Unmasking POEMS (Polyneuropathy, Organomegaly, Endocrinopathy, Monoclonal Gammopathy, and Skin Changes) Syndrome in a Heart Failure Patient: A Diagnostic Challenge
Frances Ogunnaya, Mohamed E Kambal, Thowaiba E Ali, Dina Elsayed, Jose Bustillo

TL;DR
This paper describes a rare case of POEMS syndrome in a patient initially diagnosed with heart failure, highlighting the diagnostic challenges of the condition.
Contribution
The paper presents a unique case linking heart failure symptoms with POEMS syndrome, which is rarely reported in the literature.
Findings
A 47-year-old man initially diagnosed with heart failure was found to have POEMS syndrome.
The diagnosis was confirmed through monoclonal gammopathy, sclerotic bone lesions, and Castleman's disease.
The case underscores the difficulty in diagnosing POEMS syndrome due to overlapping symptoms with other conditions.
Abstract
POEMS (polyneuropathy, organomegaly, endocrinopathy, monoclonal gammopathy, and skin changes) syndrome remains poorly understood. It is a paraneoplastic syndrome caused by underlying plasma cell dyscrasia, and there is uncertainty about the features required to establish the diagnosis, treatment efficacy, and prognosis. Almost all patients have polyneuropathy or plasma cell disorder, and approximately one-third have Castleman's disease. Peripheral neuropathy often serves as the primary presenting complaint. While extensive discussions exist regarding