Clinical Outcome of lateral mass screws for traumatic sub-axial facet dislocation
Sabir Khan Khattak, Sajid Hussain, Latif Khan, Ibtisam Haider, Amer Aziz

TL;DR
This study examines the effectiveness of lateral mass screws in treating cervical spine dislocations, showing good functional recovery and spinal stability.
Contribution
The study provides clinical evidence on the safety and reliability of lateral mass screw fixation for traumatic subaxial facet dislocation.
Findings
Lateral mass screw fixation led to excellent functional recovery in most patients.
Neurological recovery was observed in ASIA C and D patients but not in ASIA A or B patients.
C5-6 was the most common dislocation level among the studied patients.
Abstract
This study aimed to analyze the functional and neurological outcome of patients diagnosed with subaxial cervical spine bilateral facet dislocation managed by standard posterior midline approach and lateral mass screw fixation by Margerl technique We retrospectively evaluated 22 patients with traumatic cervical spine injuries who presented at the Orthopaedics and Spine Centre Ghurki Trust Teaching Hospital, Lahore from March 2020 to October 2023. Patients included in this study who has subaxial cervical spine bilateral facet dislocation managed by standard posterior midline approach and lateral mass screw fixation by Magerl technique. Functional outcomes was assessed by neck disability index and ASIA impairment scale at last follow up. Preoperative and post operative neurological status was evaluated with ASIA impairment scale. All the data were analyzed using SPSS version 23. Total 22…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
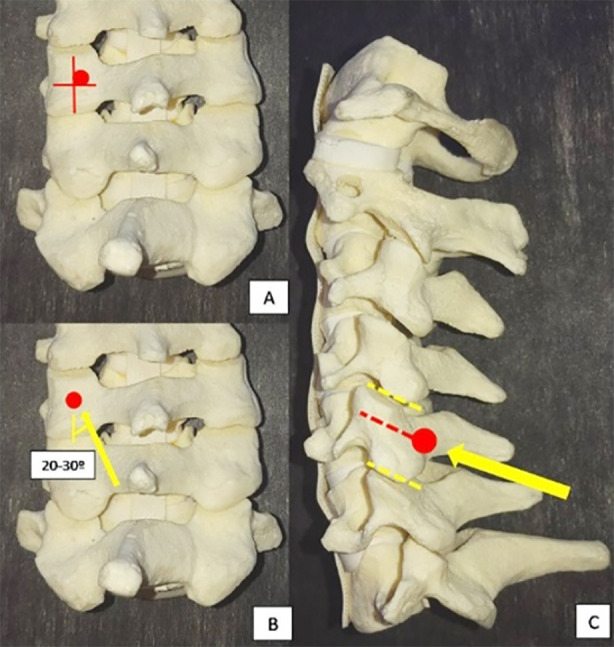 Fig:1
Fig:1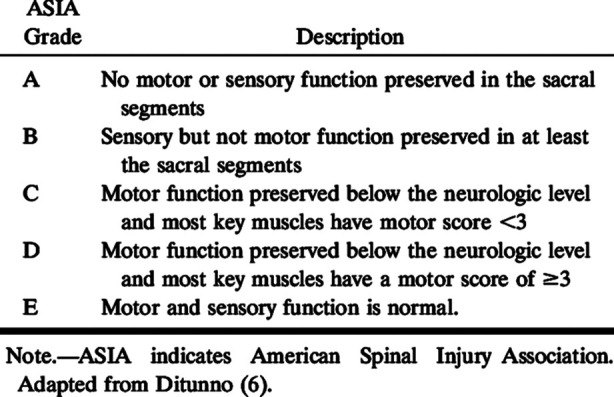 Fig.2
Fig.2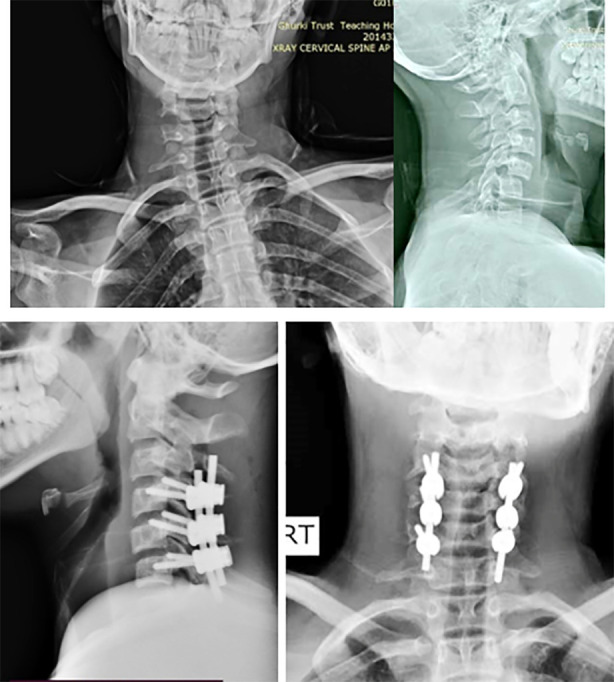 Fig.3
Fig.3| Parameters | n | % |
|---|---|---|
| Total no. of patients | 22 | |
| Age (years) | 39±17.02 (13-70) | |
|
| ||
| Male/Female | 16/6 | |
| Operation Level | ||
| C3-C4 | 5 | |
| C4-C5 | 5 | |
| C5-6 | 12 | |
|
| ||
| Type A | 2 | 9.09 |
| Type B | 1 | 4.55 |
| Type C | 2 | 9.09 |
| Type D | 6 | 27.27 |
| Type E | 11 | 50 |
|
| ||
| Type A | 2 | 9.09 |
| Type B | 1 | 4.55 |
| Type C | - | |
| Type D | - | |
| Type E | 19 | 86.36 |
| Neck Disability Index (NDI) (%) | 21±19.44 | |
| No Disability | 6 | 27.27 |
| Mild Disability | 13 | 59.09 |
| Moderate Disability | 1 | 4.55 |
| Severe Disability | 1 | 4.55 |
| Complete Disability | 1 | 4.55 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsSpinal Fractures and Fixation Techniques · Pelvic and Acetabular Injuries · Spine and Intervertebral Disc Pathology
INTRODUCTION
Traumatic injuries of the subaxial spine account for about 65% of all traumatic cervical spine injuries.1 Among them, facet dislocations and subluxations are the most severe form of injuries resulting in tetraplegia in up to 87% of the cases. Cervical facet dislocations are flexion-distraction injuries that mostly occur due to motor vehicle accidents. In a facet dislocation, the inferior facet of the superior vertebra is forced anteriorly relative to the superior facet of the inferior vertebra, which leads to ‘perched’ or locked facets. Unilateral facet dislocation results in 25% translation of one vertebra over another, while bilateral facet dislocation mostly results in 50% translation.2 Associated fractures include rare vertebral body fractures and relatively common posterior element injuries.
