Development and validation of a Nomogram for the prediction of patients with sepsis-induced multiple organ dysfunction syndrome
Jinling Ji, Qiong Wang, Kai Wang, Ting Shi, Chang Li

TL;DR
This study creates a prediction model to help doctors assess the risk of multiple organ failure in sepsis patients.
Contribution
A novel nomogram is developed and validated for predicting sepsis-induced multiple organ dysfunction syndrome.
Findings
The model identified seven key variables for predicting SI-MODS.
The model showed strong performance with an area under the curve of 0.903.
The nomogram provides a net benefit for clinical decision-making across a wide threshold probability range.
Abstract
To develop and validate a model capable of predicting the risk of Sepsis-induced multiple organ dysfunction syndrome (SI-MODS) in hospitalized sepsis patients. A retrospective cohort study was performed to analyze the clinical data of 415 patients admitted to Department of Medical Laboratory, The Affiliated Huai’an No.1 People’s Hospital of Nanjing between January 2019 and January 2022. The least absolute shrinkage and selection operator (LASSO) regression analysis was employed to pinpoint potential variables. A nomogram was developed through multivariate logistic regression. For internal validation, the bootstrapping method was utilized. The nomogram’s performance was assessed through calibration, discrimination, and clinical utility analyses. Among the 415 patients, SI-MODS was identified in 46 individuals (11.1%). This model identified seven key variables. The model’s internal…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
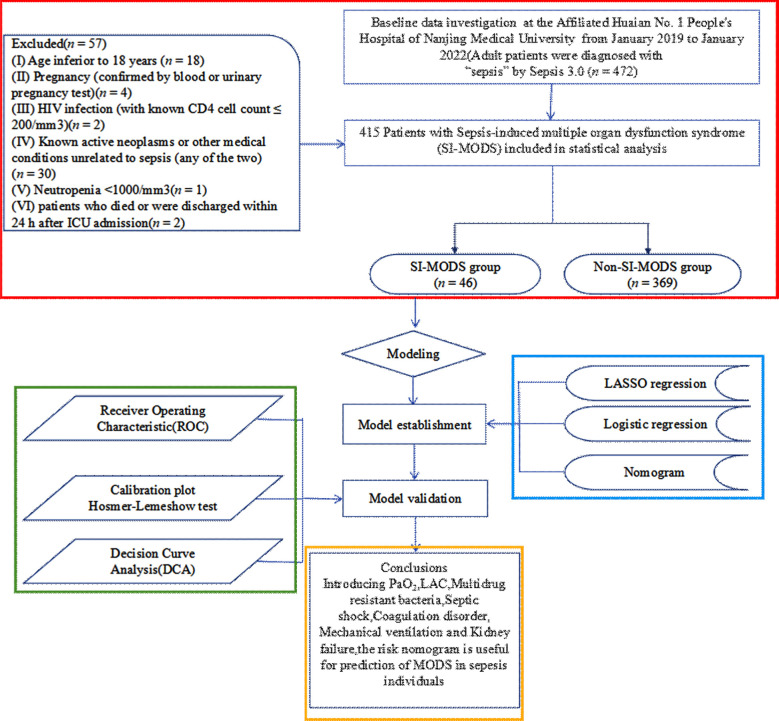 Fig.1
Fig.1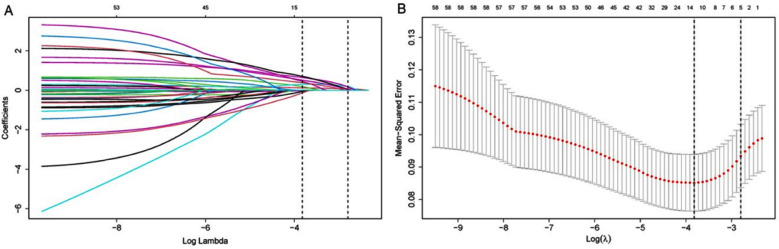 Fig.2
Fig.2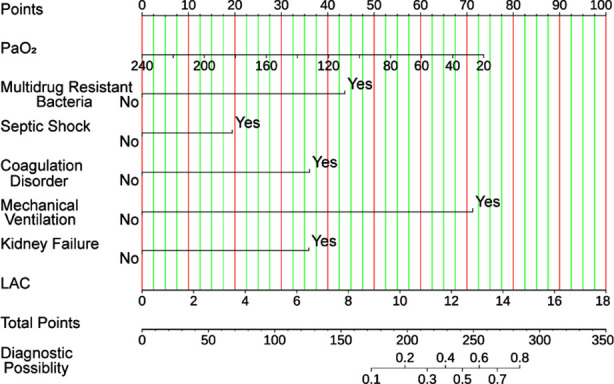 Fig.3
Fig.3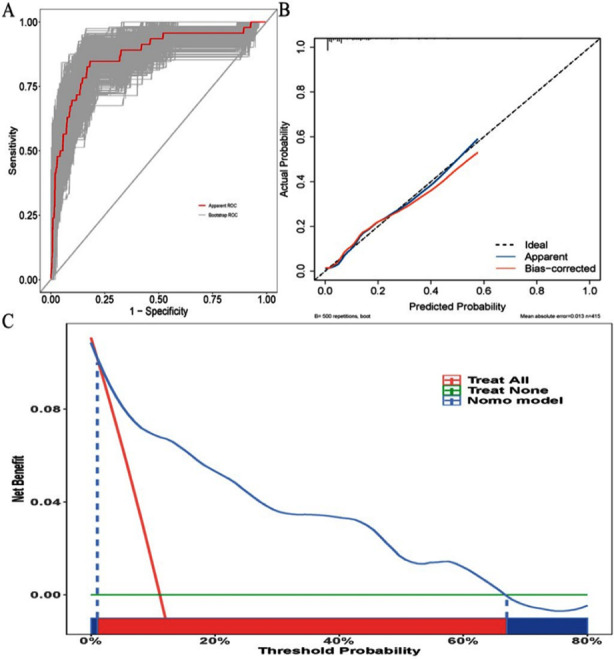 Fig.4
Fig.4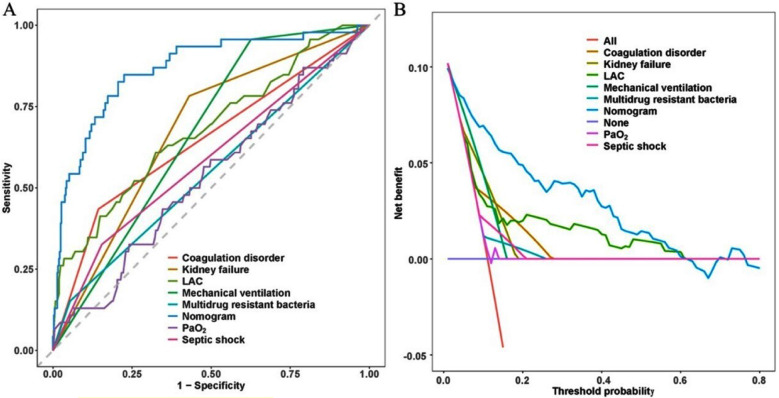 Supplementary Fig.1
Supplementary Fig.1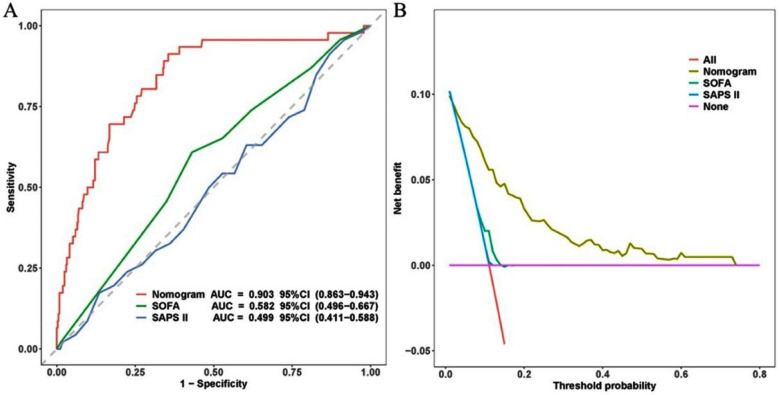 Supplementary Fig.2
Supplementary Fig.2| Organ system | 0 | 1 | 2 | 3 | 4 |
|---|---|---|---|---|---|
| Respiratory (PaO2/FIO2) | >300 | 226~300 | 151~225 | 76~150 | ≤75 |
| Renal (serum creatinine) | ≤100 | 101~200 | 201~350 | 351~500 | >500 |
| Hepatic (serum bilirubin) | ≤20 | 20~61 | 61~120 | 121~240 | >240 |
| Cardiovascular (PAR) | ≤10.0 | 10.1~15.0 | 15.1~20.0 | 20.1~30.0 | >30 |
| Hematologic (platelet count) | >120 | 81~120 | 51~80 | 21~50 | ≥20 |
| Neurologic (Glasgow Coma Score) | 15 | 13~14 | 10~12 | 7~9 | ≤6 |
