Understanding experiences of optimal survivorship care: findings from a population-based study of cancer survivors
Victoria White, Karla Gough, Eli Ristevski, Karolina Lisy, Kate Webber, Jon Emery, Peter Gibbs, Maarten IJzerman, Nikki Davis, Michael Jefford

TL;DR
This study explores cancer survivors' experiences with follow-up care in Australia and finds that only 40% report receiving optimal care, with variations based on demographics and cancer type.
Contribution
The study provides population-based insights into survivorship care experiences and identifies sociodemographic and clinical factors associated with optimal care.
Findings
Only 40% of cancer survivors reported receiving optimal survivorship care.
Optimal care was most reported for information about tests/check-ups and least for new symptoms needing investigation.
Male survivors, those with certain cancers, and those in lower socioeconomic areas were more likely to report optimal care.
Abstract
Multiple frameworks describing optimal cancer survivorship care recommend the development of systems to monitor delivery of quality care. This study reports the experiences of cancer survivorship care in Australia and examines associations with patient-level sociodemographic and clinical characteristics. People aged ≥ 16 years, with any cancer receiving cancer care in a Victorian public hospital in 2018, were invited to complete a survey assessing care experiences. Seven items assessed follow-up care experiences with optimal care indicated by the response: ‘Yes, definitely received’, and sub-optimal care by responses ‘Yes, I think so’, ‘No’, and ‘Not sure’. A composite score was derived with optimal care defined as positive experiences on the majority of items. Sociodemographic and clinical factors associated with optimal care were examined using multivariable logistic regression. Of…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
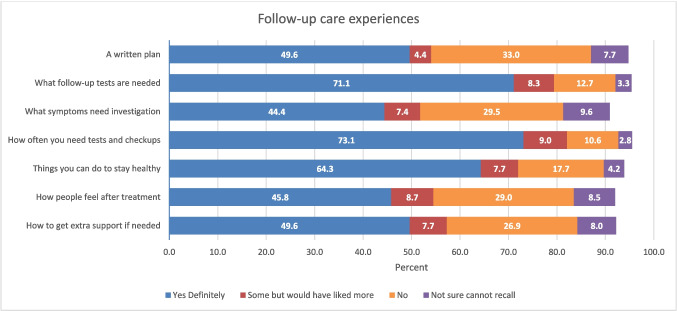 Figure 1
Figure 1- —Victorian Cancer Agency, Australia
- —http://dx.doi.org/10.13039/501100000925National Health and Medical Research Council
- —Deakin University
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCancer survivorship and care · Palliative Care and End-of-Life Issues · Family Support in Illness
Introduction
Worldwide, the number of cancer survivors is growing [1]. Although many survivors recover well after their acute cancer care, a substantial proportion experience ongoing difficulties including living with long-term side-effects and reduced quality of life (QoL) [2]. Supportive care needs are also high which includes needs relating to managing fear of cancer recurrence [3, 4]. To assist patients to manage their recovery and monitor for recurrence and new cancers, as well as for physical and psychosocial effects, follow-up care is generally recommended, which could be with the cancer care team and/or their general practitioner [5–7]. Since the Institute of Medicine’s report on the follow-up care needs of cancer survivors [8], a growing number of organisations have developed survivorship care recommendations that incorporate a holistic approach to care. These recommendations often call for the development of survivorship care plans that include information about type and frequency of medical appointments and tests, monitoring and management of adverse events, identifying and addressing psychosocial needs, and lifestyle recommendations to promote optimal health outcomes [9, 10]. In Australia, a Survivorship Quality Care Framework has been developed that recognises the need to monitor and manage the physical, emotional, practical, and social effects of cancer and its treatment, as well as monitoring for recurrence and new cancers [5]. A recent proposal for national survivorship care standards in the US promoted the need for the health system to adopt a multidisciplinary approach to survivorship care to enable it to deliver care that focuses on meeting the survivor’s physical, emotional, and social needs [11].
