Interventions for recurrent embryo implantation failure: An umbrella review
Abdulla Almohammadi, Fadi Choucair, Khalid S. Khan, Aurora Bueno‐Cavanillas, Naomi Cano‐Ibáñez

TL;DR
This umbrella review evaluates the effectiveness of various interventions for recurrent embryo implantation failure, finding some immunomodulatory treatments may help improve pregnancy outcomes.
Contribution
The study provides a comprehensive synthesis of evidence from multiple systematic reviews to assess interventions for recurrent implantation failure.
Findings
Granulocyte colony-stimulating factor (G-CSF) showed improvement in clinical pregnancy rates in 69.2% of meta-analyses.
Intralipid infusion improved live birth rates in 75% of meta-analyses.
Immunomodulatory treatments like PBMC and PRP showed moderate to high strength evidence for improving pregnancy outcomes.
Abstract
Recurrent implantation failure (RIF) has a multifactorial etiology. An umbrella review was undertaken to evaluate the multiple proposed interventions. To summarize and assess the strength of evidence of interventions for RIF from published systematic reviews (SR) of randomized clinical trials (RCTs). After prospective registration (PROSPERO CRD42023414255), a systematic search was conducted in the Cochrane Library, Scopus and Medline from inception until March 2024. SRs of RCTs, with or without meta‐analyses (MA), were included if they reported clinical pregnancy rates (CPR) or live birth rates (LBR). The methodological quality of the included SRs was appraised independently in duplicate using the AMSTAR 2 tool. For each intervention, the MAs of RCTs with statistically significant improvements were counted as a percentage of the total assessing the strength of evidence using the…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
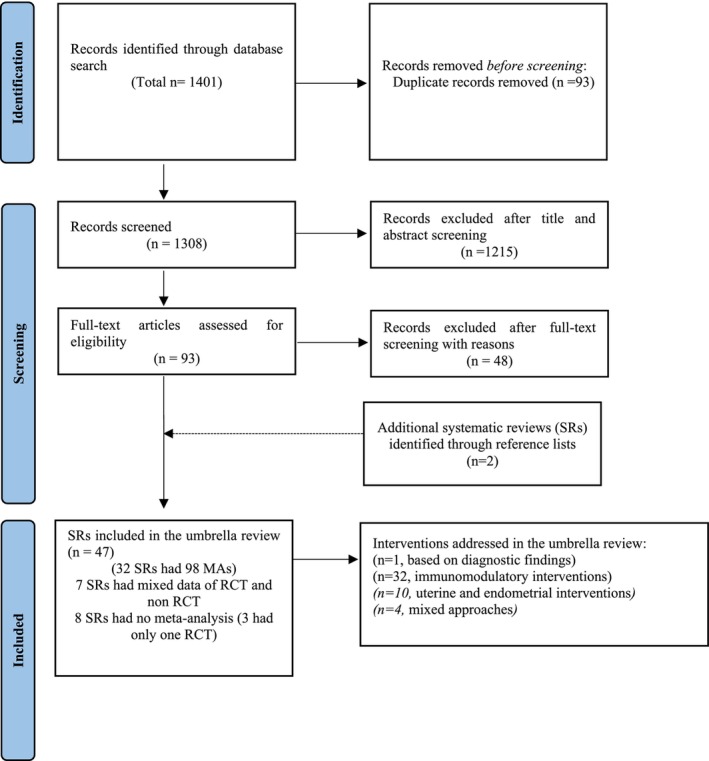 FIGURE 1
FIGURE 1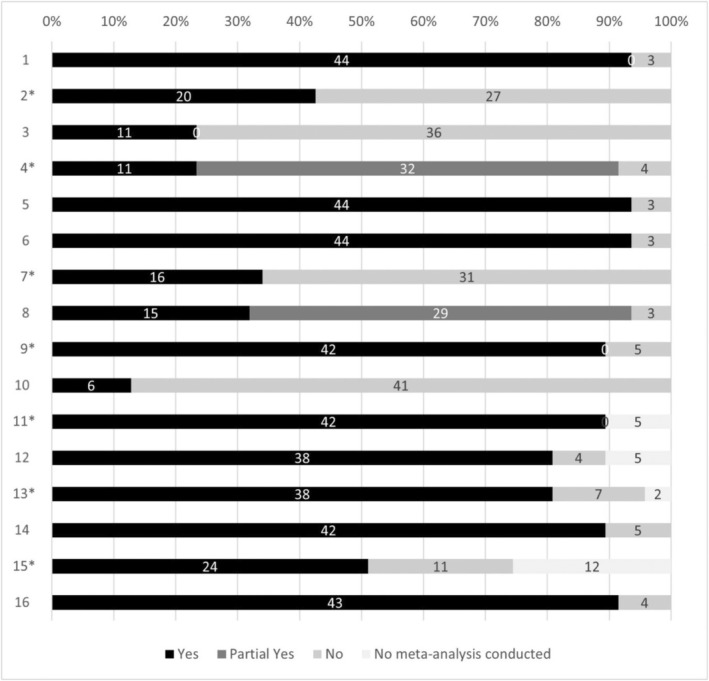 FIGURE 2
FIGURE 2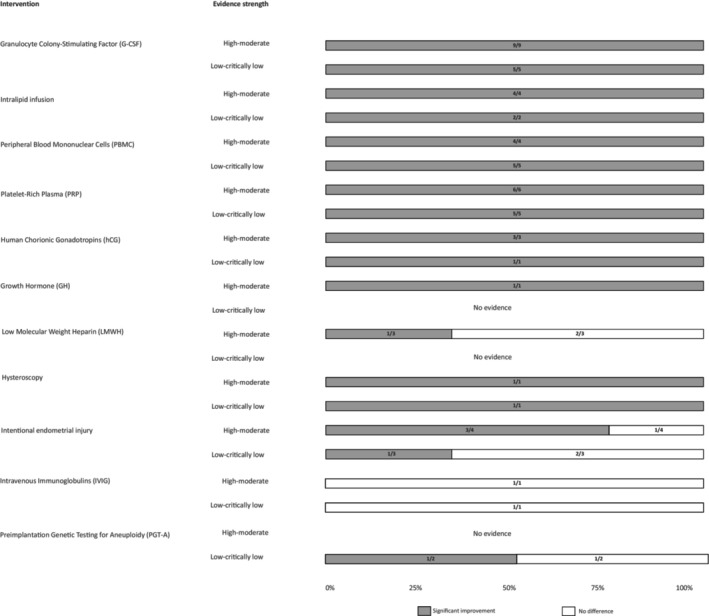 FIGURE 3
FIGURE 3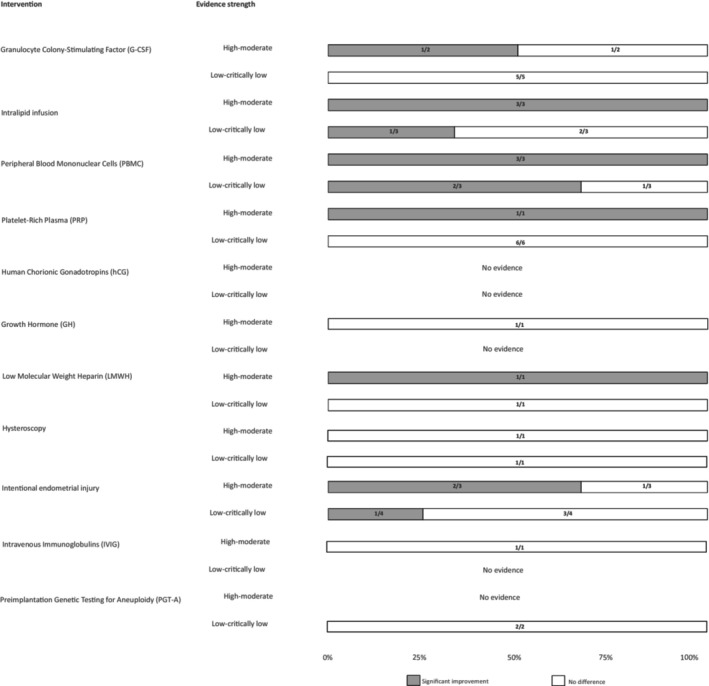 FIGURE 4
FIGURE 4| Overlapping |
| CCA | Classification |
|---|---|---|---|
| Immunomodulatory interventions | |||
| Reviews of RCTs for intralipid effects on CPR in RIF patients | 6 | 52% | Very high |
| Reviews of RCTs for intralipid effects on LBR in RIF patients | 6 | 52% | Very high |
| Reviews of RCTs for PRP effects on CPR in RIF patients | 6 | 38.30% | Very high |
| Reviews of RCTs for PRP effects on LBR in RIF patients | 6 | 30% | Very high |
| Reviews of RCTs for PBMC effects on CPR in RIF patients | 5 | 33.3% | Very high |
| Reviews of RCTs for PBMC effects on LBR in RIF patients | 5 | 0% | Low |
| Reviews of RCTs for G‐CSF effects on CPR in RIF patients | 8 | 33.3% | Very high |
| Reviews of RCTs for G‐CSF effects on LBR in RIF patients | 8 | 0% | Low |
| Reviews of RCTs for IVIG effects on CPR in RIF patients | 2 | 100% | Very high |
| Reviews of RCTs for IVIG effects on LBR in RIF patients | 2 | 0% | Low |
| Uterine and endometrial interventions | |||
| Reviews of RCTs for hysteroscopy effects on CPR in RIF patients | 2 | 0% | Low |
| Reviews of RCTs for hysteroscopy effects on LBR in RIF patients | 2 | 33.3% | Very high |
| Laboratory interventions | |||
| Reviews of RCTs for PGT‐A effect on CPR in RIF patients | 2 | 100% | Very high |
| Reviews of RCTs for PGT‐A effect on LBR in RIF patients | 2 | 100% | Very high |
| Study ID | Intervention | Comparison (No. of RCTs) | Total no. RCTs | No. of patients with CP/total no. | Summary estimate (95% CI) reported for RCT data in the included reviews | GRADE assessment | Reasons for downgrading | AMSTAR‐2 rating |
|---|---|---|---|---|---|---|---|---|
| Immunomodulatory interventions | ||||||||
| G‐CSF | ||||||||
| Kamath et al. 2020 | G‐CSF mixed routes | Placebo (2) or no intervention (4) or mixed (1) | 7 | 150/643 | RR, 2.11 (1.56–2.85) | Low | Serious ROB, strongly suspected publication bias | Low |
| Kamath et al. 2017 | G‐CSF sub‐cutaneous | Placebo (2) | 2 | 39/139 | RR, 2.51 (1.36–4.63) | High | NA | Low |
| Zhang et al. 2018 | G‐CSF mixed routes | Placebo (3) or no intervention (3) or mixed (2) | 8 | NR/NR | RR, 2.07 (1.64–2.61) | Moderate | Serious ROB | Low |
| Jiang et al. 2020 | G‐CSF mixed routes | Placebo (4) or no intervention (5) or mixed (2) | 11 | NR/1035 | RR, 1.91 (1.56–2.34) | Moderate | Serious ROB | Critically Low |