| Variables | All patients (n = 415) | Non-SI-MODS patients (n = 369) | SI-MODS patients (n = 46) | Fisher/χ2 | p-Value |
|---|---|---|---|---|---|
|
| |||||
| Gender, | 0.705 | 0.401 | |||
| Female | 179 (43) | 156 (42) | 23 (50) | ||
| Male | 236 (57) | 213 (58) | 23 (50) | ||
| Age, | 1.406 | 0.236 | |||
| <60 years | 118 (28) | 101 (27) | 17 (37) | ||
| ≥60 years | 297 (72) | 268 (73) | 29 (63) | ||
|
| |||||
| PT, (s) | 15.6 (13.65, 17.7) | 15.5 (13.6, 17.6) | 16.05 (13.85, 23.13) | 7160.5 | 0.084 |
| INR | 1.27 (1.12, 1.49) | 1.27 (1.12, 1.48) | 1.38 (1.16, 2.2) | 6804 | 0.028 |
| APTT, (s) | 37.9 (31, 47.15) | 38 (31.2, 47) | 37.55 (30.15, 47.47) | 8457.5 | 0.970 |
| TT, (s) | 16.9 (15.8, 18.6) | 16.9 (15.8, 18.5) | 17.7 (15.88, 20.27) | 7359 | 0.142 |
| FIB, (g/L) | 4.34 (2.97, 5.91) | 4.5 (3.19, 6.07) | 3.5 (2.17, 4.58) | 10962.5 | 0.001 |
| D-dimer, (ug/ml) | 4.42 (2.3, 7.94) | 4.42 (2.25, 7.81) | 4.44 (2.4, 11.76) | 7926 | 0.465 |
| PH, | 7.42 (7.34, 7.47) | 7.42 (7.35, 7.47) | 7.41 (7.31, 7.46) | 9686.5 | 0.118 |
| PaCO2, (mmHg) | 34.5 (29.55, 39.1) | 34.5 (30, 39.1) | 33.4 (28.05, 39.6) | 8953.5 | 0.544 |
| PaO2, (mmHg) | 83.4 (64.25, 109) | 85.5 (65.2, 109) | 77.85 (63.37, 103.22) | 9087 | 0.434 |
| BE, (mmol/L) | -3 (-7.45, 1.8) | -3 (-6.6, 2.2) | -2.95 (-12.08, 0.5) | 9597.5 | 0.148 |
| HCO3, (mmol/L) | 21.2 (16.9, 24.95) | 21.2 (16.9, 25.6) | 21.2 (18.05, 24.15) | 8820.5 | 0.664 |
| SO2, (%) | 96.3 (92.85, 98.4) | 96.3 (92.9, 98.3) | 96.3 (92.8, 98.9) | 8331 | 0.839 |
| LAC, (mmol/L) | 2.5 (1.6, 4.4) | 2.4 (1.5, 4.3) | 4.35 (2.3, 12.05) | 5441.5 | < 0.001 |
| WBC, (K/uL) | 10.57 (6.21, 17.12) | 10.73 (6.37, 17.16) | 9.36 (4.74, 14.31) | 9662.5 | 0.126 |
| Neutrophil, (K/uL) | 9.29 (4.67, 15.34) | 9.65 (4.8, 15.66) | 7.57 (3.52, 13.05) | 9829 | 0.08 |
| Lymphocyte, (K/uL) | 0.77 (0.46, 1.19) | 0.77 (0.45, 1.15) | 1 (0.55, 1.39) | 7474 | 0.187 |
| Platelet level, (K/uL) | 141 (79.5, 214.5) | 143 (84, 217) | 121.5 (49.75, 193.25) | 9955 | 0.056 |
| Totalbilirubin, (µmol/L) | 16.1 (9.9, 29.7) | 15.5 (9.5, 28.5) | 22.45 (12.75, 53.45) | 6336.5 | 0.005 |
| NT-proBNP, (pg/ml) | 3063 (1106.5, 10683.5) | 2979 (1040, 10113) | 6119 (1854.75, 20460) | 6815 | 0.029 |
| Albumin, (g/L) | 29.8 (25.85, 33.95) | 29.8 (25.8, 34) | 29.4 (26.22, 32.27) | 8847 | 0.639 |
| Creatinine, (µmol/L) | 98 (66, 170.75) | 98 (66, 170) | 100.5 (66.85, 175.65) | 8389.5 | 0.899 |
| BUN, (µmol/L) | 10.59 (6.85, 15.63) | 10.25 (6.68, 15.32) | 12.93 (7.89, 16.02) | 7691 | 0.300 |
| ALT, (IU/L) | Fisher | < 0.001 | |||
| ≤400 | 384 (93) | 349 (95) | 35 (76) | ||
| > 400 | 31(7) | 20 (5) | 11 (24) | ||