Bilateral facet dislocations are highly unstable injuries with associated neurological deficits and significant soft tissue injury. Urgent reduction, stabilization and decompression are needed for improved clinical outcomes.3 Closed reduction can be performed by applying Gardner-Well tongs. Initially, 2.5 to 5kg traction weight followed by 2-5kg for each level above dislocation, with incremental weights assessment of neurological status and screening with X-ray for reduction is mandatory, once closed reduction is achieved definitive surgical fixation can be done by either anterior cervical discectomy and fusion (ACDF) or posterior lateral mass screws (LMS) or anterior and posterior 360° fusion.4 Anterior cervical decompression and fusion are indicated in cases where a retropulsed disc compromises the canal, it allows restoration of cervical lordosis and reduces tension on the posterior ligamentous complex. Posterior cervical reduction and fusion have the advantage of direct visualisation and reduction of fracture/dislocation, decompression and a biomechanically stronger fixation. Despite advances in surgical techniques and methods of fixation, the optimal surgical approach remains controversial.4-8
Our part of the world which is underdeveloped and populous has a high incidence of cervical spine injuries mostly because of motor vehicle accidents. There are a few specialised centres where cervical spine trauma is being managed, so the local literature about this topic is scarce. We studied functional outcomes of bilateral cervical facet dislocation managed by standard posterior midline approach and lateral mass screws with mergels technique. We hope that our contribution will add further information to the already existing pool of knowledge and help in the advancement of surgical techniques and fixation methods in cervical spinal trauma.
METHODS
This retrospective study was conducted at Orthopaedics and Spine Centre Ghurki Trust Teaching Hospital, Lahore between March 2020 and October 2023. Total 22 patients with traumatic cervical spine injuries confirmed on xray, CT scan with 3D reconstruction and MRI and fulfilled inclusion criteria were included in the study. Consecutive sampling technique was used and the sample size was based on available cases rather than a formal power calculation.
Ethical approval:
The study was approved by the hospital ethical committee (Ref. No .2024/04/R-20, dated April 1, 2024).
Inclusion & Exclusion Criteria:
The study’s patients had bilateral facet dislocations of the subaxial cervical spine, which were treated using the usual posterior midline technique with Magerl technique for lateral mass screw fixation. The age of the participants may vary from 13 to 70 years. Patients with bilateral facet dislocation with intact facets and fit for surgery of either age with no prolapsed anterior disc were included. While patients with fracture of cervical facets or pervious neck surgery, infection or tumor and not fit for surgery were excluded.