| Wang et al. 2021 | G‐CSF mixed routes | Placebo (3) or no intervention (2) or mixed (1) | 6 | NR/NR | OR, 2.03 (1.35–3.05) | Low | Serious inconsistency, serious indirectness | Critically Low |
| Busnelli et al. 2021 | G‐CSF sub‐cutaneous | Placebo (2) or no intervention (2) | 4 | 99/333 | RR, 2.29 (1.58–3.31) | Moderate | Serious ROB | Low |
| Busnelli et al.2021 | G‐CSF intrauterine | Placebo (1) or mixed (1) | 2 | 65/257 | RR, 1.53 (1.00–2.33) | Moderate | Serious ROB | Low |
| Hou et al. 2021 | G‐CSF mixed routes | Placebo (4) or no intervention (4) or mixed (1) | 9 | NR/986 | RR, 1.55 (1.3–1.85) | High | NA | Moderate |
| Liu et al. 2022 | G‐CSF intrauterine | Placebo (3) or no intervention (1) | 4 | NR/411 | OR, 3.81 (2.53–5.72) | Moderate | Serious inconsistency | Critically Low |
| Jin et al.2022 | G‐CSF mixed routes | Placebo (3) or no intervention (2) | 5 | NR/547 | OR, 1.93 (1.37–2.72) | Low | Serious inconsistency, very serious indirectness | Critically Low |
| Liu et al. 2022 | G‐CSF sub‐cutaneous | Placebo (2) | 2 | NR/164 | OR, 6.69 (3.45–12.97) | Moderate | Serious imprecision | Critically Low |
| Lu et al. 2023 | G‐CSF mixed routes | Placebo (9) or no intervention (5) | 14 | 419/1387 | RR, 1.93 (1.63–2.29) | Moderate | Serious ROB | High |
| Kong et al. 2023 | G‐CSF | Placebo (4) or no intervention (2) | 6 | NR/923 | OR, 0.63 (0.44–0.89) | Low | Serious inconsistency, serious indirectness | Low |
| He et al. 2023 | G‐CSF | Placebo (11) or no intervention (3) | 14 | NR/1291 | OR, 1.94 (1.49–2.55) | Low | Serious ROB, serious inconsistency | Low |
| GH | ||||||||
| Vera‐Montoya et al. 2023 | Growth hormone | No intervention (2) | 2 | 37/112 | OR, 4.97 (2.05–12.05) | High | NA | High |
| IVIG | ||||||||
| Achilli et al. 2018 | IVIG | Placebo (2) | 2 | 22/90 | OR, 1.09 (0.32–3.68) | Moderate | Serious imprecision | Critically low |
| Wang et al. 2021 | IVIG | Placebo (2) | 2 | NR/100 | OR, 1.07 (0.38–2.98) | Low | Serious inconsistency, serious indirectness, serious imprecision | Critically low |
| hCG | ||||||||
| Xie et al. 2019 | hCG | No intervention (3) | 3 | NR/417 | RR, 1.33 (1.03–1.73) | High | NA | Critically Low |
| Jin et al. 2022 | hCG | No intervention (2) | 2 | NR/255 | OR, 1.8 (1.18–2.72) | Moderate | Serious inconsistency | Critically Low |
| Kong et al. 2023 | hCG | Placebo (3) or no intervention (4) | 4 | NR/668 | OR, 0.62 (0.45–0.87) | Low | Serious inconsistency, Serious indirectness | Low |
| He et al. 2023 | hCG | No intervention (4) | 4 | NR/858 | OR, 1.61 (1.15–2.29) | Moderate | Serious inconsistency | Low |
| Intralipid infusion | ||||||||
| Zhou et al. 2020 | Intralipid infusion | Placebo (2) or no intervention (2) | 4 | 153/544 | RR, 1.74 (1.27–2.4) | Moderate | Serious ROB | Low |
| Wang et al. 2021 | Intralipid infusion | Placebo (1) or no intervention (1) | 2 | NR/244 | OR, 1.98 (1.02–3.64) | Low | Serious inconsistency, serious indirectness | Critically Low |
| Han et al. 2021 | Intralipid infusion | Placebo (3) or no intervention (2) | 5 | 291/840 | RR, 4.48 (1.23–1.79) | High | NA | Low |
| Rimmer et al. 2021 | Intralipid infusion | Placebo (3) or no intervention (2) | 5 | 50/203 | RR, 1.55 (1.16–2.06) | High | NA | Critically low |
| Kumar et al. 2021 | Intralipid infusion | Placebo (2) or no intervention (3) or mixed (1) | 6 | 213/560 | OR, 1.51 (1.06–2.13) | Moderate | Very serious ROB | Critically Low |
| He et al. 2023 | Intralipid infusion | No intervention (2) | 2 | NR/345 | OR, 2.18 (1.2–3.94) | Low | Serious ROB, serious inconsistency | Low |
| LMWH | ||||||||
| Liu et al. 2022 | LMWH | No intervention (2) | 2 | NR/357 | OR, 2.94 (2.01–4.31) | Moderate | Serious ROB | Critically Low |
| Busnelli et al. 2021 | LMWH | No intervention (2) | 2 | 49/218 | RR, 1.39 (0.87–2.23) | Moderate | Very serious ROB | Low |
| He et al. 2023 | LMWH | No intervention (1) | 4 | NR/634 | OR, 1.2 (0.83–1.72) | Moderate | Serious inconsistency | Low |
| PBMC | ||||||||
| Wu et al. 2019 | PBMC | No intervention (3) | 3 | 105/316 | OR, 2.45 (1.53–3.91) | High | NA | Critically Low |
| Maleki‐Hajiagha et al. 2019 | PBMC | No intervention (2) | 2 | 76/225 | RR, 2.32 (1.57–3.44) | Low | Very serious ROB | Critically Low |
| Pourmoghadam et al. 2020 | PBMC | No intervention (2) | 2 | 76/225 | OR, 3.57 (1.99–6.4) | High | NA | Moderate |