| AST, (IU/L) | 43 (25, 105.05) | 40 (23.2, 87) | 107.65 (49.2, 424) | 4611.5 | < 0.001 |
| GGT, (IU/L) | 39 (18, 79) | 38 (18, 78) | 40 (19.25, 97) | 8249 | 0.757 |
| LDH, (IU/L) | 290 (217, 449.5) | 285 (212, 418) | 464.5 (292.5, 1602.5) | 5168.5 | < 0.001 |
| PCT, (ng/ml) | 11.56 (1.58, 52.57) | 11.18 (1.59, 55.42) | 14.86 (1.2, 32.54) | 8853 | 0.634 |
| Variables | All patients (n = 415) | Non-SI-MODS patients (n = 369) | SI-MODS patients (n = 46) | Fisher/χ2 | p-Value |
|---|---|---|---|---|---|
| Treatment | |||||
| Vasoactive drugs, | 1.545 | 0.214 | |||
| No | 323 (78) | 291 (79) | 32 (70) | ||
| Yes | 92 (22) | 78 (21) | 14 (30) | ||
| Cardiovascular drugs, | 1.045 | 0.307 | |||
| No | 308(74) | 271 (73) | 37 (80) | ||
| Yes | 107 (26) | 98 (27) | 9 (20) | ||
| Anticoagulants, | 53.138 | < 0.001 | |||
| No | 326 (79) | 309 (84) | 17 (37) | ||
| Yes | 89 (21) | 60 (16) | 29 (63) | ||
| Tracheotomy, | Fisher | 0.256 | |||
| No | 380 (92) | 340 (92) | 40 (87) | ||
| Yes | 35 (8) | 29 (8) | 6 (13) | ||
| Mechanical ventilation, | 18.535 | < 0.001 | |||
| No | 140 (34) | 138 (37) | 2 (4) | ||
| Yes | 275 (66) | 231 (63) | 44 (96) | ||
| Tracheal intubation, | 1.526 | 0.217 | |||
| No | 247 (60) | 224 (61) | 23 (50) | ||
| Yes | 168 (40) | 145 (39) | 23 (50) | ||
| Unable to wean off the ventilator, | 2.758 | 0.097 | |||
| No | 316 (76) | 286 (78) | 30 (65) | ||
| Yes | 99 (24) | 83 (22) | 16 (35) | ||
| Comorbidity | |||||
| Prior myocardial infarction | 8.975 | 0.003 | |||
| No | 317 (76) | 290 (79) | 27 (59) | ||
| Yes | 98 (24) | 79 (21) | 19 (41) | ||
| Hypertension, | 0.449 | 0.503 | |||
| No | 238 (57) | 209 (57) | 29 (63) | ||
| Yes | 177 (43) | 160 (43) | 17 (37) | ||
| Diabetes with complication, | Fisher | 1.000 | |||
| No | 400 (96) | 355 (96) | 45 (98) | ||
| Yes | 15 (4) | 14 (4) | 1 (2) | ||
| Diabetes, | 1.628 | 0.202 | |||
| No | 296 (71) | 259 (70) | 37 (80) | ||
| Yes | 119 (29) | 110 (30) | 9 (20) | ||
| Hyperlipidemia, | 3.713 | 0.054 | |||
| No | 313 (75) | 273 (74) | 40 (87) | ||
| Yes | 102 (25) | 96(26) | 6 (13) | ||
| Cerebrovascular disease, | 0.121 | 0.728 | |||
| No | 363 (87) | 324 (88) | 39 (85) | ||
| Yes | 52 (13) | 45 (12) | 7 (15) | ||
| Atrial fibrillation, | 0.676 | 0.411 | |||
| No | 355 (86) | 318 (86) | 37 (80) | ||
| Yes | 60 (14) | 51 (14) | 9 (20) | ||
| COPD, | Fisher | 0.606 | |||
| No | 407 (98) | 361 (98) | 46 (100) | ||
| Yes | 8 (2) | 8 (2) | 0 (0) | ||
| Organ or systemic injury | |||||
| Acute respiratory failure, | 12.563 | < 0.001 | |||
