Posttraumatic Epidermoid Inclusion Cyst Following Untreated Orbital‐Zygomaticomaxillary Fracture: Case Report
David Kiwango Deoglas, Paulo Joseph Laizer, Shaban Daudi Shaban

TL;DR
A case report shows how an untreated facial injury from a car accident led to a rare cyst forming a year later.
Contribution
This case highlights the delayed complication of an epidermoid cyst following an untreated facial fracture.
Findings
An untreated orbital-zygomaticomaxillary fracture led to an epidermoid inclusion cyst after one year.
The case emphasizes the importance of timely treatment for craniofacial injuries to prevent complications.
Abstract
Timely and comprehensive treatment of craniofacial injuries is essential, as complications may arise, including epidermoid inclusion cysts. We hereby present a case of an orbital epidermoid cyst that developed a year after a patient was involved in a motor vehicle accident and sustained facial injuries that remained untreated.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
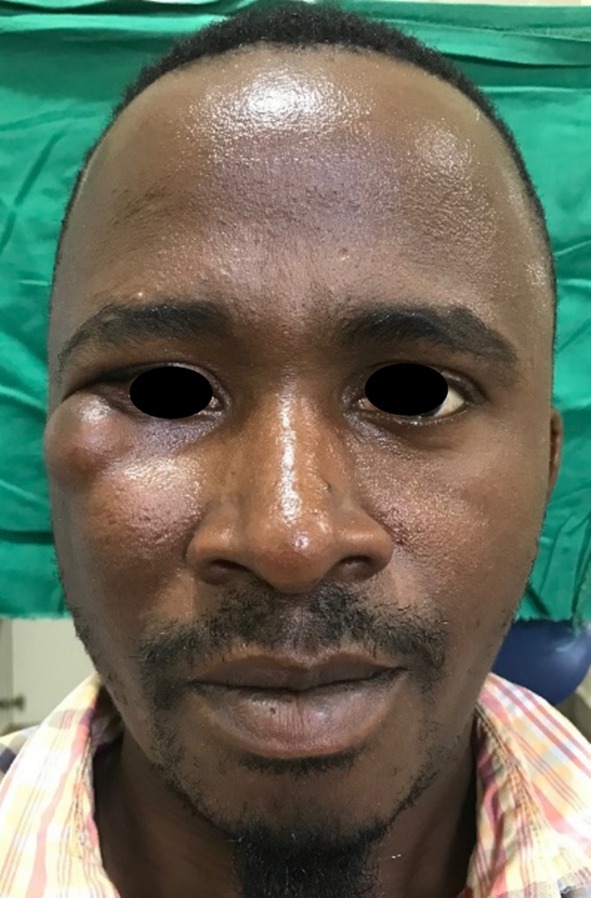 FIGURE 1
FIGURE 1 FIGURE 2
FIGURE 2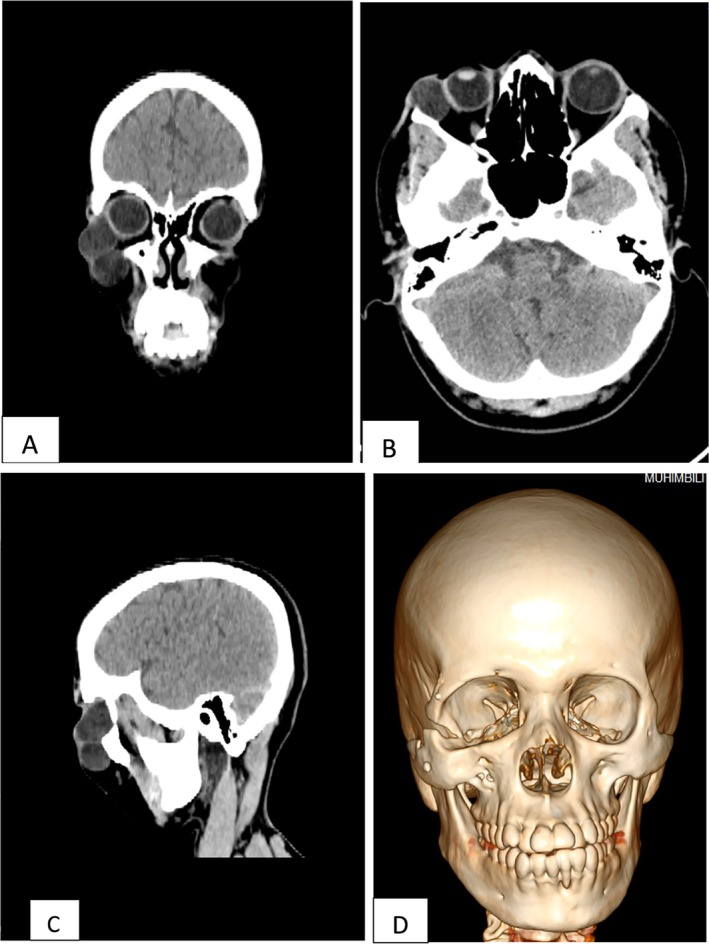 FIGURE 3
FIGURE 3 FIGURE 4
FIGURE 4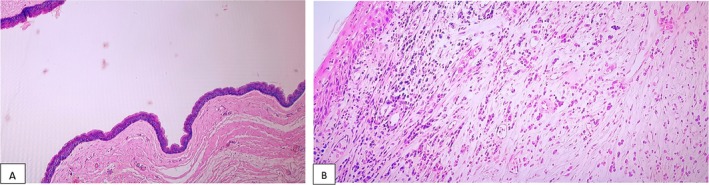 FIGURE 5
FIGURE 5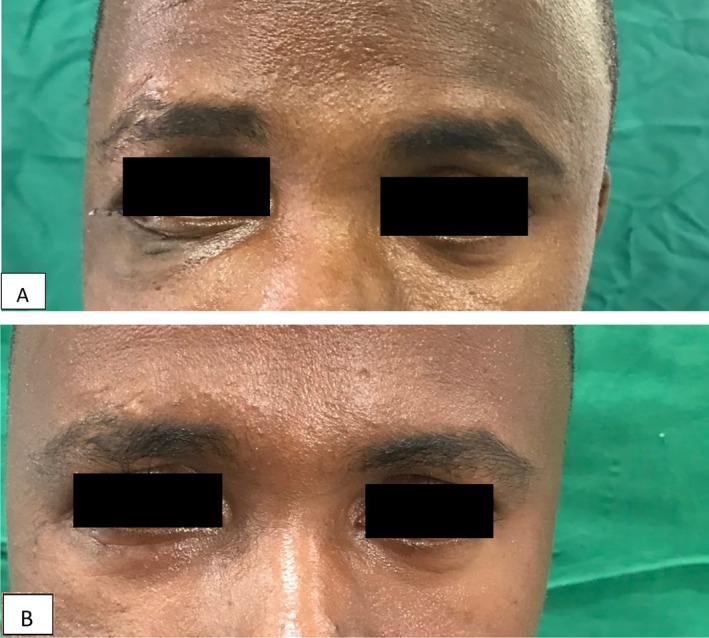 FIGURE 6
FIGURE 6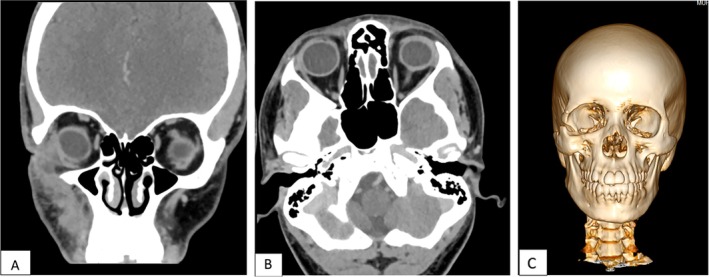 FIGURE 7
FIGURE 7Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsTeratomas and Epidermoid Cysts · Facial Trauma and Fracture Management · Head and Neck Surgical Oncology
Introduction
1
