Dynamic Velocity Tracking in the Left‐Ventricular Outflow Track Using Four‐Dimensional 4D Flow for the Assessment of Left Ventricular Outflow Track Obstruction
Chris Sawh, Pankaj Garg

TL;DR
This paper shows how 4D flow CMR can track blood flow in the heart to detect blockages when other methods fail.
Contribution
The novel use of stress 4D flow CMR for diagnosing dynamic left ventricular outflow track obstruction is introduced.
Findings
Stress 4D flow CMR provides accurate diagnosis of LVOT obstruction.
It enables detailed assessment of hemodynamics when echocardiography is insufficient.
The method improves clinical decision-making in complex cardiac cases.
Abstract
Stress 4D flow CMR is a powerful non‐invasive tool for diagnosing and localizing dynamic LVOT obstruction. By quantifying peak velocities and flow patterns under stress, it provides critical insights into hemodynamics, especially when echocardiography is limited, enabling accurate diagnosis and improved clinical decision‐making in complex cases.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
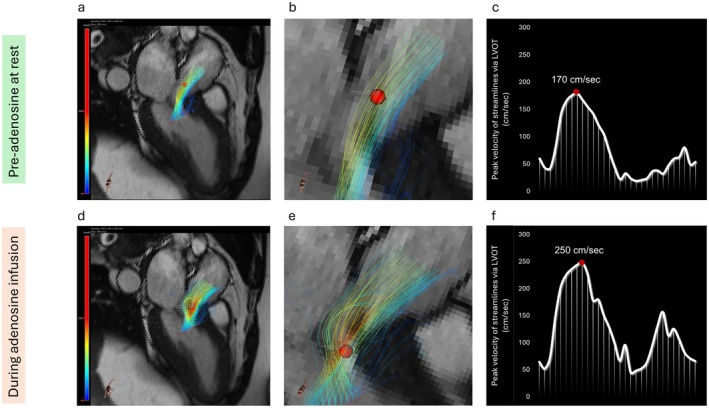 Figure 1
Figure 1- —Wellcome Trust 10.13039/100010269
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCardiovascular Function and Risk Factors · Cardiac Arrhythmias and Treatments · Atrial Fibrillation Management and Outcomes
A 58‐year‐old woman presented to the cardiology outpatient clinic with progressive shortness of breath. Her medical history included diabetes mellitus, hypertension, and hypercholesterolaemia. Initial electrocardiography showed sinus rhythm with T‐wave inversion in leads I and aVL. Transthoracic echocardiography demonstrated a normal‐sized left ventricle with preserved systolic function; however, acoustic windows were suboptimal due to body habitus. A sigmoidal basal septum was noted, resulting in systolic anterior motion (SAM) of the mitral valve and turbulent flow in the left ventricular outflow tract (LVOT), though quantification was not possible due to alignment challenges. The right ventricle was structurally and functionally normal, and no significant valvular pathology was identified.
To further evaluate cardiac function and investigate myocardial ischaemia, the patient underwent cardiovascular magnetic resonance (CMR) imaging with first‐pass perfusion and 4D flow assessment [1, 2]. Given the echocardiographic suspicion of LVOT obstruction, a tailored protocol incorporating rest and peak‐stress 4D flow CMR was applied. Dynamic velocity tracking of three‐dimensional streamlines enabled precise evaluation of flow patterns and velocities in the LVOT.
At rest, blood flow through the LVOT was smooth, with a peak velocity of 170 cm/s located just below the aortic valve, within normal limits. During adenosine‐induced hyperaemia, first‐pass perfusion imaging revealed myocardial ischaemia in the anterolateral wall (Figure 1a–c). Stress 4D flow CMR demonstrated marked flow acceleration with a high‐velocity jet near the septal bulge, coinciding with a rise in peak velocity to 250 cm/s and increased streamline density (Figure 1d–f). These findings confirmed dynamic LVOT obstruction under stress, with clear spatial localization of flow disturbance.
This case underscores the clinical value of stress 4D flow CMR as a novel, non‐invasive modality for the comprehensive assessment of suspected LVOT obstruction. By dynamically quantifying flow velocities and identifying the precise location of obstruction, this technique provides critical insights into the hemodynamics of flow acceleration and its pathophysiological impact.
The role of CMR imaging in the assessment of cardiovascular diseases is expanding [3]. In particular, 4D flow CMR is increasingly gaining attention as it circumvents issues of routine Doppler assessment, mainly the operator dependence of flow and velocity quantification. In slow flow aortic stenosis (AS), this technique may enhance the precision of stenosis severity assessment by quantifying pressure gradients during increased cardiac output. For LVOT obstruction in hypertrophic cardiomyopathy (HCM), stress 4D flow CMR can reveal the dynamic nature of obstruction under stress conditions, providing critical insights for patient stratification.
1
Stress 4D flow CMR faces some barriers to clinical adoption. The 5‐to‐10‐min acquisition time complicates maintaining consistent physiological stress, particularly during exercise. Although pharmacological stressors mitigate these, ensuring steady stress levels throughout the scan remains difficult. Additionally, the lack of standardized 4D flow sequences across imaging centres and the scarcity of expertise hinder its broader translation into routine practice.
To our knowledge, this is the first reported case utilizing stress 4D flow CMR to diagnose and localize dynamic LVOT obstruction with concurrent evidence of myocardial ischaemia. This approach demonstrates its potential to enhance diagnostic accuracy and guide tailored management strategies in complex cardiomyopathies.
Author Contributions
Pankaj Garg: data curation, formal analysis, methodology, project administration, software, writing – review and editing. Chris Sawh: conceptualization, data curation, investigation, methodology, resources, supervision, validation, writing – original draft.
Consent
The authors confirm that written consent for submission and publication of this case report, including images and associated text, has been obtained from the patient in line with COPE guidance.
Conflicts of Interest
P.G. has a clinical advisor role with Medis Medical Imaging and Pie Medical Imaging. P.G. consults for Edward Lifesciences and Anteris.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1P. Njoku , C. Grafton‐Clarke , H. Assadi , et al., “Validation of Time‐Resolved, Automated Peak Trans‐Mitral Velocity Tracking: Two Center Four‐Dimensional Flow Cardiovascular Magnetic Resonance Study,” International Journal of Cardiology 364 (2022): 148–156.35716937 10.1016/j.ijcard.2022.06.032 · doi ↗ · pubmed ↗
- 2R. J. van der Geest and P. Garg , “Advanced Analysis Techniques for Intra‐Cardiac Flow Evaluation From 4D Flow MRI,” Current Radiology Reports 4 (2016): 38.27390626 10.1007/s 40134-016-0167-7PMC 4875115 · doi ↗ · pubmed ↗
- 3A. Chowdhary , P. Garg , A. Das , M. S. Nazir , and S. Plein , “Cardiovascular Magnetic Resonance Imaging: Emerging Techniques and Applications,” Heart 107, no. 9 (2021): 697–704.33402364 10.1136/heartjnl-2019-315669 PMC 7611390 · doi ↗ · pubmed ↗