POEMS syndrome diagnosis and treatment advancements, literature reports of heart failure symptoms associated with POEMS syndrome are scarce. In this article, we present a case of newly diagnosed POEMS syndrome in a 47-year-old man who initially presented with bilateral lower extremities edema and weakness. Although the initial workup was…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
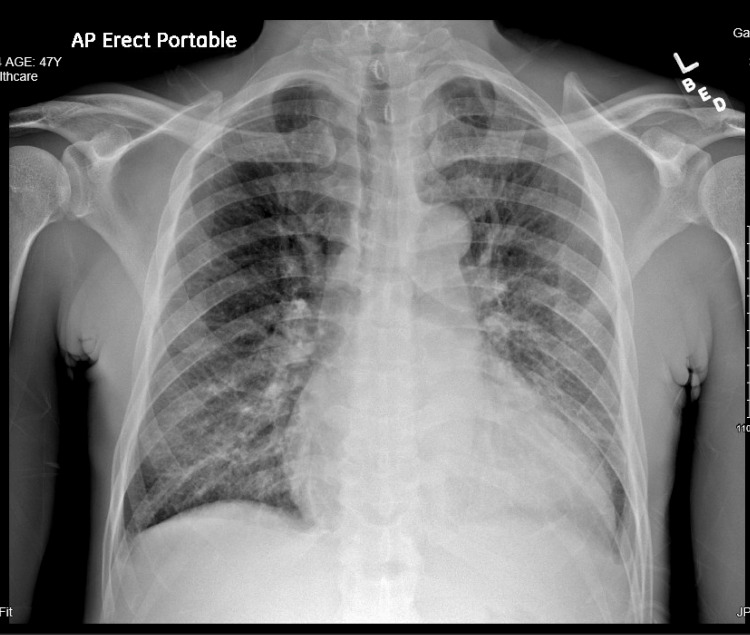 Figure 1
Figure 1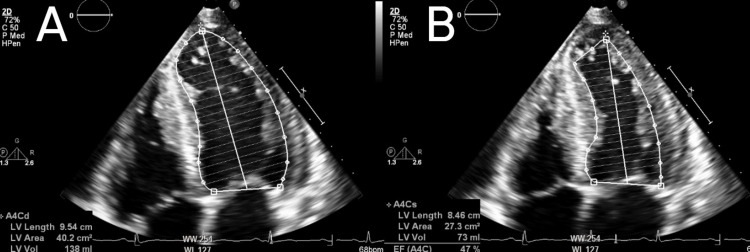 Figure 2
Figure 2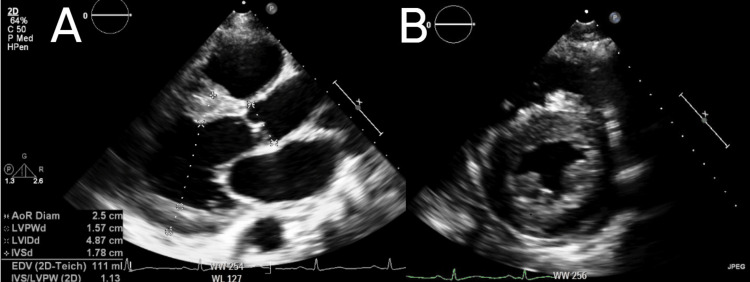 Figure 3
Figure 3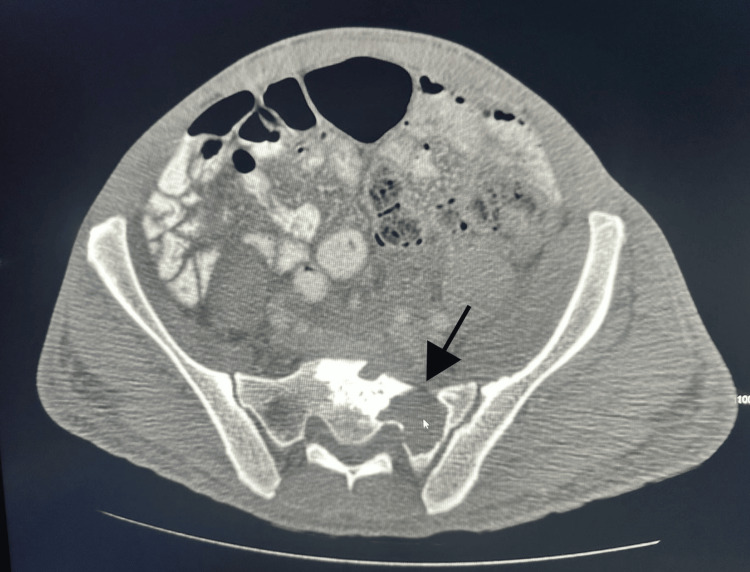 Figure 4
Figure 4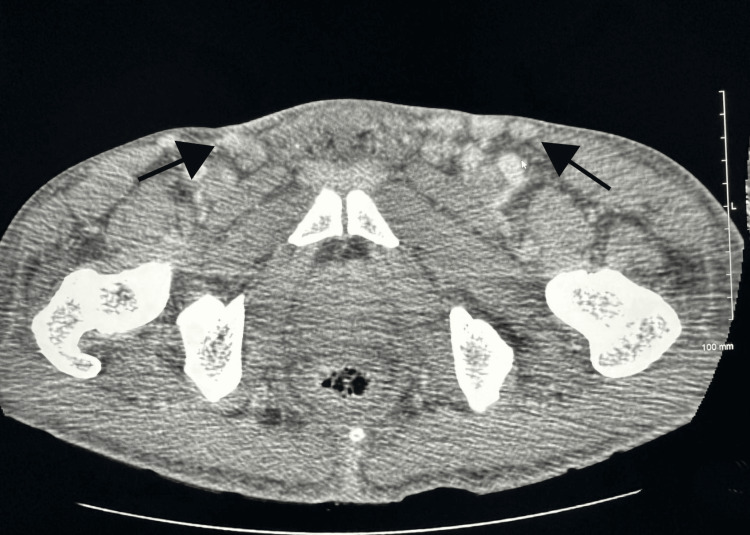 Figure 5
Figure 5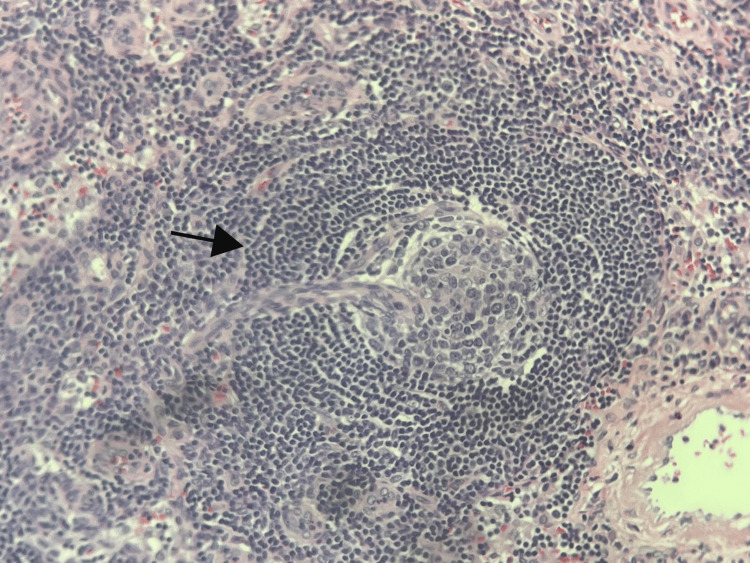 Figure 6
Figure 6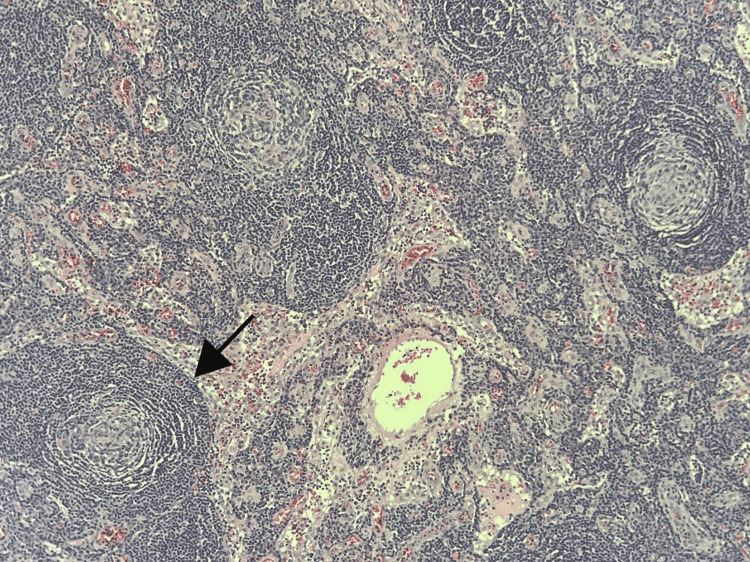 Figure 7
Figure 7| Reference | Age, gender | Presenting symptoms | Initial presumed diagnosis | Cardiac involvement |
| Pei et al. (2015) [ | 61-year-old, female | Fingers paresthesia and lower limb edema | No initial diagnosis was made | Left ventricular hypertrophy with moderate systolic dysfunction |
| Witoonpanich et al. (2005) [ | 16-year-old, male | Bilateral lower extremity weakness | CIDP | Left ventricular enlargement with slightly reduced left ventricular systolic function |
| Wang et al. (2022) [ | 31-year-old, female | Chest pain, dyspnea, and lower extremity edema | No initial diagnosis was made | Left ventricular diastolic dysfunction, pericardial effusion, enlarged left atria |
