Desensitization to Tocilizumab in a Patient With Juvenile Idiopathic Arthritis
Rosalaura V Villarreal-González, Diana E Cadenas-García, Adriana Vázquez-Nungaray, Ana V Villarreal-Treviño, Oscar Vidal-Gutiérrez

TL;DR
A child with juvenile arthritis developed an allergic reaction to tocilizumab but was successfully treated with a desensitization protocol.
Contribution
Demonstrates successful desensitization to tocilizumab in a pediatric patient with hypersensitivity.
Findings
The patient experienced a Grade II hypersensitivity reaction after four years of tocilizumab treatment.
A 12-step desensitization protocol allowed continued therapy without further allergic reactions.
Intradermal testing confirmed hypersensitivity, while skin prick testing was negative.
Abstract
Juvenile idiopathic arthritis is the most common chronic inflammatory rheumatic disease in children, classified by the number of affected joints, systemic symptoms, and rheumatoid factor presence. We describe the case of an eight-year-old female with extended oligoarticular juvenile idiopathic arthritis and a strong family history of atopy who developed a Grade II hypersensitivity reaction during a tocilizumab infusion after four years of treatment. Symptoms, including rash, urticaria on the neck and arms, periauricular edema, tachycardia, and hypertension, emerged within 30 minutes of infusion. The reaction was managed with intramuscular epinephrine, intravenous hydrocortisone, and saline, leading to symptom resolution. Skin prick testing was negative, but intradermal testing showed a positive reaction. Due to the drug’s effectiveness in controlling her disease, a desensitization…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
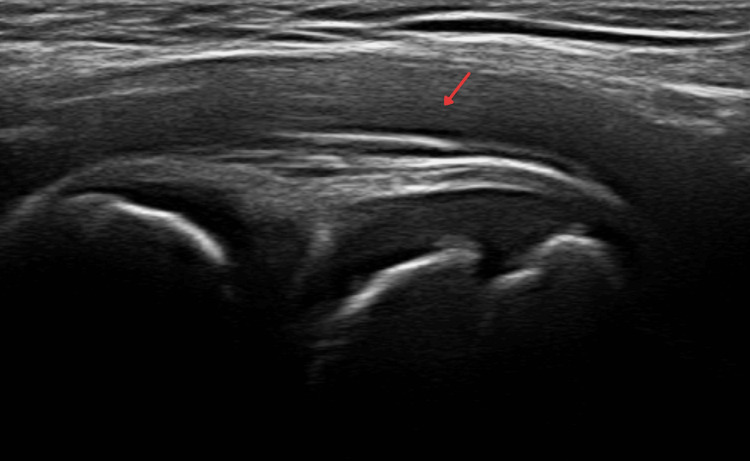 Figure 1
Figure 1 Figure 2
Figure 2| Grade | Severity | Description |
| 1 | Mild | Symptoms are limited to the skin or involve a single organ/system and are mild |
| 2 | Moderate | Symptoms involve at least two organs/systems, but there is no significant drop in blood pressure or oxygen saturation |
| 3 | Severe | Symptoms typically involve at least two organs/systems and there is a significant drop in blood pressure (systolic ≤90 mmHg and/or syncope) and/or oxygen saturation (≤92%) |
| Three bags | Volume (mL) per bag | Concentration (mg/mL) per bag | Amount (mL) of bag infused | Infused dose (mg) per bag |
| Solution 1 | 50 | 0.024 mg/mL | 3.75 | 0.09 mg |
| Solution 2 | 50 | 0.24 mg/mL | 7.5 | 1.8 mg |
| Solution 3 | 100 | 2.38 mg/mL | 100 | 238.11 mg |
| Step | Solution | Rate (mL/hour) | Time (minute) | Volume infused (mL) | Administered dose (mg) | Cumulative dose (mg) |
| 1 | 1 | 1 | 15 | 0.25 | 0.006 mg | 0.006 mg |
| 2 | 1 | 2 | 15 | 0.5 | 0.012 mg | 0.018 mg |
| 3 | 1 | 4 | 15 | 1 | 0.024 mg | 0.042 mg |
| 4 | 1 | 8 | 15 | 2 | 0.048 mg | 0.09 mg |
| 5 | 2 | 2 | 15 | 0.5 | 0.12 mg | 0.21 mg |
| 6 | 2 | 4 | 15 | 1 | 0.24 mg | 0.45 mg |
| 7 | 2 | 8 | 15 | 2 | 0.48 mg | 0.93 mg |
| 8 | 2 | 16 | 15 | 4 | 0.96 mg | 1.89 mg |
| 9 | 3 | 4 | 15 | 1 | 2.38 mg | 4.27 mg |
| 10 | 3 | 8 | 15 | 2 | 4.76 mg | 9.03 mg |
| 11 | 3 | 16 | 15 | 4 | 9.52 mg | 18.55 mg |
| 12 | 3 | 32 | 15 | 93 | 221.45 mg | 240 mg |
| Time: 5.67 h | Total dose: 240 mg | |||||
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAutoimmune and Inflammatory Disorders Research · Urticaria and Related Conditions · Drug-Induced Adverse Reactions
Introduction
Juvenile idiopathic arthritis (JIA) is the most common chronic inflammatory rheumatic condition of childhood, with a global incidence of 1.6 to 23 per 100,000 and a prevalence of 3.8 to 400 per 100,000 [1]. The International League of Associations of Rheumatology classifies subtypes based on the number of affected joints, systemic symptoms, and the presence of rheumatoid factor [2]. Treatment of JIA is categorized into non-biological treatments (anti-inflammatory drugs, corticosteroids, and disease-modifying antirheumatic drugs such as methotrexate, sulfasalazine, and leflunomide) and biological therapies, which target specific proinflammatory cytokines involved in JIA pathogenesis, such as interleukin (IL)-1, IL-6, and tumor necrosis factor [3].
