstem lesions. She was ultimately discharged on day 11 in stable condition.
MRI findings on day 3 of admissionMRI showed remained hyperintensity in the midbrain tegmentum, sparing the cerebral crus, on FLAIR imaging (A), along with hyperintensity on DWI (B) and low values on the ADC map (C) (white arrows). Furthermore, MRI revealed hyperintensity in the pontine tegmentum on FLAIR (D), with corresponding hyperintensity on DWI (E) and low values on the ADC map (F) (orange arrows).ADC: Apparent diffusion coefficient; DWI: Diffusion-weighted imaging; FLAIR: Fluid-attenuated inversion recovery
MRI findings on day 10 of admissionHyperintensity in the midbrain tegmentum, sparing the cerebral crus, resolved on FLAIR imaging (A), DWI (B), and the ADC map (C). Similarly, hyperintensity in the pontine tegmentum resolved on FLAIR (D), with corresponding resolution of hyperintensity on DWI (E) and low values on the ADC map (F).ADC: Apparent diffusion coefficient; DWI: Diffusion-weighted imaging; FLAIR: Fluid-attenuated inversion recovery
Discussion
We diagnosed a patient with impaired consciousness and diffuse MRI signal changes in the brainstem as having hepatic encephalopathy caused by primary biliary cholangitis. The brainstem reticular formation regulates consciousness, making the brainstem abnormalities observed on MRI a reasonable explanation for the altered consciousness in this case. The resolution of brainstem signal changes on MRI accompanied by the improvement in consciousness further supports the relationship between these MRI findings and the clinical symptoms. Triphasic waves are typically seen in Grade 2-3 hepatic encephalopathy, and the presence of these waves on day 4 may reflect the transitional phase of improvement in this Grade 4 case [1]. The medial temporal lobes, prone to MRI artifacts, showed no changes over time, supporting the conclusion that hyperintensity in this area was an artifact [10]. Tracking signal alterations over time is crucial for distinguishing artifacts from true pathological changes.
Conditions presenting with abnormal signals localized to the brainstem on brain MRI include vascular lesions, demyelinating inflammatory lesions, infectious diseases including infectious rhombencephalitis, neoplastic lesions, and metabolic encephalopathies such as Wernicke’s encephalopathy and central pontine myelinolysis [11]. In this case, the rapid resolution of MRI findings suggested that vascular lesions were unlikely. The improvement of MRI findings without immunotherapy further indicated that demyelinating inflammatory lesions were unlikely. Additionally, the absence of contrast enhancement or mass effect on MRI did not support a neoplastic etiology. Furthermore, negative blood and CSF cultures, along with CSF analysis showing no signs of infection, ruled out infectious causes. Especially, typical MRI features of metabolic encephalopathies include symmetrical signal changes, hyperintensity on DWI, and reversible imaging findings during the clinical course [12,13]. This case exhibited all of these characteristic findings associated with metabolic encephalopathies, supporting the conclusion that the MRI signal changes were attributable to hepatic encephalopathy. There was no deficiency of vitamin B1 or hyponatremia on laboratory tests, making Wernicke's encephalopathy and central pontine myelinolysis unlikely. Consequently, this case highlights the importance of considering hepatic encephalopathy in the differential diagnosis of patients with MRI signal changes confined to the brainstem.
Brain MRI findings in hepatic encephalopathy can be classified into three distinct signal patterns based on the underlying pathological condition: (1) hyperintensity in the globus pallidus and substantia nigra on T1WI, (2) hyperintensity on DWI with corresponding high ADC values, and (3) hyperintensity on DWI with low ADC values [6,14]. In this case, no signal changes were observed in the globus pallidus or substantia nigra on T1WI, nor were there any high-signal lesions on DWI with high ADC values, both of which are typically associated with chronic changes in hepatic encephalopathy [6]. Conversely, the hyperintensity on DWI with low ADC values, observed in this case, suggests acute cellular edema in hepatic encephalopathy, likely caused by the rapid accumulation of glutamate in astrocytes due to ammonia metabolism. This mechanism is considered a hallmark of acute hepatic encephalopathy [6,14]. In this case, the MRI findings suggest acute cellular edema, which likely contributed to the patient's rapidly impaired consciousness. Similar cases with cellular edema changes on MRI have shown acute onset and rapid progression, further supporting the link between these signal changes and the clinical presentation [15].