A key recommendation in these different frameworks is the development of systems to monitor progress towards delivering quality survivorship care. Nekhlyudov and colleagues have proposed a number of indicators to assess quality of survivorship care including patient-reported experience measures (PREMs) assessing access to services, communication, and care coordination [6] which is in line with calls to understand patients’ experiences as part of assessing quality of care [5, 12–16]. Although numerous studies have assessed experiences of care during treatment [17–21], there is less information on survivorship care experiences with studies in this area mainly focusing on the use of survivorship care plans (see for example [22–24]). Several studies from the US have used the Medical Expenditure Panel Survey (MEPS)-Experiences with Cancer Survivorship module to examine survivorship care experiences. Data from the 2011 survey found that 62% of survivors received detailed information about monitoring and follow-up tests needed but only 29% received information about emotional/social needs [25]. Similar results were found in the 2016 MEPS [26].
Several studies have suggested that survivorship care experiences can differ by disease and sociodemographic factors, although the influence of these factors may differ between countries. Work from the US has found those from lower socioeconomic status (SES) groups, and those from minority ethnic groups are less likely to report receiving quality survivorship care or receiving detailed follow-up care information [25, 27]. In contrast, an Australian study of colorectal patients diagnosed in 2012/2013 found that those from a non-English speaking background were more likely to report receiving a written follow-up care plan, and that SES had no relationship [28]. A Canadian study involving patients with a range of cancers found that males, those who were married, those who spoke French, and those with less education were more likely to report positive follow-up experiences [29].
There is a lack of recent data regarding survivorship care experiences in Australia and elsewhere, making it difficult to know whether current survivorship care is meeting the needs of cancer survivors. To better understand the care experiences of people diagnosed with cancer in Victoria, Australia, the Victorian Department of Health commissioned a Cancer Patient Experiences Survey (CPES) which was conducted across all Victorian public hospitals in 2019. This study is aimed at interrogating the Victorian CPES dataset to assess follow-up care experiences of Victorian patients and investigating associations between follow-up experiences and selected sociodemographic and clinical characteristics.
Methods
Study design and setting
Analysis of data collected via a cross-sectional survey commissioned by the Victorian Department of Health and was conducted by a contracted survey administrator. This study focuses on responses from participants in follow-up care. Analysis of the data set had institutional ethics approval (HREC/76910/PMCC).
Participants and procedure
People aged ≥ 16 years who received at least some of their cancer care (including surgery, chemotherapy, or radiotherapy) as an inpatient or outpatient in an adult Victorian public hospital in 2018 were eligible for the survey. Cancer care in Australia is delivered in the public hospital (funded by government, no costs to patients) and private hospital (funded by patient either themselves or through private health insurance) systems, with patients choosing the hospital system for each treatment (i.e. surgery, chemotherapy). Therefore, patients eligible for this survey may have had some elements of their care, including follow-up care, in the private system.
Victorian public hospitals delivering cancer care identified eligible participants and provided contact details to the survey administrator, who mailed them the survey, invitation letter, information sheet, and reply-paid envelope. The invitation letter stated that the survey was being conducted by the Victorian Department of Health. English-speaking participants could complete either an electronic or paper version of the survey. People speaking a language other than English (identified from hospital data) completed a professionally translated paper version of the survey in their preferred language.