| No | 206 (50) | 195 (53) | 11 (24) | ||
| Yes | 209 (50) | 174 (47) | 35 (76) | ||
| Kidney failure, | 18.925 | < 0.001 | |||
| No | 220 (53) | 210 (57) | 10 (22) | ||
| Yes | 195 (47) | 159 (43) | 36 (78) | ||
| Acute liver injury, | 25.802 | < 0.001 | |||
| No | 318 (77) | 297 (80) | 21 (46) | ||
| Yes | 97 (23) | 72 (20) | 25 (54) | ||
| Coagulation disorder, | 21.951 | < 0.001 | |||
| No | 342 (82) | 316 (86) | 26 (57) | ||
| Yes | 73 (18) | 53 (14) | 20 (43) | ||
| Cardiac insufficiency, | 6.127 | 0.013 | |||
| No | 325 (78) | 296 (80) | 29 (63) | ||
| Yes | 90 (22) | 73 (20) | 17 (37) | ||
| Neurological injury, n (%) | Fisher | 0.126 | |||
| No | 385 (93) | 345 (94) | 40 (87) | ||
| Yes | 30 (7) | 24 (6) | 6 (13) | ||
| Infection site | |||||
| Urinary tract, | 4.822 | 0.028 | |||
| No | 345 (83) | 301 (82) | 44 (96) | ||
| Yes | 70 (17) | 68 (18) | 2 (4) | ||
| Lung, | 2.445 | 0.118 | |||
| No | 212 (51) | 194 (53) | 18 (39) | ||
| Yes | 203 (49) | 175 (47) | 28 (61) | ||
| Abdominal cavity, | 0.512 | 0.474 | |||
| No | 283 (68) | 249 (67) | 34 (74) | ||
| Yes | 132 (32) | 120 (33) | 12 (26) | ||
| Blood culture results | |||||
| Klebsiella pneumoniae, | Fisher | 0.757 | |||
| No | 386 (93) | 342 (93) | 44 (96) | ||
| Yes | 29 (7) | 27 (7) | 2 (4) | ||
| Pseudomonas aeruginosa, | Fisher | 0.446 | |||
| No | 410 (99) | 365 (99) | 45 (98) | ||
| Yes | 5 (1) | 4 (1) | 1 (2) | ||
| Escherichia coli, | Fisher | 0.106 | |||
| No | 375 (90) | 330 (89) | 45 (98) | ||
| Yes | 40 (10) | 39 (11) | 1 (2) | ||
| Staphylococcus, | Fisher | 1.000 | |||
| No | 380 (92) | 338 (92) | 42 (91) | ||
| Yes | 35 (8) | 31 (8) | 4 (9) | ||
| Enterococcus, | Fisher | 0.219 | |||
| No | 407 (98) | 363 (98) | 44 (96) | ||
| Yes | 8 (2) | 6 (2) | 2 (4) | ||
| Bowman acinetobacter, | Fisher | 0.137 | |||
| No | 403 (97) | 360 (98) | 43 (93) | ||
| Yes | 12 (3) | 9 (2) | 3 (7) | ||
| Multidrug resistant bacteria | Fisher | 0.021 | |||
| No | 388 (93) | 349 (95) | 39 (85) | ||
| Yes | 27 (7) | 20 (5) | 7 (15) | ||
| Severity score | |||||
| SOFA | 9 (6, 12) | 9 (6, 12) | 10 (7.25, 12) | 7102.5 | 0.070 |
| SAPS-II | 45 (39, 51) | 45 (39, 51) | 45.5 (38.25, 50.75) | 8502 | 0.985 |
| Complications | |||||
| Cardiopulmonary arrest, | Fisher | 0.513 | |||
| No | 389 (94) | 347 (94) | 42 (91) | ||
| Yes | 26 (6) | 22 (6) | 4 (9) | ||
| Septic shock, | 7.247 | 0.007 | |||
| No | 343(83) | 312 (85) | 31 (67) | ||
| Yes | 72 (17) | 57 (15) | 15 (33) |
| Independent variables | B | SE | OR | 95% CI | Z | p-Value | |
|---|---|---|---|---|---|---|---|