Epidermoid cysts are benign lesions characterized by cystic spaces lined by simple squamous epithelium (epidermoid cyst), containing skin adnexa (“true” dermoid cyst) or tissues of all three germ layers (teratoid cyst) [1]. Head and neck constitute approximately 7% of all cases of epidermoid and dermoid cysts [2]. They can be either primary (congenital) or secondary cysts. Primary lesions are choristomas that involve displacement of epithelial elements during closure of the neural groove or other epithelial fusion lines. Secondary epidermoid cysts result from posttraumatic implantation of surface epithelium into the dermis [2, 3, 4]. Epidermoid inclusion cysts present as a firm, slow‐growing, mobile, painless mass or lump underneath the skin at the subcutaneous‐dermal level, with an intact skin surface with no apparent drainage point. They contain soft, cheesy‐like skin secretions [5]. Epidermoid cysts can be part of features of syndromes like Gardner syndrome, basal‐cell nevus syndrome, and pachyonychia congenita which are associated with facial swellings. Chin, lip, scalp, and cheek have been the common head and neck areas affected by epidermoid cysts [6, 7, 8, 9]. Posttraumatic epidermoid inclusion cysts are rare and occur mainly in the fingers, palms, and soles [10]. As surgery is traumatic, there have been reports of postsurgical epidermoid cysts involving the head and neck region [4, 8].
We present a rare case of posttraumatic epidermoid inclusion cyst of the facial region following an untreated orbital zygomaticomaxillary complex fracture.
Case History/Examination
2
A 32‐year‐old male patient presented to the Oral and Maxillofacial Surgery Department at Muhimbili University of Health and Allied Sciences (MUHAS) with complaints of swelling around his right eye for the past year. The patient reported that the swelling was slow‐growing, painless, and not associated with any disturbances in vision or breathing. He noted that the swellings appeared approximately 1 year after sustaining facial injuries from a motor vehicle accident. However, he did not seek treatment for the facial injuries at the time.