Variables and data sources
The CPES survey was based on items in the UK’s National Cancer Patient Experience Survey [30], and findings from a literature review, focus groups, and interviews with patients and health professionals, and was pilot tested at multiple health services [31, 32]. The questionnaire was divided into different care episodes, reflecting diagnosis, treatment (i.e. surgery, radiotherapy, chemotherapy), follow-up care, general experiences regarding communication with and between health professionals, care co-ordination, and information provision. Respondents completed sections relevant to their care. Most questions followed a format asking if a specific care element occurred or specific information was provided with responses generally made on a 4-point scale of ‘Yes, definitely’, ‘Yes, I think so’, ‘No, I don’t think so’, or ‘No, definitely not’. Options for not recalling and not applicable were provided. This paper utilises data from seven items that directly assess follow-up care experiences (see Fig. 1, Table 2 for items).Fig. 1. Receipt of information relating to the seven areas of survivorship care (missing responses included in analyses but data not shown, hence total does not add to 100%)
Demographics (see Table 1), cancer type, and location of each treatment (health service name and postcode) included for follow-up care were also assessed. Table 1. Demographic and cancer characteristics of sample and by follow-up care statusCharacteristicTotal^a^Not in follow-upIn follow-upp-valueN = 4998N = 1663N = 3335n%n%n%Gender Male24444987152157347 Female24404971343172252 Missing1392795351 < 0.001Age (in years) < 5053811119741912 50–59753151801157317 60–6914502943426101630 70–791410285253188527 ≥ 8056011262162989 Missing287613291444 < 0.001Socioeconomic disadvantage^b^ Highest disadvantage (40%)15773253832103931 Mid (40%)17713560234116935 Highest advantage (20%)778162321454616 Missing8721729117581170.17Follow-up care treatment centre location^c^ Metropolitan area371874121773250175 Regional centre1050213642268621 Large/medium/small/remote towns230583514840.37Language spoken at home Not English47610149932710 English4522901514913008900.34Aboriginal or Torres Strait Islander Yes361101261 No4962991653993309990.48Self-reported health status Excellent54511155939012 Very good/good31226495757225468 Fair/poor1062214472761518 Missing18041046762 < 0.001Cancer type Colorectal4739141833210 Breast838171721066620 Prostate615122461536911 Haematological984203772360718 Lung/Mesothelioma327714491835 Melanoma/skin22447551494 Gynaecological^d^19844221565 Urological323610662177 Other1016203602265620 < 0.001Year of diagnosis 2015 or earlier639132511538812 201625857851715 2017908182241368521 201827245588053198455 Missing4699221132487 < 0.001Number of treatment^e^ modalities 1275255115169160148 213452734221100330 369414137855717 420743321745 < 0.001Treatment Surgery28575753732232070 < 0.001 Radiotherapy16883434721134140 < 0.001 Chemotherapy22884667741161148 < 0.001 Hormone blocking therapy753151661058718 < 0.001Health care system for follow-up care Public27485527116247774 Private6921479561318Missing1558311313792457 < 0.001^a^Total respondents participating in survey^b^Based on Australian Bureau of Statistics Index of Relative Socioeconomic Advantage and Disadvantage [33]^c^Based on Modified Monash Model location index [34]^d^Gynaecological includes uterus, ovarian, cervical, vulvar, vaginal, endometrial, and fallopian tube^e^Active surveillance/watchful waiting included as a management modality
Data handling and analysis
Analyses were undertaken using STATA (version 17) and IBM SPSS Statistics (version 27). Prior to formal analysis, descriptive statistics identified missing and out-of-range values and items with low response rates.
Following others [25], responses to follow-up care items were recoded into three categories: ‘Yes, definitely’ (2, indicating optimal care), ‘Yes, I think so’ (1), and all other responses coded (0). A composite rating was calculated by summing responses across the seven follow-up care items and calculating the mean to ensure scores remained on the 0–2 scale, with this measure used as an indicator of survivorship care overall. Following others [25, 29], this score was dichotomised to indicate overall optimal survivorship care (mean score ≥ 1.5 indicating the majority of items were scored 2) or not (sub-optimal care). Internal consistency reliability for the measure was good (Cronbach’s alpha: follow-up = 0.87).