Posterior approach with Magerl technique for lateral mass screw fixation:
Standard posterior midline incision was given, after dissection lateral mass was exposed then centre of lateral mass was identified, entry point was made at slightly medial and cranial to the mid point with the screw parallel to the adjacent facet and 20-30 degree of lateral angulation.9
Rehabilitation:
The aim of rehabilitation is early recovery and out of bed mobilization, we started early out of bed mobilization and in bed physio to those with prior neurology loose. A cervical collar was adsvised to patients for six weeks to prevent uncontrolled neck movements.
Followup time:
Six months followup after surgery was done. At the final follow-up, the neck disability index (NDI)10 and American Spinal Injury Association (ASIA) Impairment Scale11 was used to measure functional results. A ten-item questionnaire called the NDI is used to gauge a patient’s level of disability brought on by neck pain. Every item was given a score between 0 and 5, and the total percentage score was determined. No disability is represented by a score of 0-8%, mild disability by 10-28%, moderate disability by 30-48%, severe disability by 50-68%, and complete disability by greater than 68%. The ASIA Score was used to assess neurological state both before and after surgery.
Magerl technique of LMS fixation.9
Statistical Analysis:
Data was analyzed using SPSS 23. Categorical variables, such as gender, level of injury, ASIA score pre-operatively and post-operatively were expressed in frequency and percentage, whereas continuous or quantitative variables such as patient’s age was expressed in mean±SD with range. Chi square test was applied and P-value of ≤0.05 was taken as significant.
RESULTS
Out of the total 22 patients, 72.72% were male and 27.27% were female.The average age was 39^ί^17.02 years (13–70 years). In terms of dislocation level, the most prevalent level was C5-6, which affected 12 patients, followed by C3-4 and C4-5, each of which affected five patients. Pre-operatively, neurological assessments based on the ASIA score indicated that 11 patients (50%) were classified as Grade-E, six patients (27.27%) as Grade-D, two patients (9.09%) as Grade C, one patient (4.55%) as Grade-B, and two patients (9.09%) as Grade-A. Post-operatively, 19 patients (86.36%) demonstrated intact neurological function and were classified as Grade-E, reflecting significant improvement or conservation of neurological status. However, two patients (9.09%) remained at Grade-A, exhibiting complete neurological deficits, while one patient (4.55%) was classified as Grade-B, showing partial neurological impairment. Notably, the number of patients with intact neurological function (Grade-E) improved from 11 to 19 after surgical intervention, indicating neurological improvement in seven patients.
The Neck Disability Index (NDI) was used to evaluate functional outcomes, with a mean score of 21 ± 19.44%. Among the participants, six patients (27.27%) reported no disability, 13 patients (59.09%) experienced mild disability, and one patient each (4.55%) reported moderate, severe, and complete disability. These findings indicate that most patients achieved favorable functional recovery post-operatively, with the majority experiencing either no or mild disability.
ASIA impairment scale.
DISCUSSION
Numerous methods and procedures can be used to conduct posterior cervical fusion on patients.12,13 The LMS method is frequently used for simple screw insertion to reduce the chance of vertebral artery perforation.14 Our findings demonstrate that lateral mass screw fixation by Magerl technique is a reliable and effective approach for managing traumatic subaxial cervical spine bilateral facet dislocation. The mean Neck Disability Index (NDI) of 21±19.44 indicated mild disability in most patients. Neurological outcomes based on ASIA scores revealed that 86.36% of patients maintained intact neurological function postoperatively which improved from 50%, suggesting favorable clinical and functional recovery. The most commonly affected level was C5-6 (54.5%). These results underline the safety and efficacy of the procedure in stabilizing cervical spine injuries and improving functional outcomes. Jiang et al.1 performed a study to measure the short-term clinical outcome for Subaxial Cervical Facet Dislocations patients The results show that 52 patients with subaxial cervical facet dislocation, comprising 15 women and 37 men, were recruited in this study, either with or without neurological disability. The average age was 44.7± 29.0 (31 to 72 years old). The average pre-op NDI was 56±25 while postoperatively it improved to 19±12 after 12 weeks. Another study by Sellin et al.4 found that the C6-7 level accounted for the majority of injuries (37.5%, n=3). With at least three months of follow-up, the mean NDI score was 5.3 (n=6, range, 1–12; standard deviation, 4.5), which is which indicates mild impairment.
Preoperative and post operative radiology of patient with LMS fixation.
The results of this investigation confirm that LMS treatments help produce positive clinical outcomes. The patients’ functional impairment and capacity to perform everyday activities have significantly improved, as evidenced by the decline in NDI scores. Further demonstrating the reliability and stability of LMS in cervical spine procedures is the high rate of successful screw insertion and solid fusion rates. Kim et al.15 performed the study and the findings reveals that in the preoperative and late postoperative follow-up evaluations, there were statistically significant improvements in the mean Neck Disability Index (NDI) scores.