| Yokokawa et al. (2013) [ | 67-year-old, male | Dyspnea and lower extremity edema | Heart failure | Cardiomegaly, left ventricular diastolic dysfunction and severe tricuspid regurgitation |
| Current case | 47-year-old, male | bilateral lower extremity weakness and edema and dyspnea | Heart failure | Left ventricular hypertrophy with mildly reduced left ventricular ejection fraction |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPeripheral Neuropathies and Disorders · Hereditary Neurological Disorders · Myasthenia Gravis and Thymoma
Introduction
POEMS (polyneuropathy, organomegaly, endocrinopathy, monoclonal gammopathy, and skin changes) syndrome, also known as osteosclerotic myeloma, Crow-Fukase syndrome, or Takatsuki syndrome is a rare paraneoplastic syndrome associated with plasma cell dyscrasias [1]. The first documented case of what is now known as POEMS syndrome was Scheinker's autopsy case in 1938, and Bardwick et al. created the acronym POEMS in 1980 to represent a syndrome that includes polyneuropathy, organomegaly, endocrinopathy, M protein, and skin changes [2]. However, the acronym does not include certain associated features, such as sclerotic bone lesions, Castleman's disease, papilledema, thrombocytosis, peripheral edema, ascites, effusions, fatigue, clubbing, weight loss, polycythemia, and hyperhidrosis. Not all of these features are necessary for diagnosis.