| Wanget al. 2021 | PBMC | No intervention (5) | 5 | NR/639 | OR, 2.63 (1.71–4.06) | Low | Serious inconsistency, serious indirectness | Critically Low |
| Busnelli et al. 2021 | PBMC | No intervention (3) | 3 | 114/363 | RR, 2.18 (1.58–3) | Low | Very serious ROB | Low |
| Liu et al. 2022 | PBMC | No intervention (4) | 4 | NR/602 | OR, 6.08 (4.37–8.45) | Low | Very serious ROB | Critically Low |
| Jin et al. 2022 | PBMC | No intervention (3) | 3 | NR/366 | OR, 2.79 (1.75–4.45) | Moderate | Serious inconsistency | Critically Low |
| Kong et al. 2023 | PBMC | No intervention (4) | 4 | NR/450 | OR, 0.42 (0.26–0.69) | Low | Serious ROB, Serious inconsistency, Serious indirectness | Low |
| He et al. 2023 | PBMC | No intervention (6) | 6 | NR/605 | OR 3.17 (2.08–4.87) | Moderate | Serious inconsistency | Low |
| PRP | ||||||||
| Busnelli et al. 2021 | PRP | No intervention (2) | 2 | 69/195 | RR, 2.45 (1.55–3.86) | Low | Very serious ROB | Low |
| Wang et al. 2021 | PRP | Placebo (3) | 3 | NR/245 | OR, 2.55 (1.36–4.79) | Low | Serious inconsistency, serious indirectness | Critically Low |
| Liu et al. 2022 | PRP | Placebo (3) or no intervention (2) | 5 | 222/718 | OR, 3.66 (2.58–5.19) | High | Serious ROS | Critically Low |
| Liu et al. 2022 | PRP | Placebo (1) or no intervention (1) | 2 | NR/195 | OR, 6.73 (3.68–12.31) | High | Serious imprecision | Critically Low |
| Li et al. 2022 | PRP | Placebo (2) or no intervention (4) | 6 | 383/1056 | OR, 2.98 (2.29–3.88) | High | NA | Low |
| Hu et al. 2023 | PRP | Placebo (2) or no intervention (2) | 4 | 238/678 | RR, 2.46 (1.93–3.12) | Low | Very serious ROB | Critically Low |
| Jin et al. 2022 | PRP | Placebo (2) or no intervention (2) | 4 | NR/755 | OR, 3.78 (2.72–5.25) | Moderate | Serious inconsistency | Critically Low |
| Maged et al. 2023 | PRP | Placebo (1) or no intervention (5) | 6 | 148/501 | OR, 1.95 (1.1–3.46) | Moderate | Serious ROB | Low |
| Anitua et al. 2023 | PRP | Placebo (3) or no intervention (4) | 7 | 284/893 | RR, 2.18 (1.76–2.7) | High | NA | High |
| Kong et al. 2023 | PRP | Placebo (2) or no intervention (5) | 7 | NR/958 | OR, 0.41 (0.26–0.66) | Low | Serious ROB, Serious inconsistency, Serious indirectness | Low |
| He et al. 2023 | PRP | Placebo (3) or no intervention (2) | 5 | NR/758 | OR 3.22 (2.13–4.78) | Low | Serious ROB, serious inconsistency | Low |
| Uterine and endometrial interventions | ||||||||
| Hysteroscopy | ||||||||
| Mao et al. 2019 | Hysteroscopy | No intervention (3) | 3 | NR/1581 | OR, 1.5 (1.06–2.12) | Moderate | Serious inconsistency | Critically Low |
| He et al. 2023 | Hysteroscopy | No intervention (4) | 4 | NR/1901 | OR, 1.76 (1.34–2.39) | Low | Very serious ROB, serious inconsistency | Low |
| Intentional endometrial injury | ||||||||
| Potdar et al. 2012 | Intentional endometrial injury | No intervention (4) | 4 | 275/983 | RR, 1.71 (1.4–2.09) | High | NA | Low |
| Vitagliano et al. 2018 | Intentional endometrial injury | Placebo (1) or no intervention (7) | 8 | 206/817 | RR, 1.57 (1.22–2.03) | High | NA | Moderate |
| Sar‐Shalom Nahshon et al. 2019 | Intentional endometrial injury | No intervention (5) | 5 | 136/522 | RR, 1.53 (0.93–2.51) | Low | Serious ROB, serious inconsistency | Low |
| Busnelli et al. 2021 | Intentional endometrial injury | No intervention (3) | 3 | 100/286 | RR, 1.43 (0.79–2.61) | Moderate | Serious inconsistency | Low |
| Jin et al. 2022 | Intentional endometrial injury | No intervention (6) | 6 | NR/1006 | OR, 1.75 (1.29–2.36) | Moderate | Serious inconsistency | Critically Low |
| Maged et al. 2023 | Intentional endometrial injury | No intervention (9) | 9 | 325/1032 | OR, 1.24 (0.77–2.02) | Low | Very serious ROB, serious inconsistency | Low |
| He et al. 2023 | Intentional endometrial injury | No intervention (6) | 6 | NR/718 | OR, 1.83 (1.28–2.64) | Low | Very serious ROB, serious inconsistency | Low |
| Laboratory interventions | ||||||||
| PGT‐A | ||||||||
| Busnelli et al. 2021 | PGT‐A | No intervention | 2 | 85/230 | RR 1.07 (0.36–3.15) | Critically Low | Serious ROB, very serious inconsistency, serious imprecision | Low |
| He et al. 2023 | PGT‐A | No intervention | 2 | 85/230 | OR 1.51 (1.05–2.19) | Low | Serious ROB, serious inconsistency | Low |
| Study ID | Intervention | Comparison | No. RCTs | No. of patients with LB/Total no. | Summary estimate (95% CI) | GRADE assessment | Reasons for downgrading | AMSTAR‐2 rating |
