A Rare Type of Myeloma: A Case of Monoclonal IgD-Lambda
Recep Kaya, Alperen Burak Kocabıyık, Erdal Kurtoğlu, Volkan Karakuş

TL;DR
This paper discusses a rare and aggressive type of myeloma involving IgD-Lambda, emphasizing the need for better diagnostic methods to avoid misclassification.
Contribution
The paper highlights the importance of including IgD and IgE in myeloma diagnostics to prevent misclassification.
Findings
IgD-MM is rare, aggressive, and often diagnosed in younger males.
IgD-MM is frequently misclassified as light chain myeloma due to standard testing limitations.
Inclusion of IgD and IgE in diagnostics is crucial for accurate classification.
Abstract
An immunoglobulin D-multiple myeloma (IgD-MM) case represents a rare subtype of MM that is often observed in male patients under 65 years of age with an advanced stage at the time of diagnosis. It exhibits an aggressive course and is associated with a short survival period. In IgD-MM, an increase in lambda light chain proteins is expected. Given that IgD and IgE heavy chains are not routinely assessed in standard serum and serum immunofixation electrophoresis (IFE) analyses in MM patients, such cases may be misclassified and monitored as light chain myeloma. Therefore, distinguishing IgD or IgE myeloma from light chain myeloma represents a critical differential diagnosis. This case highlights the necessity of including IgD and IgE in diagnostic evaluations to prevent misclassification as light chain myeloma.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
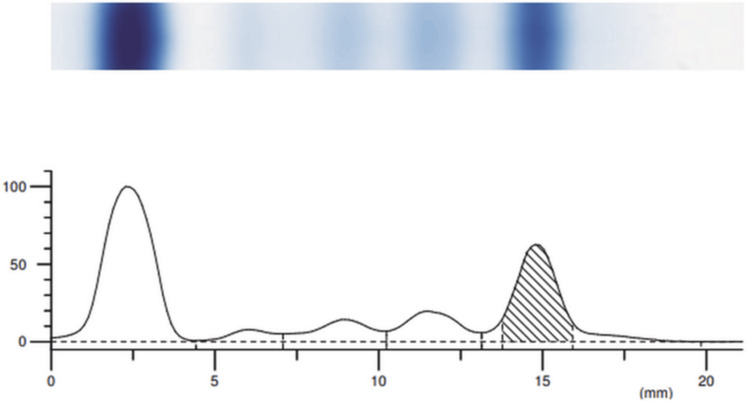 Figure 1
Figure 1| Parameter | Result | Reference Range |
| Blood Urea Nitrogen (BUN) | 36 mg/dl | 8-20 mg/dl |
| Creatinine | 1.74 mg/dl | 0.81-1.44 mg/dl |
| Potassium | 5.2 mmol/L | 3.5-5.1 mmol/L |
| Calcium | 10.8 mg/dl | 8.8-10.6 mg/dl |
| Albumin | 4 g/dl | 3.5-5.2 g/dl |
| Lactate Dehydrogenase (LDH) | 357 U/L | <248 U/L |
| Uric Acid | 11.7 mg/dl | 3.5-7.2 mg/dl |
| Leukocytes | 4000/mm³ | 4000-11000/mm³ |
| Hemoglobin | 6.8 g/dl | 12-16 g/dl (female), 13-18 g/dl (male) |
| Platelets | 99 x 10³/µL | 150-400 x 10³/µL |
| Erythrocyte Sedimentation Rate (ESR) | >140 mmol/hour | 0-20 mmol/hour |
| IgG | 277 mg/dl | 700-1600 mg/dl |
| IgA | 46 mg/dl | 70-400 mg/dl |
| IgM | 18 mg/dl | 40-230 mg/dl |
| Kappa/Lambda Ratio | 0.054 | 0.26-1.65 |
| Kappa Light Chain | 1.64 mg/dl | 6.7-22.4 mg/dl |
| Lambda Light Chain | 30.4 mg/dl | 8.3-27 mg/dl |
| Protein (Band) | Serum IFE | Urine IFE |
| T | 2 distinct bands | Faint signal |
| G (IgG) | No distinct signal | No distinct signal |
| A (IgA) | No distinct signal | No distinct signal |
| M (IgM) | No distinct signal | No distinct signal |
| κ (Kappa) | No distinct signal | No distinct signal |
| λ (Lambda) | Very faint signal (weak band) | Strong signal (clear band) |
| Index | Band | Rel. Area (%) | Conc. (g/dL) | Range (g/dL) |
| 1 | Albumin | 48.73 (L) | 3.66 | 55.80 - 65.00 |
| 2 | Alpha 1 | 3.44 | 0.26 | 2.20 - 4.60 |
| 3 | Alpha 2 | 8.07 (L) | 0.61 | 8.20 - 12.50 |
| 4 | Beta | 10.59 | 0.80 | 7.20 - 14.20 |
| 5 | Gamma | 29.17 | 2.19 | 11.50 - 18.60 |
| Total | 7.52 | |||
| 5 M | Gamma M-spike 1 | 24.59% | 1.85 | |
| Ratio | 0.49 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsMultiple Myeloma Research and Treatments · Peptidase Inhibition and Analysis · Protein Degradation and Inhibitors
Introduction
In patients with multiple myeloma (MM), an increase in the production of monoclonal immunoglobulins (Ig) and free light chains is observed due to malignant plasma cells with abnormal proliferative characteristics, leading to the accumulation of M-protein types. Among M-protein types, IgG-MM is the most common, observed in 52% of cases, followed by IgA-MM at 21%, light chain type at 16%, and the rare IgD-MM type, which is seen in 1-2% of cases [1]. IgD-MM is more closely associated with acute kidney injury, hypercalcemia, and amyloidosis as distinguishing features. In laboratory findings, while the M-protein peak may appear indeterminate in protein electrophoresis, a predominance of lambda light chains is often observed in serum and urine immunofixation electrophoresis (IFE) [2]. In such cases, IgD-MM should always be considered. However, since IgD monoclonal antibody is not assessed in standard IFE testing, IgD clonality - a monoclonal gammopathy rarely seen in MM - may be misinterpreted as light chain myeloma due to its diagnostic challenges. In this report, we present a case of IgD-lambda MM, which is rare and differentiates itself from light chain myeloma.