Residential postcode was used to assign socioeconomic status to each participant via the Australian Bureau of Statistics’ Index of Relative Socioeconomic Advantage and Disadvantage. This postcode-based indicator provides a score summarising levels of employment, income, education, and other economic and social conditions of an area [33]. Quintile cutoffs are provided, and these were categorised into three groups indicating the 20% least disadvantage, the 40% most disadvantaged, and the 40% with mid-levels of disadvantage. Participants provided the name and location (town, suburb, or postcode) of the health service managing their follow-up care, and this service was assigned to the private or public hospital system and to a metropolitan, regional, rural, or remote location using the Modified Monash (MM) Model, the measure of location used by the Australian Government [34]. The MM Model classifies areas into one of seven categories ranging from metropolitan (1) to very remote (7) based on the Australian Bureau of Statistics’ Australian Statistical Geography Standard framework [35] and population size. Responses to sociodemographic and clinical characteristic items were recoded to discrete variables as shown in Table 1, with missing data categorised into a ‘missing’ group. Aboriginal and/or Torres Strait Islander background was coded yes or no. The number of treatment modalities was counted based on whether respondents had received surgery, radiotherapy, chemotherapy, or hormonal therapy (possible range 1–4). For this study, active surveillance and watchful waiting were included as a possible management strategy.
Descriptive statistics summarised respondent characteristics for the full sample and by follow-up care status. Bivariate chi-square analyses and multivariate logistic regression assessed associations between the sociodemographic and clinical characteristics and the optimal score on each follow-up care item. Logistic regression explored multivariate associations between sociodemographic and clinical characteristics and optimal follow-up experience indicator. All tests were two-sided and given the large sample size, and alpha was set at 0.01, with no adjustment for multiplicities.
Results
Of the 10,662 patients receiving at least some of their cancer care within public hospitals in Victoria in 2018, 4998 (47%) completed the survey and of these 3335 (67%) were in follow-up care.
Participant characteristics
Participant characteristics for the entire sample and by follow-up care status are shown in Table 1. While socioeconomic status, remoteness of follow-up centre, Indigenous status, and language spoken at home did not differ between those in and not in follow-up care, differences were found for all other characteristics and treatment variables. Respondents in follow-up care were more likely to be younger, female, to rate their health as generally good and to have breast cancer.
Experiences of care during follow-up
Figure 1 shows variation in the proportion of respondents indicating they definitely received information across the seven survivorship care items. The highest proportions of respondents indicate they definitely received information related to the follow-up tests needed (71%) and the schedule of tests and checkups (73%). The percentages of respondents reporting optimal experiences on each of these items by sociodemographic and clinical factors are shown in Table 2. Items with the fewest participants reporting optimal experiences were receipt of information about new symptoms needing investigation (44%) and how people feel after treatment (46%). Characteristics consistently associated with receiving optimal care across these items in multivariate analyses (adjusted for all items in Table 2) included being male, reporting to be in excellent health, and having prostate or a haematological cancer. There was some variation in care experiences by socioeconomic status, with those from areas of higher socioeconomic advantage less likely to report optimal experiences relating to receiving a follow-up plan and how to get support if needed. Those diagnosed most recently were less likely to report optimal follow-up experiences (Table 2) especially in relation to receiving a follow-up care plan, information about follow-up tests, how to stay healthy, and what new symptoms need to be monitored for. Health system of follow-up care was not related to care experiences. Table 2. Percentage of respondents reporting optimal experience^a^ for each follow-up care item by sociodemographic and clinical variables (note p-values multivariable^b^ Chi square tests) (n = 3335)NReceive written follow-up care planReceive information about the follow-up tests neededReceive information about how to stay healthyReceive information about what new symptoms to monitor forReceive information about how people feel emotionally after treatmentReceive