|---|---|---|---|---|---|---|---|---|
| Immunomodulatory interventions | ||||||||
| G‐CSF | ||||||||
| Hou et al. 2021 | G‐CSF | Placebo (2) or no intervention (1) | 3 | NR/372 | RR, 1.43 (0.86–2.36) | Moderate | Serious inconsistency | Moderate |
| Wang et al. 2021 | G‐CSF | Placebo (2) | 2 | NR/320 | OR, 1.36 (0.74–2.51) | Low | Serious inconsistency, serious indirectness, serious imprecision | Critically low |
| Jin et al. 2022 | G‐CSF | Placebo (2) | 2 | NR/277 | Mean 1.45 (0.7–2.97) | Low | Very serious indirectness, serious inconsistency, serious imprecision | Critically low |
| Liu et al. 2022 | G‐CSF intrauterine | Placebo (2) | 2 | NR/411 | OR, 3.81 (2.53–5.72) | Moderate | NA | Critically Low |
| Kong et al. 2023 | G‐CSF | Placebo (3) | 3 | NR/413 | OR, 0.75 (0.35–1.59) | Low | Serious indirectness, serious inconsistency, serious imprecision | Low |
| Lu et al. 2023 | G‐CSF | Placebo (3) | 3 | 87/320 | RR, 1.51 (0.82–2.78) | Low | Serious ROB, serious inconsistency | High |
| He et al. 2023 | G‐CSF | Placebo (4) | 4 | NR/391 | OR, 1.55 (0.78–3.07) | Low | Serious ROB, serious inconsistency | Low |
| IVIG | ||||||||
| Achilli et al. 2018 | IVIG | Placebo (2) | 2 | 14/90 | OR, 2.1 (0.63–6.92) | Moderate | Serious imprecision | Critically low |
| GH | ||||||||
| Vera‐Montoya et al. 2023 | Growth hormone | No intervention (2) | 2 | 34/112 | OR, 5.13 (2.03–12.91) | High | NA | High |
| Intralipid | ||||||||
| Wang et al. 2021 | Intralipid | Placebo (1) or no intervention (1) | 2 | NR/244 | OR, 2.04 (0.99–4.19) | Low | Serious inconsistency, serious indirectness | Critically low |
| Zhou et al. 2020 | Intralipid | Placebo (2) or no intervention (2) | 4 | 117/544 | RR, 1.98 (1.39–2.8) | Moderate | Serious ROB | Low |
| Rimmer et al. 2021 | Intralipid | Placebo (3) or no intervention (2) | 5 | 46/203 | RR, 1.83 (1.42–2.35) | High | NA | Critically low |
| Kumar et al. 2021 | Intralipid | Placebo (2) or no intervention (3) | 5 | 185/763 | OR, 2.17 (1.54–3.05) | Low | Very serious ROB | Critically low |
| Han et al. 2021 | Intralipid | Placebo (3) or no intervention (2) | 5 | 205/840 | RR, 1.85 (1.44–2.38) | High | NA | Low |
| He et al. 2023 | Intralipid | No intervention (2) | 2 | NR/345 | OR, 2.29 (0.92–5.54) | Low | Serious ROB, serious inconsistency | Low |
| LMWH | ||||||||
| Liu et al. 2022 | LMWH | No intervention (2) | 2 | NR/357 | OR, 3.75 (2.53–5.56) | Moderate | Serious ROB | Critically Low |
| He et al. 2023 | LMWH | No intervention (4) | 4 | NR/538 | OR, 1.31 (0.71–2.58) | Low | Serious inconsistency, serious imprecision | Low |
| PBMC | ||||||||
| Wu et al. 2019 | PBMC | No intervention (2) | 2 | 59/235 | OR, 2.43 (1.32–4.49) | High | NA | Critically Low |
| Wang et al. 2021 | PBMC | Placebo (1) or no intervention (2) | 3 | NR/335 | OR, 2.96 (1.67–5.27) | Low | Serious inconsistency, serious indirectness | Critically Low |
| Jin et al. 2022 | PBMC | No intervention (2) | 2 | NR/312 | OR, 2.55 (1.27–5.11) | Moderate | Serious inconsistency | Critically Low |
| Liu et al. 2022 | PBMC | No intervention (2) | 2 | NR/567 | OR, 8.07 (4.88–13.33) | Low | Serious ROB, serious imprecision | Critically Low |
| Kong et al. 2023 | PBMC | No intervention (2) | 2 | NR/298 | OR, 0.44 (0.14–1.35) | Low | Serious ROB, serious inconsistency, serious indirectness, serious imprecision | Low |
| He et al. 2023 | PBMC | No intervention (4) | 4 | NR/389 | OR, 3.29 (1.51–7.5) | Moderate | Serious inconsistency | Low |
| PRP | ||||||||
| Jin et al. 2022 | PRP | Placebo (2) or no intervention (1) | 3 | NR/658 | OR, 5.96 (3.38–10.52) | Moderate | Serious inconsistency | Critically Low |
| Liu et al. 2022 | PRP | Placebo (1) or no intervention (1) | 2 | 93/473 | OR, 11.02 (5.72–21.21) | Low | Serious ROB, serious imprecision | Critically Low |
| Hu et al. 2022 | PRP | Placebo (1) or no intervention (1) | 2 | 91/433 | RR, 7.03 (3.91–12.66) | Low | Very serious ROB, serious imprecision | Critically Low |
| Maged et al. 2023 | PRP | Placebo (1) or no intervention (1) | 2 | 18/130 | OR, 2.36 (0.15–36.35) | Low | Serious ROB, serious inconsistency, serious imprecision | Low |
| Anitua et al. 2023 | PRP | Placebo (2) or no intervention (1) | 3 | 107/523 | RR, 3.36 (0.84–13.45) | Low | Very serious inconsistency | High |
