Hyperthyroidism From Graves Disease Relapsed as Hot Nodule
Suemi Marui, Caroline P F Oliveira, Leandro T Hyppolito, Tomoco Watanabe

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
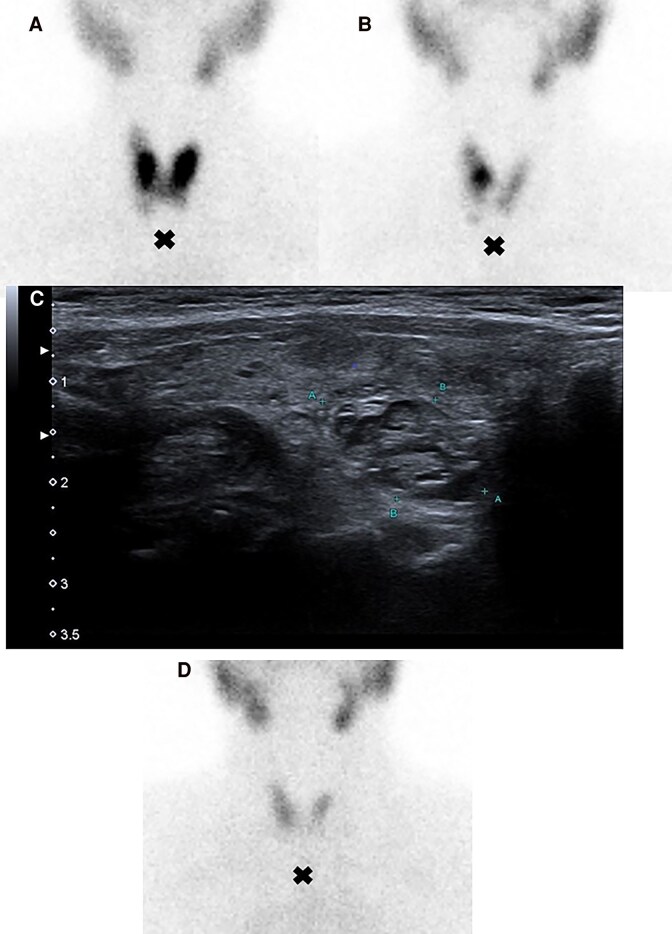 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsThyroid Disorders and Treatments · Thyroid Cancer Diagnosis and Treatment · Neuroendocrine Tumor Research Advances
Image Legend
A 70-year-old female presented with hyperthyroidism from Graves disease (GD) had positive thyrotropin receptor antibodies (TRAb) (3.78 IU/L, normal <0.55 IU/L) and high thyroid radioactive iodine uptake on a 24-hour test with diffuse distribution (Fig. 1A) [1]. Thyroid ultrasound showed a 0.6-cm cystic-solid isoechoic nodule in the right lobe. After 36 months on methimazole, thyroid function normalized with TRAb persistently <0.55 IU/L. Six months after stopping methimazole, the patient relapsed with thyrotropin <0.01 mIU/L (reference range [RR], 0.27-4.2 mIU/L), normal free thyroxine 1.27 ng/dL (16.3 pmol/L) (RR, 0.9-1.7 ng/dL; 11.9-21.8 pmol/L), normal triiodothyronine 89 ng/dL (1.4 nmol/L) (RR, 60-180 ng/dL; 0.9-2.8 nmol/L), and undetectable TRAb. Radioactive iodine scan revealed a solitary “hot” nodule in the right lobe, which changed the diagnosis to solitary toxic thyroid nodule instead of GD (Fig. 1B) [1]. Ultrasound confirmed a 1.8 × 1.0 × 0.9-cm cystic-solid isoechoic nodule (Fig. 1C). The patient was treated with iodine-131 (1.11 MBq; 30 mCi), leading to successful treatment that was confirmed by follow-up scintigraphy showing homogeneous diffuse distribution (Fig. 1D). Marine-Lenhart syndrome was considered, but scintigraphy lacked the typical diffusely increased activity in both parenchyma and affected nodules [2]. This case highlights the importance of thyroid scintigraphy in differentiating between GD and toxic nodular goiter, particularly when TRAb is negative and nodules are present, guiding appropriate treatment decisions.
Cross indicates the patient' suprasternal notch. (A) 24-hour thyroid radioactive iodine test revealed high uptake (57%; normal reference: 8%-32%) and a diffuse distribution, strengthening the diagnosis of Graves disease. (B) A 24-hour thyroid radioactive iodine test showed high uptake of 36% and a solitary “hot” thyroid nodule in the right lobe, supporting the diagnosis of solitary toxic thyroid nodule. (C) Thyroid ultrasound revealed 1 cystic-solid isoechoic nodule in the right lobe, measuring 1.8 × 1.0 × 0.9 cm, reinforcing the diagnosis of toxic thyroid nodule. (D) A 24-hour thyroid radioactive iodine scan after iodine-131 treatment with 1.11 MBq (30 mCi) showed a homogeneous diffuse thyroid distribution, demonstrating a successful treatment of the solitary toxic thyroid nodule.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Ross DS, Burch HB, Cooper DS, et al 2016 American Thyroid Association Guidelines for diagnosis and management of hyperthyroidism and other causes of thyrotoxicosis. Thyroid. 2016;26(10):1343‐1421.27521067 10.1089/thy.2016.0229 · doi ↗ · pubmed ↗
- 2Danno H, Nishihara E, Kousaka K, et al Prevalence and treatment outcomes of Marine-Lenhart syndrome in Japan. Eur Thyroid J. 2021;10(6):461‐467.34950599 10.1159/000510312 PMC 8647058 · doi ↗ · pubmed ↗