information about how to get extra support if neededReceive information about how often need tests/check-ups%%%%%%%Total sample All333550716444465073Gender Male157353766847505276 Female172746666142424870 Missing3560837146466077 Multivariate p-value0.012 < 0.001 < 0.0010.011 < 0.001 < 0.0010.019Age group (years) < 5041941635842434666 50–5957351726847455274 60–69101648726645485075 70–7988554756544464976 80 + 29850675846445066 Missing14453696340445169 Multivariate p-value0.0040.0180.060.830.460.500.004Socioeconomic disadvantage^c^ Highest disadvantage (40%)103953736649475475 Mid (40%)116950716443464973 Highest advantage (20%)54648686344494771 Missing58145706240414671 Multivariate p-value0.0010.400.230.0030.0540.0060.41Follow-up care treatment centre location^d^ Metropolitan area250149706344454872 Regional centre68651756848505677 Large/medium/small/remote towns14855726143475376 Multivariate p-value0.800.200.110.170.0460.0300.08Language spoken at home Not English32757706750525070 English300849716444455073 Multivariate p-value0.0010.510.080.0030.0010.220.93Aboriginal or Torres Strait Islander Yes2662736550505873 No330950716444465073 Multivariate p-value0.350.840.820.940.950.690.68Self-reported health status Excellent39059777154575979 Good225450736545465075 Fair or poor61543615839374364 Missing7647635836425167 Multivariate p-value< 0.001< 0.001< 0.001< 0.001< 0.001< 0.001< 0.001Cancer Type Colorectal33250726139374373 Breast66648676943495669 Prostate36960807045555779 Blood60753776853545680 Lung/Mesothelioma18350706745445074 Melanoma14944674840333475 Gyneacological^e^15647625847404976 Urological21744715536323370 Other65645676243434667 Multivariate p-value0.0030.103 < 0.001 < 0.001 < 0.001 < 0.0010.017Year diagnosed 2015 or earlier38854766553535480 201617149736149485379 201768458777147495277 2018184446686241434871 Missing24850676044424667 Multivariate p-value < 0.001 < 0.0010.0050.0030.150.43 < 0.001Number of treatment modalities^f^ 1160152736143424575 2100349716646485273 355746696847525769 417446667039515770 Multivariate p-value0.170.880.180.19 < 0.001 < 0.0010.48Health system for follow-up care^g^ Public247750716544465073 Private61347716346454974 Missing24552716342474973 Multivariate p-value0.450.980.710.490.630.920.78^a^Optimal care indicated by ‘Yes definitely’ response to the item. Percentage rounded to nearest whole number with decimal values ≥ 0.5 rounded up^b^Multivariable analyses included all variables shown in the table and involved logistic regression analyses (see supplementary Table 1 for results from these analyses)^c^Index of Relative Socioeconomic Advantage and Disadvantage [33]^d^Based on Modified Monash Model [34]^e^Gynaecological includes uterus, ovarian, cervical, vulvar, vaginal, endometrial, and fallopian tube^f^Active surveillance/watchful waiting included as a management modality^g^See text for explanation of health systems
Variation in optimal survivorship care
The average score for the combined survivorship care experience measure was 1.21 (SD = 0.67), suggesting follow-up care was on average lower than optimal. Only 27% scored 2 indicating optimal scores on all seven items. Forty percent had scores ≥ 1.5 on this scale forming the optimal follow-up care group. In bivariate analyses, optimal follow-up care was related to gender (p < 0.001), socioeconomic status (p < 0.001), language spoken at home (p < 0.001), self-reported health status (p < 0.001), cancer type (p < 0.001), number of treatment modalities (p < 0.01), and diagnosis year (p < 0.01) (Table 3). These associations generally held in the multivariate analyses. The multivariable analyses suggest that women, respondents from areas of higher socioeconomic advantage, those speaking English at home, those with poor self-reported health, and those diagnosed more recently were less likely to report optimal follow-up care (Table 3). Participants diagnosed with breast, prostate, and haematological cancers were more likely than those with colorectal cancer to report optimal follow-up care. Table 3. Descriptive statistics for the optimal follow-up care^a^ by sociodemographic and clinical characteristics and multivariate logistic regression results (all analyses based on sample included in multivariable regression: n = 3335). Adjusted odds ratio (aOR) (and 95% confidence intervals (CIs)) for demographic, disease, and treatment factors associations with optimal follow-up careN% reporting optimal careBivariate p-valueaOR95% CIsMultivariate p-valueTotal40%GenderMale157345%1Female172737%0.600.50–0.73Missing3543% < 0.0011.250.58–2.67 < 0.001Age group < 5041939%150–5957342%1.070.81–1.3960–69101641%1.050.82–1.3570–7988541%1.060.82–1.3680 + 29836%0.950.68–1.32Missing14440%0.581.290.84–1.980.86Socio-economic disadvantage^b^Highest disadvantage (40%)103945%1Mid (40%)116939%0.750.62–0.90Highest advantage (20%)54639%0.710.56–0.90Missing58136%0.0010.610.48–0.77 < 0.001Follow-up care treatment centre location^c^Metropolitan area250140%1Regional centre68644%1.150.94–1.39Large/medium/small/remote towns14841%0.141.020.71–1.480.38Language spoken at homeNot English32748%1English300840%0.0010.630.49–0.80 < 0.001Aboriginal or Torres Strait IslanderYes2650%1No330940%0.320.820.37–1.830.62Self-reported health statusExcellent39051%1Good225441%0.620.50–0.78Fair or poor61534%0.420.32–0.55Missing7633% < 0.0010.360.20–0.63 < 0.001Cancer typeColorectal33234%1Breast66643%1.751.27–2.41Prostate36947%1.481.06–2.05Blood60750%1.931.42–2.61Lung/Mesothelioma18352%1.641.11–2.42Melanoma14927%0.840.54–1.31Gyneacological^d^15635%1.450.94–2.22Urological21730%0.830.56–1.22Other65636% < 0.0011.100.82–1.47 < 0.001Year diagnosed2015 or earlier38850%1201617146%0.860.59–1.24201768445%0.850.65–1.112018184437%0.620.48–0.79Missing24838% < 0.010.690.49–0.98 < 0.001Number of treatment modalities^e^1160137%12100343%1.281.07–1.52355745%1.441.14–1.82417443% < 0.011.330.90–1.960.01Health system for follow-up care^f^Public247741%1Private61339%0.930.77–1.13Missing24540%0.651.020.76–1.360.76^a^Optimal follow-up care determined from mean of seven follow-up care items (scored 0–2) with scores ≥ 1.5 indicating optimal care^b^Based on Australian Bureau of Statistics Index of Relative Socioeconomic Advantage and Disadvantage [33]^c^Based on Modified Monash Model location index [34]^d^Gynaecological includes uterus, ovarian, cervical, vulvar, vaginal, endometrial, and fallopian tube^e^Active surveillance/watchful waiting included as a management modality^f^See text for explanation of health system
Discussion
Data from a statewide survey of care experiences for people attending a public hospital for at least part of their cancer care provided a unique opportunity to explore survivorship care experiences for a large cohort of patients with multiple cancer types, treated with a variety of treatment modalities across a range of health settings. Survivorship care experiences varied and while in general around 50% of people reported receiving information on each of the follow-up care items, when considering the items in combination, only around 40% were assessed as receiving optimal survivorship care. Those less likely to report optimal survivorship care were female, from areas with higher socioeconomic advantage, reporting their health to be good or fair/poor, not diagnosed with breast, prostate, lung or a haematological cancer, and diagnosed more recently.
With the number of cancer survivors increasing worldwide, there is growing recognition of the importance of delivering follow-up or survivorship care that meets the medical and psychosocial needs of survivors. To this end, a number of survivorship care frameworks or recommendations have now been developed to assist health services to develop their survivorship care programmes and ensure that the dimensions of care that health professionals and survivors consider important are recognised [5, 6, 9, 11, 36]. Work assessing survivors’ experiences of follow-up care can help to identify the extent to which these frameworks are informing survivorship care. Ours is one of the few studies to have examined this issue for an Australian population of cancer survivors. Although our findings that Australian survivors were less likely to receive information regarding emotional responses to cancer and support services than information about follow-up tests is similar to results found in the US literature [26, 37, 38], the proportions reporting receiving emotional and support information were higher in our study compared to the US. While this may reflect differences in study questions, it might also reflect different practices. Although at the time of our study there were no Australian specific frameworks for survivorship care, Australia had in place a set of recommendations for optimal cancer care that provided recommendations for follow-up care that extended beyond a schedule for follow-up tests and appointments [39]. Additionally, between 2011 and 2019, the Victorian Department of Health delivered a grants programme that aimed to improve survivorship care. Since then, the Department has funded other statewide improvement work, partly with the goal to increase awareness of the need for optimal survivorship care. This activity may have helped to increase delivery of supportive care information as part of routine survivorship care in Victoria. Nonetheless, with only 40% of participants in our study reporting optimal survivorship care overall, and with some groups experiencing better care than others, the current study suggests the structures and processes in place within the health care system at the time of the survey may not be working for all Victorian patients. The survey was repeated in 2023, and we plan to analyse this dataset to assess change in the delivery of survivorship care over time.