Tocilizumab is a humanized monoclonal antibody targeting IL-6, primarily used in the treatment of systemic and polyarticular JIA. IL-6 plays a critical role in the pathogenesis of JIA by driving inflammation, joint destruction, and systemic manifestations, making it a key target for monoclonal antibody therapy. Hypersensitivity reactions to this monoclonal antibody are estimated to occur in 0.1% to 0.7% of pediatric cases in previous studies [4].
The pathogenesis of hypersensitivity reactions is known to involve cytokine or IgE-mediated release reactions, which include mediators such as histamine, leukotrienes, prostaglandins, tryptase, and platelet-activating factors. Systemic clinical manifestations include urticaria, angioedema, flushing, cough, dyspnea, nausea, vomiting, and hypotension. IgE-mediated anaphylaxis is characterized as a severe, life-threatening systemic hypersensitivity reaction. Additionally, delayed drug reactions with eosinophilia and systemic symptoms have been reported in patients receiving tocilizumab in a few cases [5,6].
Case presentation
We describe the case of an eight-year-old female diagnosed with extended oligoarticular JIA (Figure 1) with a family history of atopy, including allergic rhinitis, atopic dermatitis, urticaria, drug allergy, food allergy, allergy to Hymenoptera sting, and anaphylaxis.
Ultrasound of the right hip joint at the time of juvenile idiopathic arthritis diagnosis.Bilateral hip joint effusion, more prominent on the right side. No Doppler power signal was detected (exudative synovitis). The remainder of the study was within normal parameters.
During a tocilizumab infusion, 30 minutes into the procedure after four years of treatment, the patient developed a hypersensitivity reaction, presenting with a rash, urticaria on the neck and arms, periauricular edema, tachycardia at 115 beats/minute, and hypertension at 90/50 mmHg (with a baseline of 60/30 mmHg). The hypersensitivity reaction was classified as Grade II on Brown’s scale (Table 1). Epinephrine 0.50 mg was administered intramuscularly, along with 250 mL of physiological saline and 30 mg of hydrocortisone intravenously, resulting in the resolution of symptoms.
Two weeks later, a skin prick test of tocilizumab with a concentration of 20 mg/mL was performed with a negative result. Intradermal skin tests at 0.2 mg/mL were positive (8 × 8 mm) compared to the negative control (glycerinated solution 2 × 2 mm).
Due to the adequate response of the disease to the monoclonal antibody, it was decided to initiate a desensitization protocol to tocilizumab 240 mg, consisting of three bags and 12 steps over 5.67 hours (Tables 2, 3). Premedication with levocetirizine 5 mg orally was administered one hour before the infusion. The procedure was completed successfully without any hypersensitivity reactions, repeated every four weeks (Figure 2).
MRI study (T1) after five cycles of tocilizumab desensitization, with the disease in a non-active state.The lower dorsal region, lumbar spine, sacrum, and coccyx show no abnormalities in vertebral bodies or intervertebral spaces. The spinal cord and cauda equina appear normal. The sacroiliac and hip joints show no alterations and no evidence of edema or joint effusion. The thigh muscles up to the mid-third of the femur show no abnormalities, and the signal intensity of the femur up to the mid-third is normal.
Discussion
JIA is classified into oligoarticular (persistent or extended), polyarticular (rheumatoid factor positive or negative), systemic, psoriatic arthritis, and enthesitis-related arthritis. The type of JIA influences genetic susceptibility and disease severity [3].