| Lower | Upper | ||||||
| PaO2 | -0.011 | 0.005 | 0.989 | 0.978 | 0.999 | -1.991 | 0.046 |
| LAC | 0.178 | 0.040 | 1.195 | 1.105 | 1.295 | 4.419 | <0.001 |
| Multidrug resistant bacteria | 1.398 | 0.569 | 4.047 | 1.274 | 12.120 | 2.458 | 0.014 |
| Septic shock | 0.622 | 0.404 | 1.863 | 0.827 | 4.066 | 1.541 | 0.123 |
| Coagulation disorder | 1.156 | 0.394 | 3.177 | 1.458 | 6.883 | 2.936 | 0.003 |
| Mechanical ventilation | 2.280 | 0.784 | 9.780 | 2.643 | 65.760 | 2.908 | 0.004 |
| Kidney failure | 1.150 | 0.413 | 3.158 | 1.446 | 7.413 | 2.784 | 0.005 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsSepsis Diagnosis and Treatment · Nosocomial Infections in ICU · Antibiotic Use and Resistance
INTRODUCTION
Multiple organ dysfunction syndrome (MODS) is characterized as an acute and potentially reversible dysfunction affecting two or more organs, caused by various factors.1 Studies indicate that MODS affects 11-40% of adult patients admitted to intensive care units (ICUs).2,3 MODS is prevalent among critically ill patients and is associated with a high mortality rate of 44-76%, primarily due to lack of effective treatments. Consequently, early detection and intervention in the development of MODS are crucial for improving clinical outcomes.4
MODS is the most severe outcome of sepsis progression and is highly correlated with a worse prognosis.5 Recent efforts have been made in developing prediction models for sepsis-induced multiple organ dysfunction syndrome (SI-MODS). Benscoter et al. introduced a novel risk prediction model that assessed the risk of developing multiple organ dysfunction following pediatric cardiac surgery that required cardiopulmonary bypass (CPB). The optimal model, which includes interleukin-8 (IL-8), chemokine ligand 3 (CCL3), and age as predictor variables, achieved an area under the receiver operating characteristic curve (AUROC) of 0.75 through ten-fold cross-validation.6 It was demonstrated by Atreya et al, the utility of a supervised machine learning approach for identifying 20 genes, achieving AUROC ranging from 0.74 to 0.79 in validation and test sets for predicting persistent MODS across different ages and causes of organ dysfunction7 Given the suboptimal performance and limited interpretability of existing models, and the scarcity of research on predictive models for the early diagnosis of SI-MODS, there is a clear need for a new model.8
This study was designed to develop a nomogram model based on independent risk factors to predict the risk of MODS in sepsis patients.