Others have found that SES, cancer type, age, and gender influence experience of care [25, 27] although the patterns of association in these studies differ from ours. In our study using an area-based indicator of socioeconomic advantage/disadvantage, we found that those with greater disadvantage were more likely to report optimal follow-up care. Ways of assessing SES may be important in determining whether it is associated with care experiences. For instance, a study from the US involving 1320 cancer survivors used multiple indicators to determine SES including health insurance status (public, private, or uninsured), family income, and education and found that lower SES groups were less likely to report having follow-up care discussions with their health care team [27]. However, a smaller study focusing on rural cancer survivors in the US found an inverse association with quality patient provider communication and education levels and income level [40]. An Australian study that also used an area level indicator of SES similar to the one used in our study, found no association between SES and patient communication, involvement, and provision of supportive services during cancer care [41]. More work is needed to explore the association between SES and care experiences. While we speculate that the pattern of associations we found may reflect differences in expectations or priorities, research is needed to identify the factors underlying our results.
Although others have found that people in rural and remote areas experience significant disparities in access to cancer treatment [42], our study did not find a significant association between follow-up care experiences and location of treatment service. Another Australian study also found no difference in the experiences of information provision and patient involvement during cancer care for people living in metropolitan and rural/remote areas [41]. These are positive findings that suggest survivors experience similar quality of follow-up care in metropolitan and regional/rural health services.
Our study found that males were more likely to report optimal survivorship experiences than females. While some other studies have also found that females are more likely to report poor care experiences [29, 43], others have not [27, 40]. A large population-based Australian study looking at communication throughout cancer care and provision of information and services found no difference in the experiences of males and females [41]. There are limited studies to explain the differences in care experiences by gender. One study found females reported higher need and regard for psychosocial support than men, which may explain differences [44]. This study suggested that men are more likely to receive support from sources external to the health system and hence may rate their experiences within the health system as more positive [44]. Other work has noted that patients with breast, melanoma, haematological, and testicular cancers are less likely to make negative comments about their care, whereas patients with small intestine/rarer lower gastrointestinal, hepatobiliary, and renal cancers were most likely to report negative experiences [43]. Our results align with this pattern for breast and haematological cancers but not melanoma. While more work is needed to confirm our findings for gender, if found to be true in other Australian populations, the factors influencing poorer survivorship care experiences for women with cancers other than breast need to be investigated. Our findings relating to differences in survivorship care experiences for different cancer types also suggest more work is needed to understand reasons for this.
Those reporting to have better health were more likely to report optimal survivorship care. While our results need to be confirmed, reasons for these differences need to be explored. Our results may reflect that those with better health have simpler health needs and are more satisfied with the information they receive. Those with poor self-reported health were less likely to report optimal care across all seven follow-up care items. We do not know if the poorer state of health is due to their cancer or to other health conditions. If the latter, our findings may reflect poor integration of care across different health conditions. If the former, it may reflect the greater needs of this group of survivors. While work to understand these differences is needed, our findings suggest that health services could direct further intervention efforts to those who rate their own health as poor.