In our study, preoperatively 50% of the patients had intact neurology (ASIA E), followed by
ASIA D which made up of the 27.27% patients, ASIA C 9.09%, ASIA B patients (4.55%), ASIA A 9.09% illustrating the severity of the neurological dysfunction. Postoperatively no neurological recovery was observed in ASIA A or ASIA B patients, while all ASIA C and D patients showed complete recovery.These results indicate that after reduction and LMS fixation with posterior decompression, patients showed improvement in neurology. Rehman L et al16 conduted a study in which LMS fixation was done for facet dislocation after which there is improvement in neurology in 58% patients assessed by Frankles grade.
In our study, Fusion was accomplished in each case. No patient had the onset or worsening of a neurological impairment following surgery. Except in two cases where screws were partially pulled out, there was no evidence of implant failure at the final follow-up. Though LMS is considered safest method of screw placement in cervical spine but it has complication like lateral mass fracture, redo surgery and surgical site infection which is more common than the cervical pedicle screw placement.17
Limitations:
This study has some limitations like retrospective study methodology, limited sample size, single centre and brief follow-up time. Future multicenter studies with larger sample sizes, longer follow-ups, and comparative analyses would help validate and expand upon our findings.
CONCLUSION
Lateral mass screws are a safe and dependable method of cervical fixation that, following a satisfactory reduction, not only stabilizes the cervical spine but also promotes a patient’s great functional recovery in terms of NDI and Neurology.
Authors’ Contribution:
AA, SKK: Study design, questionnaire design, data interpretation, and provided feedback through critical manuscript review. SH, IB: Study concept, study design, literature search, data collection, analysis, and interpretation. LK: Contributed to the literature search and manuscript writing. All authors have read the final version and are responsible and accountable for the accuracy and integrity of the work.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Jiang X Yao Y Yu M Cao Y Yang H Surgical treatment for subaxial cervical facet dislocations with incomplete or without neurological deficit:a prospective study of 52 cases Medical science monitor:Int Med J Exp Clin Res 201723732740 doi:10.12659/MSM.90296110.12659/MSM.902961 PMC 531473528182597 · doi ↗ · pubmed ↗
- 2Dhillon CS Jakkan MS Dwivedi R Medagam NR Jindal P Ega S Outcomes of unstable subaxial cervical spine fractures managed by posteroanterior stabilization and fusion Asian Spine J 2018123416422 doi:10.4184/asj.2018.12.3.4162987976710.4184/asj.2018.12.3.416PMC 6002174 · doi ↗ · pubmed ↗
- 3Kojima K Ishikawa M Endo T Muto J Fukui Y Asamoto S Lateral mass intra-pedicular screw fixation for subaxial cervical spines-An alternative surgical technique J Craniovertebral Junction Spine 2021122165169 doi:10.4103/jcvjs.JCVJS_17_2110.4103/jcvjs.JCVJS_17_21PMC 821424234194163 · doi ↗ · pubmed ↗
- 4Sellin JN Shaikh K Ryan SL Brayton A Fulkerson DH Jea A Clinical outcomes of the surgical treatment of isolated unilateral facet fractures, subluxations, and dislocations in the pediatric cervical spine:report of eight cases and review of the literature Child's Nervous Syst 20143012331242 doi:10.1007/s 00381-014-2395-610.1007/s 00381-014-2395-624615370 · doi ↗ · pubmed ↗
- 5Del Curto D Tamaoki MJ Martins DE Puertas EB Belloti JC Surgical approaches for cervical spine facet dislocations in adults Cochrane Database Syst Rev 2014201410 CD 008129 doi:10.1002/14651858.CD 008129.pub 22535469610.1002/14651858.CD 008129.pub 2PMC 6464931 · doi ↗ · pubmed ↗
- 6Nassr A Lee JY Dvorak MF Harrop JS Dailey AT Shaffrey CI Variations in surgical treatment of cervical facet dislocations Spine 2008337 E 188193 doi:10.1590/0004-282X 201600781837938710.1097/BRS.0b 013e 3181696118 · doi ↗ · pubmed ↗
- 7Wiseman DB Bellabarba C Mirza SK Chapman J Anterior versus posterior surgical treatment for traumatic cervical spine dislocation Curr Opin Orthop 2003143174181 doi:10.1097/00001433-200306000-00009
- 8Moawad AM El-Sawy MM Subaxial cervical spine ligamentous instability anterior versus posterior fixation:prospective nonrandomized study Egyptian J Neurol Psychiatry Neurosurg 202258117 doi:10.1186/s 41983-022-00547-w