Spontaneous coronary artery dissection in a male patient with haemophilia A: a case report
Mitsukuni Kimura, Yasuhiro Nakano, Kotaro Abe, Tetsuya Matoba

TL;DR
A 50-year-old man with haemophilia A experienced a rare heart condition called spontaneous coronary artery dissection, which was successfully managed without bleeding complications.
Contribution
This case highlights SCAD in a haemophilia patient and demonstrates the utility of CCTA in monitoring SCAD.
Findings
The patient was diagnosed with SCAD confirmed by intravascular ultrasound and CCTA.
Conservative treatment with medications resolved the haematoma without bleeding complications.
CCTA effectively tracked the resolution of the intramural haematoma over time.
Abstract
Spontaneous coronary artery dissection (SCAD) is characterized by the unexpected formation of an intramural haemorrhage within the wall of an epicardial coronary artery with or without an intimal tear, resulting in an acute coronary syndrome. Haemophilia A and B are inherited X-linked recessive bleeding disorders caused by the absence or dysfunction of clotting factors VIII (FVIII) or IX. A 50-year-old male patient with a history of haemophilia A, type 2 diabetes and smoking presented to our facility with prolonged chest pain. His laboratory results revealed increased myocardial biomarkers and an elevated activated partial thromboplastin time despite the absence of previous bleeding tendencies or coagulation factor replacement therapy. Non-ST-elevation myocardial infarction was suspected, and coronary angiography detected severe stenosis in the left circumflex artery. Intravascular…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
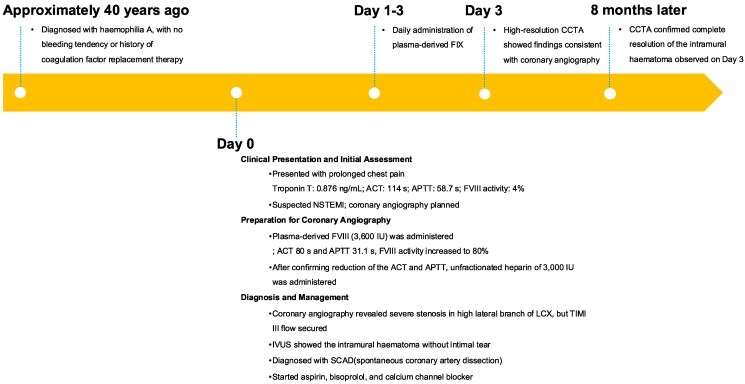 Figure 1
Figure 1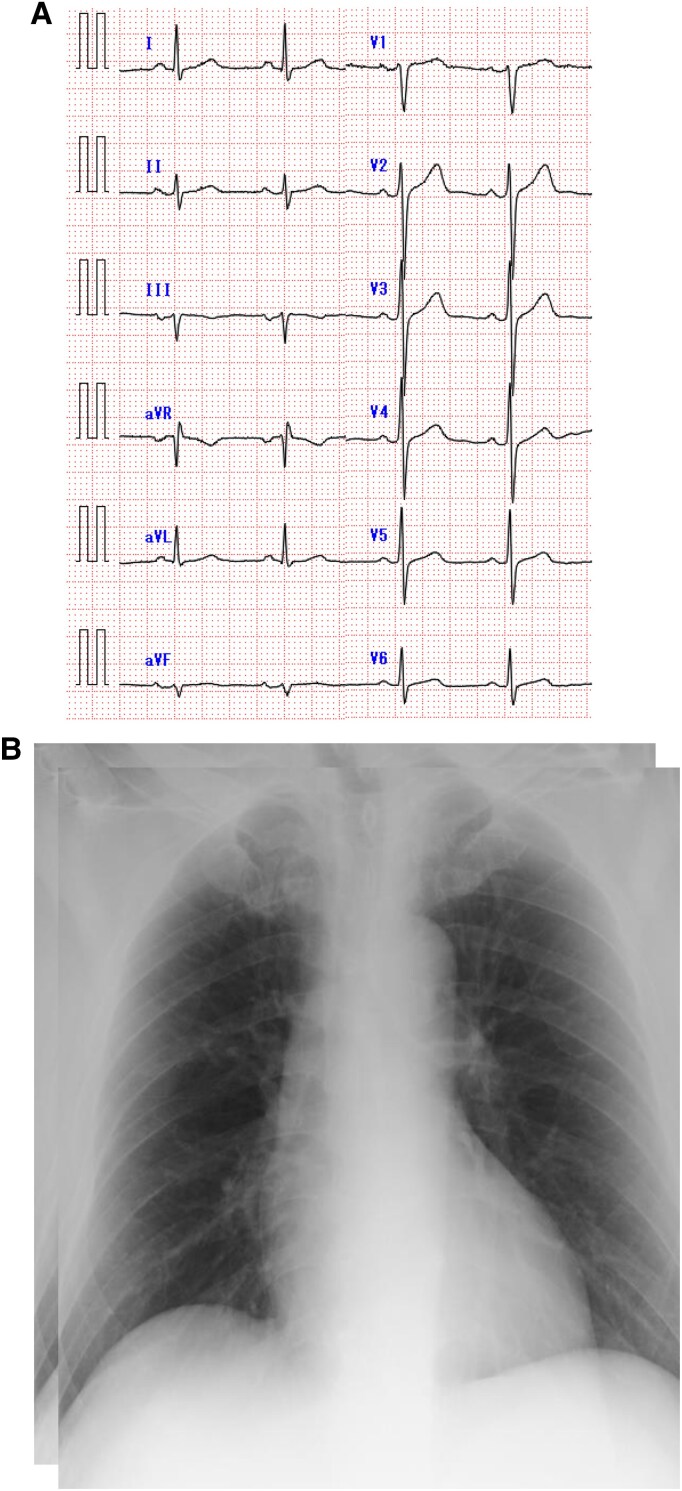 Figure 1
Figure 1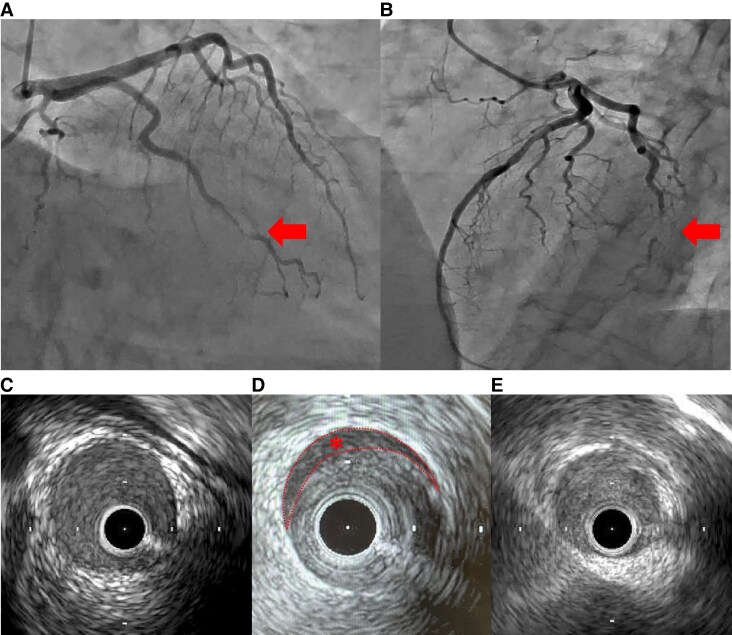 Figure 2
Figure 2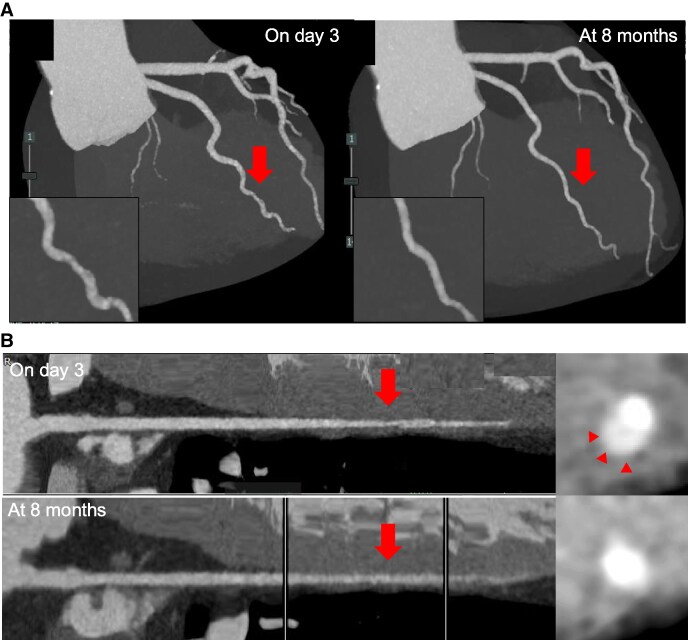 Figure 3
Figure 3| Day 0 | Day 0 | Day 1 | Day 3 | Normal values | |
|---|---|---|---|---|---|
| The arrival at hospital | 15 min after administration of plasma-derived FXIII | ||||
| CK (U/L) | 601 | 508 | 393 | 191 | 59–248 |
| CK-MB (U/L) | 77 | 67 | 49 | 13 | <12 |
| Troponin T (ng/mL) | 0.876 | 0.810 | 0.740 | 0.543 | <0.014 |
| PT-INR | 0.89 | 1.04 | 1.02 | 1.08 | 0.80–1.20 |
| APTT (second) | 58.7 | 31.1 | 34.2 | 39.3 | <35.0 |
| Factor VIII activity (%) | 4 | — | 53 | — | 60–150 |
- —JSPS10.13039/501100000646
- —KAKENHI10.13039/501100001691
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCardiovascular Issues in Pregnancy · Cardiac Structural Anomalies and Repair · Acute Myocardial Infarction Research
Introduction