Case presentation
A 74-year-old male had been experiencing complaints of weakness, fatigue, drowsiness, and muscle weakness for the past month. His medical history was significant for hypertension, but he had no other comorbidities. There was no history of smoking or alcohol use, and no family history of hematologic diseases. Laboratory results revealed anemia, thrombocytopenia, acute kidney failure, hypercalcemia, and elevated sedimentation rate. The laboratory results are presented in Table 1.
A monoclonal lambda band was observed in the serum and urine immunofixation electrophoresis (IFE) (Table 2).
Protein electrophoresis revealed a concentration of 1.85 (g/dl) of M-protein in the gamma band (Figure 1 and Table 3).
Protein electrophoresisThe presence of an M-protein spike in the gamma band
Due to the monoclonal lambda band observed in the serum and urine IFE and the M-protein peak in the gamma band, IgD and IgE were also tested in the serum IFE. The patient's IgD level was 25,500 IU/ml (<100 IU/ml), and IgD and lambda bands were observed in the serum IFE. Bone marrow biopsy pathology revealed that plasma cells accounted for 70% of the nucleated cells, and a diagnosis of monoclonal IgD-lambda multiple myeloma (MM) was established. Given the presence of acute kidney failure, the patient was initiated on a combination of bortezomib, lenalidomide, and dexamethasone was proposed.
Discussion
IgD-MM is one of the rarest subtypes of multiple myeloma, accounting for approximately 2% of cases. It is observed in younger patients and at more advanced stages compared to other subtypes, and its survival rate is shorter [3]. IgD levels in serum are lower compared to other immunoglobulins (0-0.1 g/L), and due to the short half-life of IgD (2.8 days), the M-protein peak in electrophoresis is often minimal or undetectable [4]. In a study conducted by Selene et al. with 166 patients diagnosed with IgD-MM, 136 (81.9%) had the lambda light chain subtype, 30 (18.1%) had the kappa light chain subtype, and the median age of the patients was 54.5-65 years [5]. This study supports our findings by demonstrating a high prevalence of lambda light chain involvement in IgD-MM. While IgD-MM typically presents at an advanced stage in younger patients, with a poorer prognosis compared to other myeloma subtypes, in this case, the patient presented at an older age (74) with prodromal symptoms. In patients admitted for further investigation with suspected multiple myeloma, before diagnosing light chain MM, it is crucial to conduct advanced tests, including IgD and IgE testing in both serum and serum immunofixation electrophoresis. This is particularly important in cases where bands are detected exclusively in the light chain subtype, and a minimal or gamma M protein peak is observed in protein electrophoresis.
Conclusions
In patients admitted with a preliminary diagnosis of multiple myeloma (MM), detailed laboratory results should exclude IgG and IgA MM, and in cases where light chain MM is suspected, IgD and IgE should always be screened in both serum and serum immunofixation electrophoresis. As mentioned earlier, due to the lower levels of IgD and IgE in serum, they may not be detectable in protein electrophoresis, leading to a misdiagnosis of light chain MM. This case underscores the necessity of incorporating IgD and IgE testing into standard diagnostic workups for suspected light chain myeloma to prevent misclassification. Therefore, in order to better understand the diagnosis and treatment process of rare forms of multiple myeloma, larger cohort studies are warranted to refine diagnostic and therapeutic strategies for IgD-MM.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1An extremely rare manifestation of multiple myeloma: an immunoglobulin D secreting testicular plasmacytoma Cureus Sharma A Binazir T Sintow A Lee CC Shaharyar S Tache J 09201710.7759/cureus.1400 PMC 557204428845377 · doi ↗ · pubmed ↗
- 2Immunoglobulin D myeloma--problems with diagnosing and staging (own experience and literature review)Leuk Lymphoma Kuliszkiewicz-Janus M Zimny A Sokolska V Saşiadek M Kuliczkowski K 10291037462005 https://doi.org/10.1080/002689705000964421601955410.1080/00268970500096442 · doi ↗ · pubmed ↗
- 3Unusual myelomas: a review of Ig D and Ig E variants Oncology Pandey S Kyle R 798803272013 https://www.cancernetwork.com/view/unusual-myelomas-review-igd-and-ige-variants 24133829 · pubmed ↗
- 4Characteristics of 15 subjects affected by IGD multiple myeloma and the key role of the laboratory in diagnosis: a retrospective study report and literature review Int J Transl Med Intra J Pezzatti S Brivio R Carpenedo M Romano R Spinoni N vdvd 49850442024
- 5Presentation patterns, diagnostic markers, management strategies, and outcomes of IGD multiple myeloma: a systematic review of literature Cureus Selene II Jose JA Khalil MJ Faisal MS Malik MN 011201910.7759/cureus.4011 PMC 645058831001465 · doi ↗ · pubmed ↗