Upon examination, two swellings were observed: A 3 × 2 cm swelling at the lower lateral aspect of the right eye and a 4 × 3 cm swelling lateral to the right nasolabial groove (Figure 1).
Preoperative; two swelling at the orbital‐zygomaticomaxillary area, intact skin.
The swellings were fluctuant, mobile, non‐tender, with normal overlying skin. He had intact visual acuity, and eye movement was normal, with no diplopia. Aspiration was done on the inferior cyst via intraoral route, revealing a cheesy‐white granular aspirate (Figure 2). It was submitted for cytological investigation. A CT scan revealed a cystic lesion extending from the lateral side of the globe through a fracture line at the lateral orbital wall to the temporal fossa. Another 4 × 3 cm cystic lesion was below the inferior orbital rim. A 1 cm bone discontinuity was seen at the lateral orbital wall, signifying a non‐union of an inferiorly displaced zygomaticomaxillary complex fracture. Despite the obvious increase in the right orbital volume, there was not a visual disturbance reported prior to the development of the cyst (Figure 3).
Aspirant via intraoral on the infraorbital cyst, see the cheesy like yellowish secretions.
CT scan views (A–C), coronal, axial, sagittal cuts showing the cysts on the orbit and infraorbital regions. (D) A 3D reconstruction CT showing the non‐union lateral orbital rim fracture, see the increased orbital volume on the right orbit signifying a displaced zygomaticomaxillary fracture.
Differential Diagnosis
3
Dermoid cyst, lipoma, neuroma, neurofibroma, abscess.