| Kong et al. 2023 | PRP | Placebo (1) or no intervention (1) | 2 | NR/593 | OR, 0.27 (0.07–0.97) | Low | Serious ROB, serious inconsistency, serious indirectness | Low |
| He et al. 2023 | PRP | Placebo (2) or no intervention (1) | 3 | NR/563 | OR, 4.82 (2.13–9.95) | Low | Serious ROB, serious inconsistency | Low |
| Uterine and endometrial interventions | ||||||||
| Hysteroscopy | ||||||||
| Mao et al. 2019 | Hysteroscopy | No intervention (2) | 2 | NR/1160 | OR, 1.38 (0.8–2.38) | Moderate | Serious inconsistency | Critically low |
| He et al. 2023 | Hysteroscopy | No intervention (3) | 3 | NR/1480 | OR, 1.58 (0.9–2.85) | Low | Very serious Rob, serious inconsistency | Low |
| Intentional endometrial injury | ||||||||
| Potdar et al. 2012 | Intentional endometrial injury | No intervention (2) | 2 | 131/525 | RR, 2.63 (1.94–3.57) | High | NA | Low |
| Vitagliano et al. 2018 | Intentional endometrial injury | Placebo (1) or no intervention (6) | 7 | 145/702 | RR, 1.64 (1.21–2.21) | Moderate | Serious ROB | Moderate |
| Sar‐Shalom Nahshon et al. 2019 | Intentional endometrial injury | No intervention (3) | 3 | 73/276 | RR, 1.22 (0.52–2.82) | Low | Serious ROB, serious inconsistency, serious imprecision | Low |
| Busnelli et al. 2021 | Intentional endometrial injury | No intervention (3) | 3 | 83/376 | RR, 1.55 (0.81–2.94) | Moderate | Serious ROB | Low |
| Jin et al. 2022 | Intentional endometrial injury | No intervention (5) | 5 | NR/891 | OR, 1.7 (1.07–2.69) | Low | Serious inconsistency, very serious indirectness | Critically Low |
| Maged et al. 2023 | Intentional endometrial injury | No intervention (6) | 6 | 189/707 | OR, 0.95 (0.44–2.01) | Low | Very serious ROB, serious inconsistency, serious imprecision | Low |
| He et al. 2023 | Intentional endometrial injury | No intervention (3) | 3 | NR/396 | OR, 1.55 (0.77–3.16) | Low | Very serious ROB, serious inconsistency | Low |
| Laboratory interventions | ||||||||
| PGT‐A | ||||||||
| Busnelli et al. 2021 | PGT‐A | No intervention | 2 | 75/230 | RR 0.98 (0.32–2.94) | Critically low | Serious ROB, very serious inconsistency, serious imprecision | Low |
| He et al. 2023 | PGT‐A | No intervention | 2 | 75/230 | OR 1.01 (0.54–1.90) | Low | Serious ROB, serious inconsistency | Low |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsReproductive System and Pregnancy · Endometriosis Research and Treatment · Reproductive Health and Contraception
INTRODUCTION
1
Assisted reproductive techniques continue to evolve, many patients still experience serial in vitro fertilization (IVF) failures. Implantation is a complex process involving various factors related to the embryo, endometrium, and the immune system.1, 2 Recurrent implantation failure (RIF) presents a challenging condition characterized by the inability to achieve pregnancy, determined by persistently negative human chorionic gonadotropin levels, even after undergoing multiple embryo transfers (ETs).3, 4, 5 While definitions of RIF agree on the recurrent nature of the condition, there is a lack of consensus on the specific number of failed attempts.2, 6 The pathogenesis of RIF is multifaceted,2 and numerous interventions have been proposed for its management.7, 8
The European Society for Human Reproduction and Embryology (ESHRE) developed good practice recommendations in early 2023 for RIF management.9 These recommendations were an amalgam of expert opinions and a literature review (PubMed 1950–August 10, 2022), prioritizing randomized clinical trials (RCTs) but also including relevant observational studies without evidence grading.10 Several network meta‐analyses have ranked interventions for their effectiveness in different orders.11, 12, 13, 14, 15 Thus, there are varying recommendations. An umbrella review with evidence grading of systematic reviews (SR) and meta‐analyses (MA) could aid in interpreting these findings and provide clinicians with a more thorough and transparent evidence‐based approach.
The objective of this umbrella review was to systematically review and assess the strength of evidence pertaining to interventions for the management of RIF within SRs of RCTs reporting clinical pregnancy rates (CPR) or live birth rates (LBR) as outcomes.
METHODS
2
We conducted this overview of SRs after prospective registration (PROSPERO no. CRD42023414255) and reported it in accordance with the PRISMA (Preferred Reporting Items for Meta‐analyses guidelines)16 (Table S1).