The pathogenesis of POEMS syndrome is thought to involve the overproduction of inflammatory cytokines, such as TNF-α, IL-1β, IL-6, and vascular endothelial growth factor (VEGF) [3]. It predominantly affects males and typically presents in the fifth or sixth decade of life. Diagnosing POEMS syndrome can be challenging because no single test definitively establishes the diagnosis. Furthermore, because the disease affects multiple systems, its signs and symptoms may not be obvious at the initial presentation, causing diagnostic delays.
POEMS syndrome is sometimes mistaken for other conditions, such as monoclonal gammopathies and chronic inflammatory demyelinating polyneuropathy, both of which can present with peripheral neuropathy [4]. We present the case of a patient who initially presented with heart failure exacerbation and lower extremity weakness, ultimately leading to the diagnosis of POEMS syndrome.
Case presentation
A 47-year-old man with a medical history of hypertension and chronic kidney disease (stage 1) presented to our emergency room with complaints of progressive bilateral lower extremity weakness, swelling, heaviness, and exertional dyspnea for a year duration. He attributed his weakness to the heaviness caused by the edema. He had not seen a primary care physician in over a year due to the COVID-19 pandemic.
On arrival, his vital signs were as follows: blood pressure, 124/83 mm Hg; heart rate, 78 beats per minute; respiratory rate, 19 breaths per minute; oxygen saturation, 100% on room air and he was afebrile.
Physical examination revealed rales on auscultation of the lung, bilateral lower extremity pitting edema extending to the knees, significant muscle atrophy and decreased reflexes in lower extremities bilaterally and bilateral foot drop. Laboratory findings revealed a B-type natriuretic peptide (BNP) level of 248 pg/ml (reference range: <100 pg/ml), a creatinine level of 1.510 mg/dl (reference range: 0.700-1.300 mg/dl), an albumin level of 3.2 g/dl (reference range: 3.4-5.0 g/dl), an alanine aminotransferase (ALT) level of 12 units/L (reference range: <61 units/L), and an aspartate aminotransferase (AST) level of 4 units/L (reference range: <37 units/L).
A single anteroposterior chest radiograph was performed that showed cardiomegaly with pulmonary vascular congestion (Figure 1).
Chest radiograph, in an anteroposterior view.Enlarged cardiac silhouette, accompanied by bilateral increased interstitial markings and cephalization of pulmonary vessels, indicative of pulmonary vascular congestion.
A transthoracic echocardiogram demonstrated left ventricular hypertrophy (Figures 2A, 2B) with a mildly reduced left ventricular ejection fraction of 47% (Figures 3A, 3B) and normal right ventricular size and function.
Apical four-chamber view which was used in Simpson's biplane method of disks to estimate mildly reduced left ventricular ejection fraction of 47% on echocardiogram.(A) Image shows left ventricular end-diastolic volume; (B) image shows left ventricular end-systolic volume.
Echocardiogram demonstrating evidence of moderate concentric left ventricular hypertrophy with normal LV cavity size.(A) Parasternal long-axis view on echocardiogram; (B) parasternal short-axis view on echocardiogram.LV: left ventricle.
As a result, the patient was admitted to the medical floors due to difficulty walking caused by lower extremity edema related to decompensated heart failure. Diuresis was initiated with intravenous frusemide 80 mg daily. However, despite improvements in his respiration and lower extremity edema, his weakness persisted.
An MRI of the brain and spine was performed to rule out central causes of weakness and yielded unremarkable findings. The patient was then discharged to a sub-acute rehabilitation center, with a scheduled follow-up appointment with neurology for further evaluation.