Spontaneous coronary artery dissection (SCAD) is characterized by the unexpected formation of intramural haemorrhage within the wall of an epicardial coronary artery with or without an intimal tear, resulting in an acute coronary syndrome (ACS).^1^ Approximately 90% of SCAD cases occur in women, and SCAD is a frequent cause of acute myocardial infarction (AMI) in young women.^1^ A recent study hypothesized that the primary mechanism of SCAD is a disruption of the vasa vasorum resulting in the secondary intramural haemorrhage to form a haematoma, which may obstruct the bloodstream.^2^ Haemophilia A and B are inherited X-linked recessive bleeding disorders caused by the absence or dysfunction of clotting factors VIII (FVIII) or IX. Some cohort studies revealed that patients with haemophilia are more likely to develop coronary artery disease, especially AMI, at a younger age despite the presence of bleeding disorders.^3,4^ However, the mechanisms by which patients with haemophilia suffer from the early onset of cardiovascular disease remain unknown.
Here, we report the first case of a patient with haemophilia who suffered AMI due to SCAD. We paid special attention to antithrombotic therapy during catheterisation. Further, we used high-resolution coronary computed tomographic angiography (CCTA) to observe the SCAD lesion during the acute and healing phases, which seemed useful for SCAD lesion observation, especially in cases with a high risk of cardiac catheterisation.