We describe a pediatric patient with extended oligoarticular JIA who developed a hypersensitivity reaction to tocilizumab and underwent a desensitization protocol. Hypersensitivity reactions to monoclonals can be infusion-related reactions, cytokine release reactions, type I reactions (which can be IgE-mediated or non-IgE-mediated), type III reactions, and late type IV reactions. Infusion-related reactions and cytokine release reactions to monoclonal antibodies can occur from the first infusion and may present with moderate to severe symptoms [8].
In a recent study of patients with JIA treated with tocilizumab, hypersensitivity reactions were reported to occur within 35 minutes to five hours after administration, with symptoms including fever, respiratory symptoms (cough, desaturation), gastrointestinal symptoms (vomiting, abdominal pain), and cardiovascular symptoms (tachycardia, bradycardia, hypotension). Risk factors for hypersensitivity reactions to tocilizumab included younger age and higher disease activity [9].
The first report of rapid desensitization of a pediatric patient in a Latin American population was of eight steps, with a dilution of tocilizumab (0.47 mg/mL in 250 mL of 0.9% physiological solution), successfully performed [10]. There are few reported cases in the literature of desensitization to tocilizumab in pediatric patients. One such case involved a 15-year-old boy with JIA who presented with Grade 2 anaphylaxis after the second dose of tocilizumab. The desensitization protocol consisted of 12 steps with three bags of tocilizumab (600 mg), and lasted five hours and 45 minutes, with no adverse events [11].
Currently, monoclonal antibodies constitute a cornerstone in the treatment of numerous diseases; therefore, an increasing number of adverse reactions are being documented, underscoring the importance of desensitization protocols.
Conclusions
This case underscores the challenges of managing hypersensitivity reactions in patients undergoing biologic therapy. Despite four years of effective treatment with tocilizumab for extended oligoarticular JIA, the patient developed a Grade II hypersensitivity reaction, which was promptly resolved with epinephrine, hydrocortisone, and physiological saline. Therefore, the implementation of a desensitization protocol was required. The successful desensitization process enabled the continuation of treatment without further hypersensitivity episodes, highlighting the importance of such protocols for patients reliant on biologic therapies. With the increasing use of monoclonal antibodies in the treatment of various diseases, this case emphasizes the necessity of proactive measures and individualized strategies to manage hypersensitivity reactions while ensuring patient safety and therapeutic efficacy.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Prevalence and titres of antinuclear antibodies in juvenile idiopathic arthritis: a systematic review and meta-analysis Autoimmun Rev Storwick JA Brett AC Buhler K 1030862120223539827210.1016/j.autrev.2022.103086 · doi ↗ · pubmed ↗
- 2Juvenile idiopathic arthritis: from aetiopathogenesis to therapeutic approaches Pediatr Rheumatol Online J Zaripova LN Midgley A Christmas SE Beresford MW Baildam EM Oldershaw RA 1351920213442584210.1186/s 12969-021-00629-8PMC 8383464 · doi ↗ · pubmed ↗
- 3Biologics in juvenile idiopathic arthritis-main advantages and major challenges: a narrative review Arch Rheumatol Adrovic A Yildiz M Köker O Şahin S Barut K KasapçopurÖ 1461573620213404658410.46497/Arch Rheumatol.2021.7953 PMC 8140868 · doi ↗ · pubmed ↗
- 4Severe hypersensitivity reactions to biological drugs in children with rheumatic diseases Pediatr Allergy Immunol Soyer O Demir S Bilginer Y 8338403020193141931110.1111/pai.13114 · doi ↗ · pubmed ↗
- 5Management of hypersensitivity reactions to tocilizumab Clin Exp Allergy Tétu P Hamelin A Moguelet P Barbaud A Soria A 7497524820182960380910.1111/cea.13142 · doi ↗ · pubmed ↗
- 6Hypersensitivity to biological treatments in juvenile idiopathic arthritis: how should it be managed?J Clin Med Kasap Cuceoglu M Basaran O Soyer O Ozen S 72911120223655590810.3390/jcm 11247291 PMC 9785630 · doi ↗ · pubmed ↗
- 7Current knowledge and management of hypersensitivity reactions to monoclonal antibodies J Allergy Clin Immunol Pract Picard M Galvão VR 600609520172811005610.1016/j.jaip.2016.12.001 · doi ↗ · pubmed ↗
- 8Hypersensitivity reactions to therapeutic monoclonal antibodies: phenotypes and endotypes J Allergy Clin Immunol Isabwe GA Garcia Neuer M de Las Vecillas Sanchez L Lynch DM Marquis K Castells M 15917014220182951842710.1016/j.jaci.2018.02.018 · doi ↗ · pubmed ↗