METHODS
From January 2019 and January 2022, patients diagnosed with sepsis were admitted to the Affiliated Huai’an No.1 People’s Hospital of Nanjing Medical University and subsequently enrolled in this retrospective cohort study using simple random sampling.
Inclusion criteria:
- Diagnosis of sepsis according to the Sepsis 3.0 guidelines.9
- Age 18 years or older.
- A minimum intensive care unit (ICU) stay of 48 hours.
- At least one instance meeting the MODS diagnostic criteria. For patients with multiple ICU admissions during their hospital stay, only data from the initial admission were considered.
Exclusion criteria:
- Patients younger than 18 years.
- Pregnant women, confirmed via blood or urinary pregnancy tests.
- Individuals with HIV infection and a known CD4 cell count of 200/mm^3 or less.
- Patients with active neoplasms or other medical conditions not related to sepsis.
- Neutropenia, defined as having fewer than 1000 neutrophils per cubic millimeter of blood.
- Patients who either died or were discharged within 24 hours after ICU admission.
Ethical Approval:
The hospital’s ethical review board approved the study protocol (approval number: KY-2023-156-01, dated Sept. 6, 2023). Informed consent was waived as the data were anonymized, per ethical board approval. The procedures in this study were performed in accordance with the Helsinki Declaration of 1975.
Data Collection:
We reviewed the clinical data of patients in the Electronic Medical Records Systems (EMRS) and Picture Archiving and Communication Systems (PACS). Data were collected retrospectively, encompassing demographic information, chronic complications, laboratory test, Simplified Acute Physiology Score II (SAPS-II) and Sequential Organ Failure Assessment (SOFA) scores and others.
SI-MODS:
Data from all eligible sepsis patients were analyzed to identify those with MODS, defined according to the scoring system developed by Marshall et al.10 This scoring system incorporates clinical and laboratory variables across six organ systems. A total score is computed, as detailed in Table-I, which assists clinicians in predicting the mortality risk of critically ill patients.
Statistical Analysis:
Continuous variables are summarized using the median and interquartile range and compared employing the Wilcoxon rank-sum test. Categorical variables are presented as numbers and percentages and are compared using either Chi-square tests or Fisher’s exact test. Feature selection is a critical step in constructing models. Predictor selection and model regularization were performed using the Least Absolute Shrinkage and Selection Operator (LASSO) regression analysis. Following this, a multivariate logistic regression analysis was conducted to develop a predictive model that distinguishes between SI-MODS and non-SI-MODS patients.
This model was then used to create a nomogram. The discriminative performance of the model was assessed by calculating the area under the receiver operating characteristic curve (AUC). For internal validation, a bootstrapping analysis with 500 iterations was conducted.11 The Hosmer-Lemeshow test was conducted to assess the calibration of the model. Additionally, Decision Curve Analysis (DCA) was performed to determine the clinical utility of the model.12 Data were statistically analyzed using the R software (v3.6.3). The significance level was established at p <0.05.
RESULTS
A total of 472 patients were diagnosed with sepsis upon admission according to Sepsis 3.0 criteria. Following exclusion criteria application, 57 patients were excluded as shown in Fig.1. Consequently, 415 patients were included in the study, among whom 46 (11.1%) developed SI-MODS after ICU admission. Table-II and III describes the differences in characteristics between the SI-MODS and non-SI-MODS groups.
Flowchart of data extraction and study design.Abbreviations: PaO2: Arterial partial pressure of oxygen; LAC: Lactate. LASSO: Least absolute shrinkage and selection operator.
Patients in the SI-MODS group exhibited a higher incidence of anticoagulant use, mechanical ventilation, previous myocardial infarction, acute respiratory failure, kidney failure, acute liver injury, coagulation disorders, cardiac insufficiency, and urinary tract infections compared to those in the non-SI-MODS group. Initial laboratory values such as international normalized ratio (INR), lactate (LAC), total bilirubin, NT-proBNP, alanine aminotransferase (ALT), aspartate aminotransferase (AST), and lactate dehydrogenase (LDH) were significantly higher in septic patients with SI-MODS than in those without (p<0.05). Conversely, fibrinogen (FIB) levels were lower in the SI-MODS group compared to the non-SI-MODS group (p<0.05).
Predictors entering the model:
LASSO regression analysis was utilized to refine the patient dataset from 62 variables to 14, based on non-zero coefficients (Fig.2A-2B). Using the “Backward: Wald” multiple logistic regression model, seven predictors significantly associated with SI-MODS were identified: partial pressure of oxygen (PaO_2_), LAC, multidrug-resistant bacteria, septic shock, coagulation disorder, mechanical ventilation, and kidney failure (Table-IV).
LASSO regression analysis was performed to select the predictors.