Summary figure
**
Case presentation
A 50-year-old male patient visited our hospital because of sudden prolonged chest pain. He was diagnosed with haemophilia A in childhood, but demonstrated no bleeding tendency and was not treated with coagulation factor replacement therapy. He was a current smoker, reporting a history of type 2 diabetes. His blood pressure was 132/84 mmHg, and his pulse rate was 73 bpm. Electrocardiography demonstrated no significant ST-segment elevation or depression (Figure 1A). Laboratory examination detected increased myocardial biomarkers, including serum troponin T at 0.876 ng/mL (normal < 0.014), creatine kinase at 601 U/L (normal >59 to < 248), and creatine kinase-MB at 77 U/L (normal < 12). The prothrombin time and international normalized ratio were normal. However, the APTT was increased at 58.7 s (normal < 35), and the factor VIII activity was 4% (normal >60 to <150) (Table 1). The chest X-ray revealed no cardiac enlargement or pulmonary congestion (Figure 1B). Echocardiography demonstrated no local asynergy and almost normal left ventricular systolic function with a left ventricular ejection fraction of 60%. Hence, NSTEMI was suspected. The patient had persistent chest symptoms after the arrival at the hospital; thus, we decided to perform coronary angiography using a right radial approach after administering plasma-derived VIII (rurioctocog alfa, Takeda Pharmaceuticals) of 3600 IU (40 IU/kg), resulting in an VIII activity of 80%. The ACT was reduced from 114 to 80 s and APTT was reduced from 58.7 to 31.1 s after 15 min of administration (Table 1). Unfractionated heparin at 3000 IU was administered after local anaesthesia with lidocaine and a 6F introducer sheath insertion. Coronary angiography revealed single-vessel disease with a severe stenosis of the high lateral branch of the left circumflex artery (Figure 2A, B). The stenosis remained unchanged despite the intracoronary administration of nitro-glycerine, and atherosclerosis was mild. Hence, we proceeded with intracoronary imaging using Intravascular ultrasound (IVUS) (AnteOwl, Terumo Corp). This imaging detected the presence of an intramural haematoma and the absence of an intimal tear (Figure 2C, D, E). No evidence indicated plaque rupture or erosion, which could have caused the ACS. Therefore, we diagnosed this patient with NSTEMI related to SCAD. Thrombolysis in myocardial infarction III flow was secured; thus, we adopted a conservative approach. We started aspirin (ASA) and bisoprolol for this patient to treat SCAD as well as a calcium channel antagonist to control blood pressure after coronary angiography. The peak serum creatine kinase level was 601 mg/dL. We administered plasma-derived FXIII daily until post-operative day 3, but FXIII administration was completed without any bleeding complications after ASA administration; thus, we decided not to administer a coagulation factor replacement therapy. An ultra-high-resolution CCTA^5^ was performed on day 3 (Aquilion Precision, Canon, Inc.), and this CCTA revealed similar findings to coronary artery imaging. The patient underwent abdominal echography as part of the screening for extracoronary arthropathies (especially fibromuscular dysplasia), which revealed no abnormal results. He was discharged on day 11. CCTA at the 8-month follow-up detected the disappearance of the intramural haematoma seen on day 3, as well as lesion resolution (Figure 3A, B).
(A) Electrocardiogram upon admission. (B) Chest X-ray upon admission.
Angiography and IVUS of the left coronary artery. (A) and (B) Angiography demonstrating severe stenosis of the high lateral branch of the left circumflex artery. (C) The IVUS image of the proximal segment, (D) the culprit lesion and (E) the distal segment. IVUS image of the culprit lesion exhibited a false lumen ().*
(A) Maximum intensity projection (MIP) image of CCTA. Left: MIP image demonstrating dissection flaps and stenosis on day 3. Right: a healed lesion at 8 months (arrows). (B) Curved planar reformation (CPR) image of the CCTA. Upper panel: CPR image showing intramural haematoma in the culprit lesion on day 3 (arrows). Lower panel: Absence of haematoma at 8 months.
Discussion
We revealed two important clinical issues: (i) SCAD in a male patient with haemophilia and (ii) the usefulness of CCTA to observe SCAD lesions.
First, patients with haemophilia can develop MI due to SCAD. The cause of SCAD frequently includes pre-disposing factors associated with vascular vulnerabilities (e.g. fibromuscular dysplasia, connective tissue disorder or inherited tissue disorder) and precipitating factors such as emotional stress, physical stress (e.g. from an extreme Valsalva manoeuvre, retching, vomiting, coughing or isometric exercise), the use of stimulant medications or illicit drugs and hormonal triggers (e.g. pregnancy).^6^ However, 90% of SCAD cases occur in women; thus, the pre-disposing factors of male SCAD cases remain unclear. The proportion of fibromuscular dysplasia is generally lower and physical exertion may trigger SCAD in male patients.^7^ In this case, IVUS findings revealed an intramural haematoma without an intimal tear despite the absence of obvious pre-disposing or precipitating factors except for hypertension, which is predominantly observed in patients with haemophilia. Further, the lesion was flanked by arteries of normal calibre, resulting in a type 2A SCAD diagnosis.^1^ Considering the hypothesis that the primary mechanism of SCAD is a vasa vasorum disruption resulting in secondary intramural haemorrhage forming a haematoma, in patients with haemophilia, the pre-disposition to bleeding may contribute to the expansion of the haematoma, potentially causing SCAD to develop AMI. Previous cohorts reporting that patients with haemophilia developed MI at a young age did not include coronary imaging data, and these reports were conducted when SCAD was not well recognized. Therefore, young patients with haemophilia who developed MI may include SCAD cases. The present case does not provide a causal association between SCAD and haemophilia, but reports indicated spontaneous dissections in cervical vessels in a patient with haemophilia.^8^ Additional research is required to confirm any potential connection between SCAD and haemophilia, but this report is important to recognize that young patients with haemophilia may be at risk of MI due to SCAD.