Three months later, and just before his follow-up appointment, the patient returned to the emergency room with new symptoms. He reported increased abdominal girth, discomfort, and an inability to open his left hand fully. We noticed skin hyperpigmentation, persistent bilateral foot drop, and bilateral claw hand deformity, which was worse on the left hand. An abdominal CT scan revealed anasarca and a 5 cm sacral soft tissue mass. In addition, a lytic lesion was found at the lumbosacral spine (Figure 4), as well as bilateral inguinal and pelvic lymphadenopathy (Figure 5).
CT of the abdomen and pelvis showing a large lytic lesion in the left sacral bone (black arrow).CT: computed tomography.
CT of the abdomen and pelvis showing enlarged inguinal lymph nodes (black arrows).CT: computed tomography.
The initial differential diagnosis for the patient's weakness included peripheral neuropathy caused by chronic inflammatory demyelinating polyneuropathy, toxic exposure, vitamin deficiency, or monoclonal gammopathy. To further investigate, additional tests were performed to rule out the aforementioned differential diagnoses. These revealed vitamin B12 deficiency with vitamin B12 level of 181 pg/ml (reference range: 193-986 pg/ml), and serum protein electrophoresis (SPEP) showed an elevated spike in the gamma globulin region with a predominance of IgG. The patient underwent a CT-guided biopsy of the sacral mass, which revealed IgG-lambda restricted plasmacytoma. He also had an excisional axillary lymph node biopsy, which revealed histologic characteristics consistent with Castleman's disease, specifically the hyaline vascular variant (Figures 6, 7). Notably, human herpesvirus-8 (HHV-8) immunostaining yielded negative results.
Axillary lymph node biopsy showing mantle zones arranged in concentric rings (black arrow) and penetrating sclerotic blood vessels characteristic of hyaline vascular Castleman's disease.
Axillary lymph node biopsy showing germinal centers with concentric onion-like layering of surrounding lymphoid cells (black arrow) seen in Castleman's disease.
Further testing revealed a remarkably elevated vascular endothelial growth factor receptor (VEGFR) level of 8243. The patient was diagnosed with POEMS syndrome based on a constellation of symptoms and signs including polyneuropathy, monoclonal gammopathy, Castleman's disease, volume overload, skin changes, weight loss, and low vitamin B12 levels.
Initially, the patient received treatment with bortezomib, dexamethasone, and vitamin B12 injections. However, bortezomib had to be discontinued due to severe neuropathy. Subsequently, the patient was switched to daratumumab, lenalidomide, and dexamethasone, resulting in improvements in lower extremity edema, dyspnea, walking ability, and overall functional status. Later, the patient underwent stem cell transplantation, which led to significant improvement. Currently, the patient is receiving monthly maintenance subcutaneous injections of daratumumab.
Discussion
Diagnosing POEMS syndrome can be extremely challenging, even when a patient presents with a classic set of symptoms. A review of the literature shows that diagnosis of POEMS syndrome is usually delayed by approximately 15 months often it is misdiagnosed with chronic inflammatory demyelinating polyneuropathy and metastatic cancer [5]. Typically, in cases involving peripheral neuropathy, further investigation may lead to the suspicion of POEMS syndrome. However, if neuropathy is not prominent, the diagnosis might be missed unless there is a high level of suspicion.
The diagnostic criteria for POEMS syndrome include two mandatory criteria and three major criteria, one of which must be present. Additionally, there are six minor criteria, one of which must also be met [6]. The mandatory criteria encompass polyneuropathy and monoclonal gammopathy. The major criteria include Castleman's disease, sclerotic bone lesions, and elevated VEGF levels. The minor criteria involve organomegaly, volume overload, endocrinopathy, skin changes, papilledema, and thrombosis. Additional markers, such as low vitamin B12 levels, can provide further support for the diagnosis.
Despite the extensive investigation into various aspects of POEMS syndrome, there remains a significant gap in comprehensive data regarding cardiac involvement. To address this limitation, we have included a table from studies in our literature review in this paper to shed further light on this aspect (Table 1).
Our review of the literature shows that cardiac involvement in POEMS syndrome can manifest in diverse ways, including left ventricular hypertrophy, systolic dysfunction, diastolic dysfunction, pericardial effusion, and arrhythmias. It is important to recognize that no single presentation or pattern is specific enough to definitively suspect POEMS syndrome.