Search strategy and selection criteria
2.1
A comprehensive search strategy without language restriction was applied in electronic databases (Medline, Scopus, Cochrane Library) from inception until March 25, 2024. We used a combination of keywords and free text terms including “Recurrent implantation failure,” “implantation failure,” “meta‐analyses,” “meta‐analysis” and “randomized controlled trials.” The search terms are presented in Appendix S1. All citations found were exported to Endnote software (version X9), where duplicates were removed. Two reviewers (AI and FC) carried out the searches independently and screened all abstracts and titles using Rayyan software. We included SRs comprising RCTs assessing interventions (stand‐alone interventions compared to a placebo or no treatment) for RIF. The SR with MA encompassed interventions for RIF treatment, defined a priori within categories in the latest ESHRE recommendations (2023) (9), regardless of the specific definition of RIF used. Four nodes were identified to classify these interventions: (i) interventions based on diagnostic findings (include antibiotic treatment); (ii) immunomodulatory interventions (include intravenous immunoglobulin (IVIG)); peripheral blood mononuclear cells (PBMC) infusion; subcutaneous or intrauterine granulocyte colony‐stimulating factor (G‐CSF) administration; intrauterine autologous platelet‐rich plasma (PRP) infusion; intravenous intralipid; intrauterine human chorionic gonadotropins (hCG) injection; low molecular weight heparin (LMWH); (iii) uterine and endometrial interventions (include: intentional endometrial injury; hysteroscopy; GnRH agonist and aromatase inhibitor pretreatment; sildenafil); and (iv) laboratory interventions (include: preimplantation genetic testing for aneuploidy (PGT‐A)). The clinical outcomes of interest were clinical pregnancy rates (CPR) or live birth rates (LBR) reported as either primary or secondary outcomes. The exclusion criteria were reviews and studies which did not report these outcomes, and their designs were other than SR or MA, that is, narrative reviews and reviews of non‐RCT evidence. Any disagreement regarding the inclusion of the citations was resolved by obtaining the opinion of a third researcher (NC‐I).
Data extraction, methodological quality assessment and evidence grading
2.2
The characteristics of selected studies, methodological quality assessment and evidence grading was extracted by AI and checked for accuracy by FC after reading the full text. Extracted data included citation details (author and year), type of intervention, comparator, the number of RCTs included, number of participants, the ratings of their quality, and pooled effect sizes with their 95% confidence intervals (CI) for the outcome: CPR or LBR. The pooled effect estimates, and heterogeneity of estimates were those reported within each included MA. The methodological quality of the included SRs was independently assessed by two reviewers (AI and FC) using the 16‐item questionnaire, that is, a measurement tool for assessment of multiple systematic reviews (AMSTAR‐2).17 Disagreements were resolved via consultation with a third reviewer (NC‐I). According to the guidelines, the reviewers assigned one of four global quality ratings (i.e., high, moderate, low or critically low) after the consideration of 16 potential critical and noncritical weaknesses. High and moderate ratings reflected the presence of one or less or one noncritical weakness, respectively. Low and critically low ratings indicated one or more than one critical weakness, respectively.
Using Grading of Recommendations Assessment, Development and Evaluation (GRADE) methodology,10 the strength of evidence was categorized as high, moderate, low, or critically low, considering five domains: risk of bias of included studies, indirectness of evidence, inconsistency of results (heterogeneity), imprecision of results and possibility of publication bias.18 The risk of bias was assessed based on the quality of the included RCTs, with grading categorized as “not serious,” “with serious limitations,” or “with very serious limitations,” depending on the assessment tool used by the included MA. Indirectness was evaluated through the population, intervention, comparator, outcome (PICO) framework. If the MA clearly defined these elements, the domain was considered “not serious.” Inconsistency was assessed using the I^2^ score, with a score above 50% classified as a “serious limitation” and a score exceeding 80% considered a “very serious limitation.” Imprecision was evaluated based on point estimates, CIs, and P values, with thresholds set around 0.75 and 1.25.19 A point estimate below 1 with an upper CI limit exceeding 1.25, or a point estimate of 1 or higher with a lower CI limit falling below 0.75, was marked as a “serious limitation.” Finally, for assessing publication bias, data from the funnel plots and Egger tests reported in the included MAs were utilized.18
Data synthesis
2.3
The extracted data in each SR were structured and the findings were tabulated, including the overall number of RCTs and participants. Significant summary results were grouped by intervention and outcomes to present an overview of direction and magnitude of effect. The corrected covered area (CCA) was calculated to quantify the degree of overlap between SRs. Analysis of overlap was performed by groups of MAs determined by: (a) The type of evaluated interventions, and (b) the reported pre‐specified outcomes of the study: CPR and live birth rates. CCA is a percentage, calculated as (N − r)/(rc − r), where N is the number of publications included in the evidence synthesis, r is the number of rows and c is the number of columns. CCA below 5% was considered a slight overlap, a CCA >5 and ≤10% a moderate overlap, a CCA >10 and ≤15% a high overlap, and a CCA >15% as a very high overlap.20 The results with statistically significant improvements for each intervention were counted as a percentage of the total taking into account the evidence strength assessed by GRADE. With many interventions, vote‐counting conducted within broad subgroups stratified by evidence strength assessment is known to minimize bias by incorporating quality. It has previously been used to synthesize whether evidence showed improvement or no change.21, 22, 23
RESULTS
3
Of the total of 1401 records were initially identified, 47 SRs met the eligibility criteria including a total of 375 RCTs. Out of 47, eight SRs did not have MAs; of these, three SRs had only one RCT each. Seven SRs had unextractable MA data for RCTs only. Out of the included 32 SRs with MA, six SRs had multiple MAs.7, 11, 12, 13, 14, 15 There were 98 MAs of RCTs. Figure 1 presents the PRISMA16 flow diagram of the selection process. A list of studies excluded from the overview with the main reason for their exclusion are summarized in Table S2.
Flow chart of the systematic reviews included in the umbrella review of interventions for the treatment of recurrent embryo implantation failure.
Characteristics of the included systematic reviews
3.1
The main characteristics of the selected SRs are described in Table S3. All included SRs were published between 2012 and 2023, and their searches for RCTs were conducted between 2012 and 2022. Only one of the SRs was a Cochrane Review.24 Total number of MAs for CPR were 59 and that for LBR were 39. Of the total SRs, 32 (237 RCTs) covered immunomodulatory interventions, 10 (68 RCTs) covered uterine and endometrial interventions, one (1 RCT) covered antibiotics, and four (69 RCTs) covered mixed approaches.