Conclusion and Results
4
Surgical excision was planned, the patient was prepared, after obtaining an informed consent after explaining in detail about the surgical procedure and advantages and disadvantages of treatment. An infraorbital incision was used as a surgical access for the orbital cyst and an intraoral vestibular incision for the zygomaticomaxillary cyst. The orbital cyst was found to be firmly adhering to the periosteum at the lateral orbital wall connecting to the zygomatic cyst through the non‐union gap at the lateral orbital rim. The cysts were excised with the involved fibrotic tissues along the non‐union fracture areas (Figure 4). No plates or implants were placed on the lateral orbital wall. Soft tissue repair was done, and the operation ended uneventfully. The specimen was sent for histological evaluation, revealing sections showing a cystic lesion lined by stratified squamous epithelium with a granular layer that did not contain eccrine glands, sebaceous glands, or hair follicles. Keratin flakes were not seen in the lumen since the specimen was submitted open with sections showing a fibrous cyst wall with marked lymphoplasmacytic infiltrates and foreign body type of giant cells that were conclusive of epidermoid inclusion cyst (Figure 5). The patient was followed up, and after 1 year, no ocular or nasal symptoms were reported. There were no signs of recurrence as seen on Figure 6 and on the follow‐up CT scan (Figure 7).
(A, B) Intraoperative; showing the cyst and the fracture area on the lateral orbital rim. (C) The specimen from infraorbital region, excised from the intraoral route, see the fibrotic appearance from the previous FNA procedure.
(A) Sections showing a cystic lesion lined by stratified squamous epithelium with a granular layer. Cyst wall does not contain eccrine glands, sebaceous glands or hair follicles. Keratin flakes are not seen in the lumen since the specimen was submitted open. H&E, ×100 magnification. (B) Sections showing a fibrous cyst wall with marked lymphoplasmacytic infiltrates and foreign body type of giant cells (foreign body reaction due to ruptured cysts), H&E ×400 magnification. These features are consistent with epidermal inclusion cyst.
(A, B) Post operative view a, 7 days post operative b, 1 year post‐operative.
(A, B) 1‐year post‐operative CT scan, coronal and axial views showing no signs of recurrence. (C) CT scan 3D reconstructed view showing the lateral orbital rim defect that was unrepaired.
Discussion
5
Epidermoid cyst from localized trauma in the craniofacial region has been reported in several literature. After trauma, the skin epithelial cells are driven deep into the dermis and other tissues, where they continue to proliferate and form an epidermoid inclusion cyst [2, 6, 11, 12, 13]. They have been reported in lips, oral mucosa, scalp, and palms, which are common areas to be traumatized [8, 10, 11]. Epidermoid cysts grow slowly and, when in the orbital region, can present with restricted eye movement, double vision, proptosis, and decreased visual acuity. Depending on the location, the cyst can grow to a bigger size associated with pain and facial disfigurements [14]. The epidermoid inclusion cyst can mimic other facial swellings like the findings from Choi et al. [7] where the swelling resembled parotid pleomorphic adenoma. Rupture of the cyst releases keratinaceous contents, which may incite an inflammatory foreign body reaction that causes pain and could be mistaken for infection, as reported by Jeyaraj et al. [9] where the chin mass resembled an infection.
In our case the patient had a right zygomaticomaxillary complex fracture with an inferior displacement following a motor traffic accident. The fractures were untreated leading to a non‐union gap at the lateral orbital wall. An epidermoid cyst developed possibly from the trapped epithelial cells around the orbital region from the initial facial trauma. The swellings grew slowly, were painless without causing much of the patient's concerns until they became big enough to cause aesthetic issues.
FNAC has been used for diagnosis although histology is mandatory to differentiate epidermoid cysts from other cysts. Depending on the location, epidermoid cysts should be distinguished from other cysts including dermoid cyst, lipoma, pilar cyst, furuncle, pilonidal cyst, and steatocystoma. In radiological investigation, CT scan allows for the good assessment of both bone involvement and extensions, with MRI bringing an edge when the cysts have cranial extensions [15].
Surgery is the treatment of choice for epidermoid inclusion, with complete excision being mandatory to avoid recurrence [16, 17]. In this case, the two cysts were found to be interconnected along the fractured lateral orbital rim. The cysts could not be removed without rupturing, as they were adhering to the periosteum and entangled with the fibrotic tissues. There have been reports of possible malignant transformation to squamous cell carcinoma from the residual keratin‐producing lining of these cysts [17, 18]. This warrants meticulous, timely complete surgical excision of the cyst and thorough histopathologic analysis.