Strengths and limitations
Principal strengths of this study are its large sample size and inclusion of participants from a range of health services and with a range of cancers. However, a number of limitations need to be noted. While many people in Australia have their cancer treatment in both the public and private systems, this study identified patients for inclusion through public hospitals only. Therefore, people who received all their cancer care in the private system were not included. Socioeconomic status was inferred by postcode, which may not be as reliable as a person-level indicators such as income, education, or occupation status. While we included treatment and cancer type in our multivariable models, we did not have information on disease stage, health service utilisation, or treatment outcomes and hence could not control for their potential impact. As data were self-reported, bias in recall due to the time since people entered follow-up may influence findings.
Although the survey was available in a variety of languages, representation of people from culturally and linguistically diverse backgrounds, as indicated by language spoken at home, was relatively low. Further research to enhance inclusivity of these populations is required. There was a relatively low response rate of 47%, which places the results at risk of selection bias. However, the response rate is comparable to other surveys of patient experiences conducted in Australia [45, 46]. Our study also had a low number of responses from Aboriginal and Torres Strait Islander peoples, which precluded undertaking analysis of this data. Strategies to engage and support Aboriginal and Torres Strait Islander peoples to participate in studies to assess their care experiences, including using culturally appropriate questions, are needed [47, 48].
Conclusion
Large numbers of Australian cancer survivors report sub-optimal survivorship care. Further work is needed to understand the factors influencing survivorship care experiences for different groups of patients, particularly for women with cancers other than breast and for those with poor self-reported health. Ongoing monitoring of patients’ care experiences during and post-treatment can provide important information relating to the quality of care and gaps in services. Our findings suggest that further work is needed to increase the provision of information to survivors about new symptoms to monitor for, common emotional responses after treatment, and ways to access support when needed.
Supplementary Information
Below is the link to the electronic supplementary material.Supplementary file1 (XLSX 28 KB)
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Victorian Cancer Registry (2021) Cancer in Victoria 2020. Melbourne, Victoria. https://www.cancervic.org.au/downloads/cec/cancer-in-vic/Cancer-in-Victoria-statistics-and-trends-2020.pdf. Accessed Sept 2024
- 2Lisy K, Ly L, Kelly H et al (2021) How do we define and measure optimal care for cancer survivors? An online modified reactive Delphi study. Cancers (Basel) 13(10):229910.3390/cancers 13102299 PMC 815085934064957 · doi ↗ · pubmed ↗
- 3Rechis R, Beckjord EB, Arvey S, Reynolds K, Mc Goldrick D (2011) The essential elements of survivorship care: a livestrong brief. https://www.iccp-portal.org/system/files/resources/Essential Elements Brief.pdf. Accessed Aug 2024
- 4Mollica MA, Mc Whirter G, Tonorezos E et al (2024) Developing national cancer survivorship standards to inform quality of care in the United States using a consensus approach. J Cancer Survivorship 10.1007/s 11764-024-01602-6PMC 1132467438739299 · doi ↗ · pubmed ↗
- 5NHS England. National Cancer Experience Survey 2024 [cited 2024 22/8/2024]; web site for National Cancer Patient Experience survey UK]. Available from: https://www.ncpes.co.uk/about-the-survey/. Accessed Feb 2024
- 6State of Victoria Department of Health and Human Services (2016) Understanding care experiences of people with cancer: findings from pilot study 2. Technical paper. Victorian Government, Melbourne. https://www.health.vic.gov.au/health-strategies/victorian-cancer-patient-experience-survey-tool-project. Accessed Sept 2023
- 7State of Victoria Department of Health and Human Services (2016) Victorian cancer patients’ care experiences in 2015. Developing a survey to measure expereinces across the cancer treatment pathway. Victorian Government, Melbourne. https://www.health.vic.gov.au/health-strategies/victorian-cancer-patient-experience-survey-tool-project. Accessed Sept 2023
- 8Statistics A Bo. Socio-Economic Indexes for Areas (SEIFA): technical paper 2023. Technical paper available at https://www.abs.gov.au/statistics/detailed-methodology-information/concepts-sources-methods/socio-economic-indexes-areas-seifa-technical-paper/2021. Accessed Jul 2024