In our patient’s case, despite later fulfilling the diagnostic criteria, the initial presentation did not immediately suggest investigating POEMS syndrome. Initially, he presented with volume overload, which, along with his long-standing hypertension and echocardiogram findings, was attributed to congestive heart failure exacerbation. Interestingly, the lower extremity edema also masked his weakness, as he primarily perceived it as heaviness related to the edema and physical deconditioning.
However, as other systemic signs arose and neuropathy became more prominent, particularly with the resolution of the edema and the development of claw hands, further investigations were initiated to explore other potential causes. It is essential to note that volume overload, a symptom commonly seen in heart failure, is also part of the minor criteria in POEMS syndrome.
Vitamin B12 deficiency also poses an additional challenge in diagnosing POEMS syndrome. As its presence can complicate the diagnostic process, vitamin B12 deficiency alone can also cause peripheral neuropathy, further adding to the complexity of the diagnosis.
Conclusions
While there is a well-defined diagnostic criterion for identifying POEMS syndrome, there is no single symptom or test that would raise the initial suspicion for POEMS syndrome. it is crucial to maintain a vigilant approach to initiate the necessary investigations and meet the diagnostic requirements. When encountering symptoms and signs like peripheral neuropathy and monoclonal gammopathy in the context of heart failure, clinicians should consider the possibility of POEMS syndrome.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1POEMS syndrome Hematology Am Soc Hematol Educ Program Dispenzieri A 36036720052005 https://doi.org/10.1182/asheducation-2005.1.36010.1182/asheducation-2005.1.36016304404 · doi ↗ · pubmed ↗
- 2Plasma cell dyscrasia with polyneuropathy, organomegaly, endocrinopathy, M protein, and skin changes: the POEMS syndrome. Report on two cases and a review of the literature Medicine (Baltimore) Bardwick PA Zvaifler NJ Gill GN Newman D Greenway GD Resnick DL 311322591980624872010.1097/00005792-198007000-00006 · doi ↗ · pubmed ↗
- 3Overproduction of vascular endothelial growth factor/vascular permeability factor is causative in Crow-Fukase (POEMS) syndrome Muscle Nerve Watanabe O Maruyama I Arimura K 13901397211998977166110.1002/(sici)1097-4598(199811)21:11<1390::aid-mus 5>3.0.co;2-4 · doi ↗ · pubmed ↗
- 4Update on the diagnosis and treatment of POEMS (polyneuropathy, organomegaly, endocrinopathy, monoclonal gammopathy, and skin changes) Syndrome: a review JAMA Oncol Khouri J Nakashima M Wong S 13831391720213408109710.1001/jamaoncol.2021.0586 · doi ↗ · pubmed ↗
- 5Clinical characteristics, risk factors, and outcomes of POEMS syndrome: a longitudinal cohort study Neurology Keddie S Foldes D Caimari F 079952020 https://doi.org/10.1212/wnl.000000000000994010.1212/WNL.000000000000994032606227 · doi ↗ · pubmed ↗
- 6POEMS syndrome: 2019 update on diagnosis, risk-stratification, and management Am J Hematol Dispenzieri A 812827942019 https://doi.org/10.1002/ajh.254953101213910.1002/ajh.25495 · doi ↗ · pubmed ↗
- 7Cardiac involvement in a patient with POEMS syndrome detected using cardiac magnetic resonance imaging Int Heart J Pei G Yang D Sun J Luo Y Yan J Chen Y 571573562015 https://www.jstage.jst.go.jp/article/ihj/56/5/56_15-038/_article/-char/en 2634651810.1536/ihj.15-038 · doi ↗ · pubmed ↗
- 8POEMS syndrome with venous sinus thrombosis and visual failure: a case report J Med Assoc Thai Witoonpanich R Phankhian S Jootar S Poonyathalang A Worapongpaiboon S Phudhichareonrat S Chanplakorn N 690694882005 https://medassocthai.org/journal/files/Vol 88_No 5_690.pdf 16149691 · pubmed ↗