Methodological quality assessment and overlap of evidence
3.2
Using AMSTAR 2 tool (Table S4), three SRs (6%) were rated as high methodological quality,25, 26, 27 three were rated as moderate methodological quality (6%),28, 29, 30 19 (41%) were evaluated as low quality,7, 14, 15, 24, 31, 32, 33, 34, 35, 36, 37, 38, 39, 40, 41, 42, 43, 44, 45 and 22 (47%) were critically low quality.11, 12, 13, 38, 46, 47, 48, 49, 50, 51, 52, 53, 54, 55, 56, 57, 58, 59, 60, 61, 62, 63 The high‐quality reviews were conducted for immunomodulatory interventions G‐CSF26; growth hormone (GH); PRP.25 Regarding the SRs with moderate quality, one pertained to PBMC,29 another focused on G‐CSF,28 and one SR was related to endometrial scratch.30 Among the AMSTAR‐2 criteria (Figure 2), the most frequent critical weakness identified were the lack of a previous protocol review (27 SRs), the exclusion studies without robust justification (31 SRs); and an inappropriate investigation of publication bias (11 SRs). The AMSTAR‐2 assessment of methodological quality revealed that the majority of the included SRs (42 out of 47) described the risk of bias in the incorporated studies. A degree of overlap was found between SRs, with a median CCA of 33.3% (IQR 45.15%, min 0%–max 100%) (Table 1). Tables 2 and 3 show the strength of the evidence between proposed interventions and each selected clinical outcome.
*Methodological quality of 47 Systematic reviews included in the umbrella review of interventions for the treatment of recurrent embryo implantation failure. Quality assessment according to the 16 items of AMSTAR 2 (see Section 2 for details). Item 1: Research questions and inclusion criteria include PICO components; Item 2: Previous protocol review; Item 3: Explaining decision about the study designs to include in the review; Item 4: Adequate literature search; Item 5: Study selection performed in duplicate; Item 6: Data extraction performed in duplicate; Item 7: Excluded studies justification; Item 8: Describing included studies with sufficient detail; Item 9: Bias risk of individual studies included; Item 10: Reporting the sources of funding for the studies included in the review; Item 11: Appropriate meta‐analysis methods; Item 12: Assessing the potential impact of bias risk on results; Item 13: Consideration of the bias risk in the interpretation of the review results; Item 14: Satisfactory explanation and discussing any observed heterogeneity in the review results; Item 15: Assessment of the presence and probable impact of publication bias; and Item 16: Potential sources of conflict including any funding received. Critical items: 2, 4, 7, 9, 11, 13 and 15; Non‐critical items: 1, 3, 5, 6, 8, 10, 12, 14 and 16.
Effect of interventions
3.3
The changes in CPR and LBR associated with different interventions for RIF grouped by evidence strength (GRADE assessment) are given in Figures 3 and 4. The evidence strength for CPR was high‐moderate in 36 MAs and low‐critically low in 23 MAs. The evidence strength for LBR was high or moderate in 17 MAs and low or critically low in 22 MAs. Granulocyte colony‐stimulating factor (G‐CSF) showed improvement in CPR in 13/14 (93%) MAs (9/13, 69.2% high‐moderate evidence strength) and in LBR in 1/7 (14%) MAs (moderate evidence strength). Intralipid infusion showed improvement in CPR in 6/6 (100%) MAs (4/6, 57.14% high‐moderate evidence strength) and in LBR in 4/6 (66.6%) MAs (3/4, 75% high‐moderate evidence strength). Peripheral blood mononuclear cells (PBMC) showed improvement in CPR in 8/9 (88%) MAs (4/8, 50% high‐moderate evidence strength) and in LBR in 5/6 (83.33%) MAs (3/5, 60% high‐moderate evidence strength). Platelet‐rich plasma (PRP) intervention showed improvement in CPR in 10/11 (91%) MAs (6/10, 60% high‐moderate evidence strength) and in LBR in 5/7 (71.42%) MAs (1/5, 20% moderate evidence strength). Human chorionic gonadotropins (hCG) showed improvement in CPR in 3/4 (75%) MAs (3/3 (100%) high‐moderate evidence strength). Growth hormone (GH) showed improvement in CPR in 1/1 (100%) MA (1/1, 100% high evidence strength) and in LBR in 1/1 (100%) MA (1/1, 100% high evidence strength). Low molecular weight heparin (LMWH) showed improvement in CPR in 1/3 (33.33%) MAs (1/1, 100% moderate evidence strength) and in LBR in 1/2 (50%) MAs (1/1, 100% moderate evidence strength). For uterine and endometrial interventions, hysteroscopy showed improvement in CPR in 2/2 (100%) MAs (1/2, 50% moderate evidence strength). Intentional endometrial injury showed improvement in CPR in 4/7 (57.14%) MAs (3/4, 75% high‐moderate evidence strength) and in LBR in 3/7 (42.86%) MAs (2/3, 66.66% high‐moderate evidence strength). For laboratory interventions, preimplantation genetic testing for aneuploidy (PGT‐A) showed improvement in CPR in 1/2 (50%) MAs (1/1, 100% low evidence strength), but not LBR.
Change in clinical pregnancy rate (CPR) associated with different interventions for recurrent implantation failure grouped by evidence strength (GRADE assessment) of meta‐ analyses included in umbrella review. Data presented as 100% stacked bar chart with numbers inside bars indicating number of meta‐analyses with statistically significant improvements (color code: Gray) or no difference (color code: White) (see Table 2 for details of meta‐analysis).
Change in live birth rate (LBR) associated with different interventions for recurrent implantation failure grouped by evidence strength (GRADE assessment) of meta‐analyses included in umbrella review. Data presented as 100% stacked bar chart with numbers inside bars indicating number of meta‐analyses with statistically significant improvements (color code: Gray) or no difference (color code: White) (see Table 3 for details of meta‐analysis).
DISCUSSION
4
Principal findings
4.1
This overview assessed 47 SRs, encompassing 375 RCTs, on the effectiveness of various interventions for RIF in terms of CPR and LBR. According to our search, this is the only comprehensive overview with methodological quality and evidence strength assessment focusing on interventions for RIF. Overall, among the 10 different interventions reviewed, we found that nine demonstrated statistically significant support for improving CPR, and seven showed similar results for LBR. Most of the significant meta‐analytical associations (32 out of 52 for CPR and 12 out of 16 for LBR) were of high or moderate evidence strength, as assessed by GRADE. Our review indicated that the majority of interventions for RIF involved immunomodulatory treatments, particularly G‐CSF, PRP, PBMC, and intralipid infusion. Eight interventions (G‐CSF, PBMC, PRP, GH, hCG, intralipid infusion, LMWH, and intentional endometrial injury) statistically demonstrated superiority over placebo or no intervention in enhancing clinical outcomes for patients with RIF.
For instance, while historical evidence suggested a consistent trend with considerable certainty regarding the benefits of G‐CSF and PRP in improving CPR, recent findings indicate no significant improvement. Similarly, although earlier studies showed a consistent trend with considerable certainty for Intralipid infusion in enhancing CPR and LBR, recent evidence offers only limited support for CPR improvement. For PBMC, evidence shows a converging and convincing trend supporting improvements in clinical outcomes. In contrast, there is limited evidence to support the use of GH, hCG, hysteroscopy, and LMWH for improving clinical outcomes. Although intentional endometrial injury was previously associated with a consistent trend and considerable certainty for improving clinical outcomes, recent findings indicate no significant improvement. As for PGT‐A, there is limited evidence showing no improvement in CPR and LBR; however, in clinical practice, it may be proposed as a pragmatic approach to address embryo aneuploidy in patients with advanced maternal age and RIF, in alignment with ESHRE recommendations.9 It is essential to consider adverse events associated with pharmacological administration when implementing or recommending treatments in clinical practice, to carefully balance the potential benefits and risks.
