Salmonella Endocarditis: Rare Bacteremia Causing Mural Infective Endocarditis
Seth Krueger, Michael Carcella, Caroline Dillon, Darrell McBride

TL;DR
A rare case of Salmonella endocarditis in a patient with heart devices highlights the need for cardiac imaging in atypical bacteremia.
Contribution
This case demonstrates that cardiac imaging may be beneficial in patients with cardiac devices and atypical bacteremia.
Findings
Salmonella bacteremia led to right atrial mural endocarditis in a patient with implantable devices.
Removal of infected devices in the operating room prevented embolization risks.
Eight-month follow-up showed no recurrence after 6 weeks of antibiotic therapy.
Abstract
Current guidelines do not recommend routine cardiac imaging in patients with gram-negative bacteremia, as gram-negative infective endocarditis is rare. Nongastrointestinal Salmonella infections causing endocarditis are even more uncommon, especially in the developed world. We present the case of a 60-year-old female with Salmonella bacteremia, ultimately found to have a right atrial mural endocarditis involving an implantable cardioverter–defibrillator and an indwelling venous catheter. The vegetation and indwelling devices were removed from the operating room due to the high concern of embolization if performed percutaneously, and she completed 6 weeks of antibiotic therapy. Both indwelling devices were later replaced once treatment was completed, and there was no evidence of recurrence at the 8-month follow-up. This case proves that in those with cardiac implantable electronic devices…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
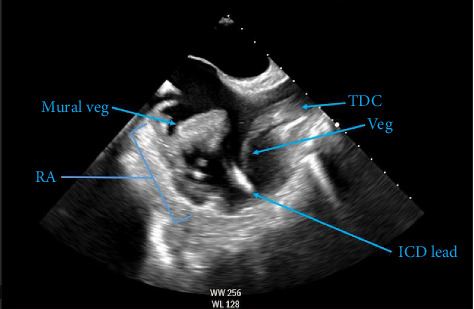 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsInfective Endocarditis Diagnosis and Management · Antimicrobial Resistance in Staphylococcus · Salmonella and Campylobacter epidemiology
1. Introduction
Infective endocarditis (IE) is most commonly caused by gram-positive bacteria, such as Staphylococcus, Streptococcus, and Enterococcus species, and usually occurs in the immunocompromised, intravenous drug users, patients receiving hemodialysis, and those with structural cardiac abnormalities [1]. Rarely, IE can be caused by gram-negative bacteria, such as the Salmonella species. This gram-negative endocarditis is uncommon in the developed world; patients are often immunocompromised and the mortality rate is high [2]. Even more rare is mural IE (MIE), which is only described in case reports and a small number of retrospective reviews [3, 4]. In this report, we describe a patient who presented with septic shock due to Salmonella bacteremia and was ultimately diagnosed with Salmonella MIE, which involved her implantable cardioverter–defibrillator (ICD) and dialysis catheter. To our knowledge, this is the first case of its kind to be reported in the literature.
2. Case Presentation
The patient was a 60-year-old Caucasian female with numerous medical comorbidities, most notable for end-stage renal disease on intermittent hemodialysis via tunneled dialysis catheter within the right internal jugular vein, and heart failure with reduced ejection fraction with in situ biventricular pacemaker/ICD. Other comorbidities included coronary artery disease, Type 2 diabetes mellitus, and chronic wounds of the right lower extremity. She presented to the emergency department with severe pain, swelling, and redness in the right lower extremity in the location of a chronic wound. She denied recent diarrheal illness or sick contacts. She was admitted to the hospital and treated with broad-spectrum antibiotics. Early in the admission, she developed signs of septic shock, prompting escalation to intensive care with vasopressor support. Preliminary culture data demonstrated growth of Salmonella species in all four blood culture bottles, with resistance to ampicillin and ceftriaxone, but susceptibility to cefepime, ciprofloxacin, and carbapenems. Computed tomographic (CT) imaging of the right lower extremity was normal and subsequent CT of the cervical, thoracic, and lumbar spine was also negative for osteomyelitis and discitis. An initial transthoracic echocardiogram (TTE) was performed and was unremarkable for intracardiac or valvular vegetations. Follow-up transesophageal echocardiography (TEE) demonstrated a 3.0 × 2.2 cm mass on the right lateral wall of the right atrium as well as multiple, scattered, mobile echo densities on the tip of the neighboring hemodialysis catheter (Figure 1). These findings were consistent with underlying endocarditis, likely due to Salmonella.
After receiving antibiotics, the patient was hemodynamically stable, and a multidisciplinary discussion was held between the patient and the primary medical team, electrophysiology, nephrology, and cardiovascular surgery. Options for management included definitive treatment with removal of the mass and contaminated hardware or long-term antibiotic suppression with frequent surveillance imaging. After a discussion of the risks and benefits, the patient underwent an unsuccessful attempt at transcatheter aspiration of the right atrial vegetation. She subsequently underwent an open cardiothoracic procedure for the removal of the mass. The ICD and dialysis catheter were also removed during surgery due to concern for increased risk of embolization if removed percutaneously. Intraoperatively, the large vegetation was found to involve the right atrial wall. Vegetations were also noted on the tip of the hemodialysis catheter, as well as on the implanted pacemaker leads. The tricuspid valve was not involved. No major complications occurred intraoperatively or in the postoperative course. Culture of the surgical specimens revealed Salmonella species, confirming the source of bacteremia.