Second, CCTA may be a useful means of observing dissection lesions in patients with haemophilia having SCAD. In patients with haemophilia undergoing catheterisation, pre- and post-procedural coagulation factor supplementation is required, and careful attention must be paid to haemorrhagic complications such as haematoma formation at the puncture site. In our case, ultra-high-resolution CCTA confirmed both the flap in the acute phase and its resolution in the chronic phase. Catheterisation is undoubtedly the gold standard for diagnosing SCAD, but CT may be effectively used for follow-up.
Conclusions
We reported the first case of a patient with haemophilia who developed AMI due to SCAD, indicating an interaction in the pathogenesis. A high-resolution CCTA was useful to follow-up on the SCAD lesion.
Supplementary Material
ytaf196_Supplementary_Data
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Kim ESH . Spontaneous coronary-artery dissection. N Engl J Med 2020;383:2358–2370.33296561 10.1056/NEJ Mra 2001524 · doi ↗ · pubmed ↗
- 2Jackson R, Al-Hussaini A, Joseph S, Van Soest G, Wood A, Macaya F. Spontaneous coronary artery dissection: pathophysiological insights from optical coherence tomography. JACC Cardiovasc Imaging 2019;12:2475–2488.30878439 10.1016/j.jcmg.2019.01.015 · doi ↗ · pubmed ↗
- 3Pocoski J, Ma A, Kessler CM, Boklage S, Humphries TJ. Cardiovascular comorbidities are increased in US patients with haemophilia A: a retrospective database analysis. Haemophilia 2014;20:472–478.24286307 10.1111/hae.12339 · doi ↗ · pubmed ↗
- 4Girolami A, Ruzzon E, Fabris F, Varvarikis C, Sartori R, Girolami B. Myocardial infarction and other arterial occlusions in patients with haemophilia A: a cardiological evaluation of all 42 cases reported in the literature. Acta Haematol 2006;116:120–125.16914907 10.1159/000093642 · doi ↗ · pubmed ↗
- 5Oostveen LJ, Boedeker KL, Brink M, Prokop M, de Lange F, Sechopoulos I. Physical evaluation of an ultra-high-resolution CT scanner. Eur Radiol 2020;30:2552–2560.32040726 10.1007/s 00330-019-06635-5PMC 7160079 · doi ↗ · pubmed ↗
- 6Hayes SN, Tweet MS, Adlam D, Kim ESH, Gulati R, Price JE, et al Spontaneous coronary artery dissection: JACC state-of-the-art review. JACC 2020;76:961–984.32819471 10.1016/j.jacc.2020.05.084 · doi ↗ · pubmed ↗
- 7Khalili H, Hanzel GS. Periprocedural bleeding in patients undergoing WATCHMAN device placement. JACC Cardiovasc Interv 2016;9:865–866.27101916 10.1016/j.jcin.2016.02.023 · doi ↗ · pubmed ↗
- 8Iacono S, Baschi R, Di Giorgi L, Gagliardo C, Pezzini A, Monastero R. Internal carotid artery dissection in a patient with haemophilia A: a case report and literature review. Neurol Sci 2023;44:1765–1768.36795298 10.1007/s 10072-023-06671-6 · doi ↗ · pubmed ↗