Notably, to the best of our knowledge, only three cases of hepatic encephalopathy with brainstem signal changes on MRI have been reported with detailed clinical and imaging findings [14,16,17] (Table 2). The distribution of brainstem signal changes in our case differed from those in the previously reported cases and was the most extensive among them. In contrast, two cases (Case 2 and Case 3) that exhibited widespread signal changes beyond the brainstem, including the cerebrum, had poor prognoses, with either prolonged recovery or fatal outcomes. On the other hand, our case, which showed no signal changes outside the brainstem, and Case 1, which exhibited additional signal changes only in the thalamus, demonstrated rapid clinical improvement. A previous cohort study, which included 98 hepatic encephalopathy patients without detailed clinical and imaging information, indicated that hepatic encephalopathy with MRI signal changes confined to the brainstem tends to exhibit a milder clinical course compared to cases with signal changes involving regions outside the brainstem [18]. This finding aligns with our observations in the literature review that hepatic encephalopathy with MRI signal changes confined to the brainstem or a limited region has a favorable prognosis. However, the previous cohort study did not clearly distinguish between acute and chronic MRI change or discuss the extent of lesion localization [18]. Similarly, prior case reports have not differentiated between acute and chronic changes in MRI findings [14,16,17]. Thus, further prospective studies are warranted to investigate the detailed patterns and distribution of MRI signal changes in hepatic encephalopathy, as well as their correlation with clinical prognosis.
This case has a few limitations. First, while continuous EEG monitoring is useful for differentiating epilepsy as a cause of impaired consciousness, our facility was unable to perform this test, and only a single EEG was conducted on day 4. Additionally, polymerase chain reaction (PCR) testing for herpes simplex virus in CSF, which is valuable for excluding herpes encephalitis, was not performed. However, given the multiple findings strongly suggestive of hepatic encephalopathy and the exclusion of other conditions through various tests, we confidently diagnose this case as hepatic encephalopathy.
Conclusions
We diagnosed a patient with hepatic encephalopathy presenting with diffuse MRI signal changes confined to the brainstem. The MRI features in this case, including symmetrical signal changes, hyperintensity on DWI, and reversible imaging findings during the clinical course, supported the diagnosis of metabolic encephalopathy. Hepatic encephalopathy should be considered in patients with brainstem-limited MRI changes. Early diagnosis and intervention are key for improving outcomes. Additionally, the MRI findings in this case showed hyperintensity on DWI with low ADC values, possibly reflecting acute onset and rapid progression. Moreover, the brainstem-restricted signal changes may indicate a favorable prognosis. However, further research is needed to explore the correlation between MRI findings and prognosis in hepatic encephalopathy.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Hepatic encephalopathy N Engl J Med Wijdicks EF 1660167037520162778391610.1056/NEJ Mra 1600561 · doi ↗ · pubmed ↗
- 2Hepatic encephalopathy as a result of ammonia-induced increase in GAB Aergic tone with secondary reduced brain energy metabolism Metab Brain Dis Sørensen M Andersen JV Bjerring PN Vilstrup H 194020243956084410.1007/s 11011-024-01473-x PMC 11576828 · doi ↗ · pubmed ↗
- 3Hepatic encephalopathy: diagnosis and management J Transl Int Med Ridola L Faccioli J Nardelli S Gioia S Riggio O 210219820203351104810.2478/jtim-2020-0034 PMC 7805282 · doi ↗ · pubmed ↗
- 4Hepatic encephalopathy: definition, clinical grading and diagnostic principles Drugs Weissenborn K 597920193070642010.1007/s 40265-018-1018-z PMC 6416238 · doi ↗ · pubmed ↗
- 5Introduction to the Hepatic Encephalopathy Scoring Algorithm (HESA)Dig Dis Sci Hassanein TI Hilsabeck RC Perry W 5295385320081771055110.1007/s 10620-007-9895-0 · doi ↗ · pubmed ↗
- 6MR imaging findings in hepatic encephalopathy AJNR Am J Neuroradiol Rovira A Alonso J Córdoba J 161216212920081858341310.3174/ajnr.A 1139 PMC 8118773 · doi ↗ · pubmed ↗
- 7Hyperintense globus pallidus on T 1-weighted MRI in cirrhotic patients is associated with severity of liver failure Neurology Pujol A Pujol J Graus F 6569431993842391310.1212/wnl.43.1_part_1.65 · doi ↗ · pubmed ↗
- 8Hepatic encephalopathy on magnetic resonance imaging and its uncertain differential diagnoses: a narrative review J Yeungnam Med Sci Lim CG Hahm MH Lee HJ 1361454020233662465410.12701/jyms.2022.00689 PMC 10076915 · doi ↗ · pubmed ↗