Even though posttraumatic epidermoid inclusion cysts in the craniofacial region are relatively rare, they should be considered as one of the differential diagnoses for craniofacial cysts. Treatment of facial fractures and better surgical techniques are of paramount importance to prevent these complications. Although 1 year follow‐up revealed no recurrency, longer follow‐up is required to monitor for recurrence and other outcomes as the healed fractured bones were not corrected in this case.
Author Contributions
David Kiwango Deoglas: conceptualization, methodology, writing – original draft, writing – review and editing. Paulo Joseph Laizer: methodology, writing – review and editing. Shaban Daudi Shaban: methodology, supervision, writing – review and editing.
Ethics Statement
This case report was conducted in accordance with the principles of the Declaration of Helsinki. All efforts were made to maintain the patient's privacy and confidentiality.
Consent
Written informed consent was obtained from the patient for publication of this article and accompanying images.
Conflicts of Interest
The authors declare no conflicts of interest.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1M. Dutta , J. Saha , G. Biswas , S. Chattopadhyay , I. Sen , and R. Sinha , “Epidermoid Cysts in Head and Neck: Our Experiences, With Review of Literature,” Indian Journal of Otolaryngology and Head & Neck Surgery 65, no. SUPPL 1 (2013): 14–21.24427609 10.1007/s 12070-011-0363-y PMC 3718960 · doi ↗ · pubmed ↗
- 2C. E. Noffke , “Implantation‐Type Epidermoid Cyst of the Mandible,” Dentomaxillofacial Radiology 28, no. 6 (1999): 383–385.10578196 10.1038/sj/dmfr/4600477 · doi ↗ · pubmed ↗
- 3G. Tchernev , I. Temelkova , I. Yungareva , and U. Wollina , “Multiple Epidermal Cysts of the Scalp: Dermatosurgical Approach With Favourable Outcome!,” Open Access Macedonian Journal of Medical Sciences 7, no. 9 (2019): 1509–1511.31198464 10.3889/oamjms.2019.257PMC 6542396 · doi ↗ · pubmed ↗
- 4S. K. Mandal , A. Mandal , and A. A. Bandyopadhy , “Post Surgical Giant Epidermal Inclusion Cyst of the Lid and Orbit‐ A Rare Case,” Journal of Clinical and Diagnostic Research 9, no. 9 (2015): ND 01.10.7860/JCDR/2015/13858.6573 PMC 460626126500932 · doi ↗ · pubmed ↗
- 5T. O. Acarturk and G. M. Stofman , “Posttraumatic Epidermal Inclusion Cyst of the Deep Infratemporal Fossa,” Annals of Plastic Surgery 46, no. 1 (2001): 68–71, 10.1097/00000637-200101000-00015.11192040 · doi ↗ · pubmed ↗
- 6W. C. Wang , L. M. Lin , Y. H. Shen , Y. J. Lin , and Y. K. Chen , “Concurrent Extravasation Mucocele and Epidermoid Cyst of the Lower Lip: A Case Report,” Kaohsiung Journal of Medical Sciences 21, no. 10 (2005): 475–479.16302452 10.1016/S 1607-551X(09)70154-8PMC 11918009 · doi ↗ · pubmed ↗
- 7H. J. Choi , J. H. Lee , and Y. M. Lee , “Traumatic Epidermoid Inclusion Cyst on Cheek Area,” Journal of Craniofacial Surgery 27, no. 4 (2016): e 343–e 344.27244199 10.1097/SCS.0000000000002509 · doi ↗ · pubmed ↗
- 8N. Swain , A. U. Bhandarwar , S. Patel , J. Pathak , and A. Gandevivala , “Postsurgical Epidermal Inclusion Cyst in the Cheek Region,” Journal of Contemporary Dentistry 7, no. 3 (2017): 178–180.