Establishment of the Model and Nomogram:
A predictive model for SI-MODS was developed based on seven crucial predictors, and the coefficients assigned to each predictor in the model were as follows: PaO_2_ (-0.011), LAC (0.178), Multidrug-resistant bacteria (1.398), Septic shock (0.622), Coagulation disorder (1.156), Mechanical ventilation (2.280), and Kidney failure (1.150).
A nomogram was constructed to assess the individual risks of SI-MODS using multivariate logistic regression analysis (Fig.3). The model’s derived formula was: logistic (risk score) = -5.162 -0.011 × PaO_2_ + 0.178 × LAC + 1.398 × Multidrug resistant bacteria + 0.622 × Septic shock + 1.156 × Coagulation disorder + 2.280 × Mechanical ventilation + 1.150 × Kidney failure (Table-III).
The predictive nomogram can evaluate the risk of SI-MODS in patients with sepsis. Abbreviations: PaO2: Arterial partial pressure of oxygen; LAC: Lactate.
To evaluate the accuracy of the nomogram, multiple methodologies were employed. The area under the curve (AUC) of the nomogram was 0.903 (95% CI: 0.863-0.943), as determined through a bootstrap method involving 500 resamples (Fig.4A). The predicted probabilities from the nomogram showed a high concordance with observed clinical outcomes, as depicted in Fig.4B. Additionally, a Hosmer-Lemeshow test yielded a p-Value of 0.290, indicating excellent model fit. In the decision curve analysis (DCA), the nomogram’s risk estimates for SI-MODS demonstrated a significantly greater net benefit compared to both the “screen-none” and “screen-all” strategies, particularly when the threshold probability for SI-MODS ranged from 1% to 66% (Fig.4C).
The nomogram model was verified through the following analyses. (A) The nomogram-related ROC curve was constructed by bootstrap resampling (500 iterations). (B) The predictive accuracy of the nomogram was evaluated using a calibration plot. (C) DCA was performed for the nomogram, and it illustrates the expected net benefit per patient based on the nomogram’s prediction of SI-MODS risk.
Model comparison:
Supplementary Fig.1A presented the results of the receiver operating characteristic (ROC) curve analysis. The AUC values were as follows: 0.903 for the nomogram, and 0.535, 0.679, 0.549, 0.586, 0.646, 0.665, and 0.676 for PaO_2_, LAC, multidrug-resistant bacteria, septic shock, coagulation disorder, mechanical ventilation, and kidney failure, respectively. Notably, the nomogram demonstrated superior discriminatory accuracy in identifying patients at risk of SI-MODS compared to each individual variable within the nomogram (all P < 0.05).
Comparison of models in the entire study cohort.(A) ROC curves of various models. (B) DCA curves of various models. Abbreviations: PaO2: Arterial partial pressure of oxygen; LAC: Lactate.
The clinical utility of the model was assessed using DCA. The results revealed that the nomogram outperformed models that solely incorporated risk factors from within the nomogram itself. This advantage was evident in the overall net benefit across a broad spectrum of threshold probabilities (Supplementary Fig.1B).
The predictive model demonstrated superior performance compared to both the SOFA and SAPS-II in assessing the risk of SI-MODS in sepsis patients, with statistically significant differences (both P < 0.05, Supplementary Fig.2A). The AUC for the predictive model was 0.903 (95% CI: 0.863-0.943), significantly higher than the AUCs for the SOFA score (0.582, 95% CI: 0.496–0.667) and the SAPS-II score (0.499, 95% CI: 0.411–0.588).
Comparison of ROC and DCA curves between the predictive model (nomogram) and the SOFA and SAPS-II scoring methods. (A) ROC curves; (B) DCA curves.Abbreviations: SOFA: Sequential organ failure assessment; SAPS-II: Simplified acute physiology score II; AUC: Area under curve; CI: Confidence interval.
DCA was conducted to evaluate the clinical utility of the predictive model and conventional scoring methods. The analysis demonstrated that for threshold probabilities greater than 1%, interventions based on the nomogram yielded a higher net benefit than those guided by the SOFA and SAPS-II (Supplementary Fig.2B).