Postoperatively, the patient was managed definitively with cefepime and completed 6 weeks of treatment. She was counseled on the risks of hardware reinfection versus the benefit of maintaining reliable hemodialysis access and ultimately chose for a replacement tunneled dialysis catheter in the right internal jugular vein. No recurrence was present on follow-up echocardiography at four and 8 months.
3. Discussion
Salmonella species are often associated with diarrhea [5]. However, in certain immunocompromised hosts, cardiac infection may occur [4, 6]. We have described a rare case of large MIE.
The incidence of isolated mural endocarditis is unknown but is regarded as less common than the valvular presentation and, in one study, represented only 0.07% of IE cases [4]. A retrospective analysis published in 2022 also found that vegetation in MIE is more likely to be large, defined as 10 mm or greater [3]. Patients with indwelling devices, such as central venous catheters or hemodialysis lines, have a higher incidence of mural involvement [4, 7, 8]. Gutierrez et al. hypothesized that the direct mechanical insult from a catheter tip or flow from the catheter jet predisposes local cardiac tissue to Salmonella colonization [4]. Our case is consistent with this hypothesis, as the catheter tip was intimately involved with the mural vegetation.
In addition to MIE, our patient also had a cardiovascular implanted electronic device infection (CIED). In the setting of CIED, extraction of the device is imperative and, when left in situ, there is a 7-fold increase in mortality within the first 30 days. With the proper extraction and antibiotic treatment, the risk of recurrence is 1% compared to 50%–100% when treated with antibiotics alone [9]. If the patient is considered too high risk to undergo removal, long-term palliative antibiotics can be considered, but this should be used as a last resort [10].
Since gram-negative endocarditis is rare, current guidelines do not recommend routine cardiac imaging in patients with gram-negative bacteremia, even in the setting of cardiac implantable devices [11]. We propose that cardiac imaging should be strongly considered when atypical bacteremia is found in patients who are receiving hemodialysis, are immunocompromised, or have indwelling devices. A thorough evaluation of endocarditis in these patients is imperative, as timely diagnosis is crucial in mitigating serious complications.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Nappi F. Avtaar Singh S. S. Host-Bacterium Interaction Mechanisms in Staphylococcus aureus Endocarditis: A Systematic Review International Journal of Molecular Sciences 20232413 p. 1106810.3390/ijms 241311068 PMC 1034175437446247 · doi ↗ · pubmed ↗
- 2Cheng W. L. Li C. W. Li M. C. Lee N. Y. Lee C. C. Ko W. C. Salmonella Infective Endocarditis Journal of Microbiology, Immunology, and Infection 201649331332010.1016/j.jmii.2015.02.6592-s 2.0-8492712721925882489 · doi ↗ · pubmed ↗
- 3Rajesh G. N. Vellani H. Vadasseril Jose J. Mohanan S. Sajeev C. G. Clinical Profile and One-Year Outcomes of Patients With Mural Infective Endocarditis: A Tertiary Care Centre Study Based on Data From a Seven-Year Registry Indian Heart Journal 202274316316910.1016/j.ihj.2022.05.00335550126 PMC 9243601 · doi ↗ · pubmed ↗
- 4Gutiérrez-Villanueva A. Muñoz P. Delgado-Montero A. Infectious Disease and Therapy 20211042749276410.1007/s 40121-021-00490-y PMC 857295034312819 · doi ↗ · pubmed ↗
- 5Cdc Salmonella-Questions and Answers
- 6Hall R. L. Partridge R. Venkatraman N. Wiselka M. Invasive Non-Typhoidal Salmonella Infection With Multifocal Seeding in an Immunocompetent Host: An Emerging Disease in the Developed World BMJ Case Reports 20132013 p. bcr 201200823010.1136/bcr-2012-0082302-s 2.0-84874668194 PMC 360432823370956 · doi ↗ · pubmed ↗
- 7López-Ciudad V. Castro-Orjales M. J. León C. Successful Treatment of Candida Parapsilosis Mural Endocarditis With Combined Caspofungin and Voriconazole BMC Infectious Diseases 200661 p. 7310.1186/1471-2334-6-732-s 2.0-33646589312 PMC 145834816608509 · doi ↗ · pubmed ↗
- 8Huang D. B. Du Pont H. L. Problem Pathogens: Extra-intestinal Complications of Salmonella enterica Serotype Typhi Infection The Lancet Infectious Diseases 20055634134810.1016/s 1473-3099(05)70138-92-s 2.0-2034437667715919620 · doi ↗ · pubmed ↗