Strength and limitations
4.2
The review was reported according to established guidelines. We conducted a comprehensive search, updated during the course of our work, to capture the most current literature. We opted for an overview of reviews to help explore the heterogeneity in the populations, interventions, and outcomes studied. Our overview indicated the tendency or direction of the effect of interventions in RIF patients. We systematically appraised the evidence presented in the reviews. This work incorporated evidence from 98 MAs. To enhance transparency, we assessed the evidence of RCTs using the GRADE framework.
Our analysis primarily focused on summarizing the synthesized effects. In our appraisal of methodological quality, we did not re‐evaluate the original statistics reported, such as the I ^2^ metric for between‐study heterogeneity, nor did we reassess evidence for small‐study effects. This approach may limit our understanding of study variability and potential biases within the reviewed literature. When evaluating the results of the meta‐analyses in our umbrella review, it is crucial to note that the individual studies included were extensively scrutinized in the original reviews. Thus, our conclusions are based on the interpretations and summary estimates of pooled effects presented by the authors of these meta‐analyses. There was a notable degree of overlap among the RCTs included in the systematic reviews and meta‐analyses, indicating that numerous studies were repeatedly included across some meta‐analyses but not others. This repetition may inadvertently amplify the influence of certain studies in the umbrella review, a phenomenon attributable to the timeframe of the searches or the year of publication. It is anticipated that more recent meta‐analyses would incorporate newer studies while also encompassing earlier ones. Additionally, the variability in population characteristics, comparators, and outcome measures restricted the synthesis of results. Despite these limitations, this umbrella review stands as the first to systematically summarize current evidence regarding the effectiveness of interventions for RIF treatment in an umbrella review.
Comparison with current overviews and future recommendations
4.3
To our knowledge, this is the first umbrella review of its kind. This review emphasizes the challenges in evaluating evidence syntheses due to overlap and generally variable methodological quality, underscoring the need for higher‐quality intervention studies rather than the publication of additional meta‐analyses. Existing overviews, in the form of network meta‐analyses, present heterogeneous conclusions, ranging from recommendations for new RCTs to advocating for specific interventions.11, 12, 13, 14, 15 Such reviews tend to mix up placebo and no treatment when constructing the networks. Authors and readers are advised to consult the AMSTAR‐2 guidelines prior to conducting and using meta‐analyses for RIF interventions, as inferences depend heavily on the methodological quality of evidence syntheses. The existing network meta‐analyses often compare interventions with controls that mix placebos and no interventions together. Future network meta‐analyses should evaluate whether there is a placebo effect. If a placebo effect is present, future trials should ethically be required to consider using placebo instead of no treatment as a comparator. Overall, more rigorously designed primary studies are necessary to clearly demonstrate the effects of interventions on clinical outcomes in RIF patients and to further explore the distinct components that make interventions effective.
CONCLUSIONS
5
Immunomodulatory interventions such as G‐CSF, PRP, PBMC, intralipid infusion, and intentional endometrial injury could potentially enhance the management of RIF patients based on evidence of high to moderate strength. However, the heterogeneity due to variations in the definitions of RIF places provisos on the interpretation of these findings.
AUTHOR CONTRIBUTIONS
Conceptualization: Abdulla Almohammadi, Fadi Choucair. Data curation: Abdulla Almohammadi, Fadi Choucair. Formal analysis: Abdulla Almohammadi, Fadi Choucair, Naomi Cano‐Ibáñez. Supervision: Aurora Bueno‐Cavanillas, Khalid S Khan. Visualization: Abdulla Almohammadi, Fadi Choucair, Aurora Bueno‐Cavanillas, Khalid S Khan. Writing – original draft: Abdulla Almohammadi, Fadi Choucair. Review and editing: Abdulla Almohammadi, Fadi Choucair, Aurora Bueno‐Cavanillas, Khalid S Khan, Naomi Cano‐Ibáñez.
FUNDING INFORMATION
No funding was required or obtained for this research.
CONFLICT OF INTEREST STATEMENT
The authors declare no conflicts of interest.
Supporting information
Data S1. Supporting Information.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Fox C , Morin S , Jeong J‐W , Scott RT Jr , Lessey BA . Local and systemic factors and implantation: what is the evidence? Fertil Steril. 2016;105(4):873‐884.26945096 10.1016/j.fertnstert.2016.02.018PMC 4821679 · doi ↗ · pubmed ↗
- 2Das M , Holzer HE . Recurrent implantation failure: gamete and embryo factors. Fertil Steril. 2012;97(5):1021‐1027.22425200 10.1016/j.fertnstert.2012.02.029 · doi ↗ · pubmed ↗
- 3Polanski LT , Baumgarten MN , Quenby S , Brosens J , Campbell BK , Raine‐Fenning NJ . What exactly do we mean by ‘recurrent implantation failure’? A systematic review and opinion. Reprod Biomed Online. 2014;28(4):409‐423.24581986 10.1016/j.rbmo.2013.12.006 · doi ↗ · pubmed ↗
- 4Rinehart J . Recurrent implantation failure: definition. J Assist Reprod Genet. 2007;24:284‐287.17674185 10.1007/s 10815-007-9147-4PMC 3455006 · doi ↗ · pubmed ↗
- 5Simon A , Laufer N . Assessment and treatment of repeated implantation failure (RIF). J Assist Reprod Genet. 2012;29:1227‐1239.22976427 10.1007/s 10815-012-9861-4PMC 3510376 · doi ↗ · pubmed ↗
- 6Macklon N . Recurrent implantation failure is a pathology with a specific transcriptomic signature. Fertil Steril. 2017;108(1):9‐14.28602479 10.1016/j.fertnstert.2017.05.028 · doi ↗ · pubmed ↗
- 7Busnelli A , Somigliana E , Cirillo F , Baggiani A , Levi‐Setti PE . Efficacy of therapies and interventions for repeated embryo implantation failure: a systematic review and meta‐analysis. Sci Rep. 2021;11(1):1747.33462292 10.1038/s 41598-021-81439-6PMC 7814130 · doi ↗ · pubmed ↗
- 8Cimadomo D , Craciunas L , Vermeulen N , Vomstein K , Toth B . Definition, diagnostic and therapeutic options in recurrent implantation failure: an international survey of clinicians and embryologists. Hum Reprod. 2021;36(2):305‐317.33313697 10.1093/humrep/deaa 317 · doi ↗ · pubmed ↗