DISCUSSION
In the present study, we firstly constructed a nomogram to predict SI-MODS, utilizing seven variables from sepsis patients. These variables included PaO_2_, LAC, multidrug resistant bacteria, septic shock, coagulation disorder, mechanical ventilation, and kidney failure. The nomogram showed good discriminatory ability, calibration, and clinical usefulness, which is considered more effective than univariate analysis for choosing predictors.13,14 Consistently, Luo et al, developed a nomogram based on age, diastolic blood pressure, LAC, PaO_2_, platelet, mechanical ventilation, and found that it could help clinicians reasonably determine the risk of sepsis associated-acute respiratory failure.15 Xu et al, established a nomogram incorporating thirteen clinical features including septic shock, and showed a predictive ability to predict the acute respiratory distress syndrome risk in patients with sepsis.16 In addition, it has been reported that the emergence of multidrug-resistant organisms (MDROs) has intensified the challenges in managing multidrug-resistant sepsis.17 Coagulation disorder is closely associated with SI-MODS, and anticoagulant therapy is considered as an effective treatment for SI-MODS.18 Moreover, kidney failure is one of the most frequent complications underlying sepsis.19
Besides, this predictive model also demonstrated superior performance compared to both the SOFA and SAPS-II in assessing the risk of SI-MODS in sepsis patients. The AUC for the predictive model was 0.903 (95% CI: 0.863-0.943), significantly higher than the AUCs for the SOFA score (0.582, 95% CI: 0.496-0.667) and the SAPS-II score (0.499, 95% CI: 0.411-0.588). DCA analysis further proved the clinical utility of the predictive model, and demonstrated that for threshold probabilities greater than 1%, interventions based on the nomogram yielded a higher net benefit than those guided by the SOFA and SAPS-II. Therefore, the combined model may be a better choice for predicting MODS in sepsis patients, which was in line with previous reports.20,21
Limitations:
This predictive model presents several limitations that warrant attention. Firstly, the nomogram was developed from data collected during a three-year prospective study at the First Affiliated Hospital of Nanjing Medical University in Huai’an. Consequently, further multicenter studies are essential to validate the nomogram’s applicability across different regions or countries. Secondly, the nomogram does not account for the etiology of SI-MODS. This limitation signifies an area of uncertainty that necessitates further research to understand how SI-MODS develops. Thirdly, the analysis excluded certain patient variables, such as treatment regimens and duration, due to their absence in the initial dataset. The inclusion of these variables in future studies could potentially improve the predictive accuracy of the model.
CONCLUSION
Our study firstly develops a nomogram incorporating based on PaO_2_, LAC, multidrug resistant bacteria, septic shock, coagulation disorder, mechanical ventilation, and kidney failure can predict the risk of MODS in sepsis patients, which helps clinicians make risk-based decisions and treatment strategies.
Authors’ Contributions:
JJ and QW: Conceived, designed the study and were involved in writing and revising of the manuscript.
KW, TS and CL: Collected the data and performed the analysis.
All authors have read, approved the final manuscript and are responsible for the integrity of the study.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Qian D Zhou D Liu H Xu D Therapeutic effects of percutaneous coronary intervention on acute myocardial infarction complicated with multiple organ dysfunction syndrome Pak J Med Sci 201935617011706 doi:10.12669/pjms.35.6.11623177751910.12669/pjms.35.6.1162 PMC 6861476 · doi ↗ · pubmed ↗
- 2Bernard GR Vincent J-L Laterre P-F La Rosa SP Dhainaut J-F Lopez-Rodriguez A Efficacy and safety of recombinant human activated protein C for severe sepsis N Engl J Med 200134410699709 doi:10.1056/NEJM 2001030834410011123677310.1056/NEJM 200103083441001 · doi ↗ · pubmed ↗
- 3Guidet B Aegerter P Gauzit R Meshaka P Dreyfuss D Group C-RS Incidence and impact of organ dysfunctions associated with sepsis Chest 20051273942951 doi:10.1378/chest.127.3.9421576478010.1378/chest.127.3.942 · doi ↗ · pubmed ↗
- 4Gourd NM Nikitas N Multiple Organ Dysfunction Syndrome J Intensive Care Med 2020351215641575 doi:10.1177/08850666198714523145513310.1177/0885066619871452 · doi ↗ · pubmed ↗
- 5Silva CMS Wanderley CWS Veras FP Sonego F Nascimento DC Gonçalves AV Gasdermin D inhibition prevents multiple organ dysfunction during sepsis by blocking NET formation Blood 20211382527022713 doi:10.1182/blood.20210115253440754410.1182/blood.2021011525 PMC 8703366 · doi ↗ · pubmed ↗
- 6Benscoter AL Alten JA Atreya MR Cooper DS Byrnes JW Nelson DP Biomarker-based risk model to predict persistent multiple organ dysfunctions after congenital heart surgery:a prospective observational cohort study Crit Care 2023271193 doi:10.1186/s 13054-023-04494-73721054110.1186/s 13054-023-04494-7PMC 10199562 · doi ↗ · pubmed ↗
- 7Atreya MR Banerjee S Lautz AJ Alder MN Varisco BM Wong HR Machine learning-driven identification of the gene-expression signature associated with a persistent multiple organ dysfunction trajectory in critical illness E Bio Medicine 202499104938 doi:10.1016/j.ebiom.2023.1049383814263810.1016/j.ebiom.2023.104938 PMC 10788426 · doi ↗ · pubmed ↗
- 8Chothani S Schäfer S Adami E Viswanathan S Widjaja AA Langley SR Widespread Translational Control of Fibrosis in the Human Heart by RNA-Binding Proteins Circulation 201914011937951 doi:10.1161/circulationaha.119.0395963128472810.1161/CIRCULATIONAHA.119.039596 PMC 6749977 · doi ↗ · pubmed ↗