Leukaemia-associated priapism in children (LAPC): reviewing clinical outcomes and management strategies
Abhijit Shah, KR Surag, Anupam Choudhary, Kasi Viswanath, AVB Krishnakanth, Chaitanya Krishna, Padmaraj Hegde, S Gayathri, PM Swathi

TL;DR
This review examines priapism in children with leukemia, highlighting the importance of early diagnosis and combined treatment for better outcomes.
Contribution
The study provides a scoping review of leukaemia-associated priapism in children, analyzing clinical outcomes and management strategies.
Findings
Chronic myeloid leukaemia was the most common malignancy associated with priapism in children.
Early management with corporal lavage and cytoreductive measures improved long-term erectile function outcomes.
Three children died, while 14 survivors retained erectile function after treatment.
Abstract
Priapism is a prolonged penile erection for more than 4 hours unrelated to sexual stimulation. Rarely, it is the first clinical sign of an underlying haematological malignancy. A similar presentation is noted in childhood leukaemias. Although rare, it is known to occur and, if not managed early, can have poor long-term outcomes in terms of erectile function and psychosexual growth. We present a scoping review of leukaemia-associated priapism in children (LAPC). We researched literature using PubMed, Google Scholar, Embase, Scopus and Cochrane databases from January 1990 to 2024. Applicable search limiters were applied, and grey literature was excluded. A total of 31 articles were finally included in the review, from which 51 cases of LAPC were isolated and studied. The average age was 11.5 years, with chronic myeloid leukaemia (CML) being the most common malignancy (68.9%), and more…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
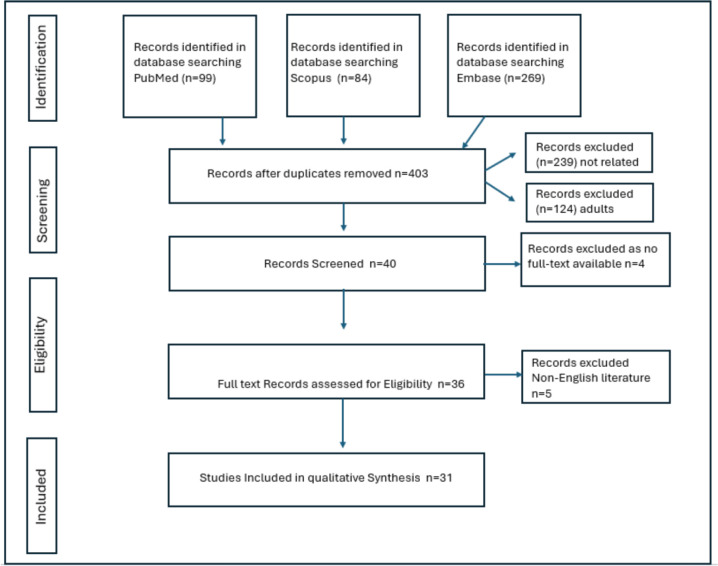 Figure 1
Figure 1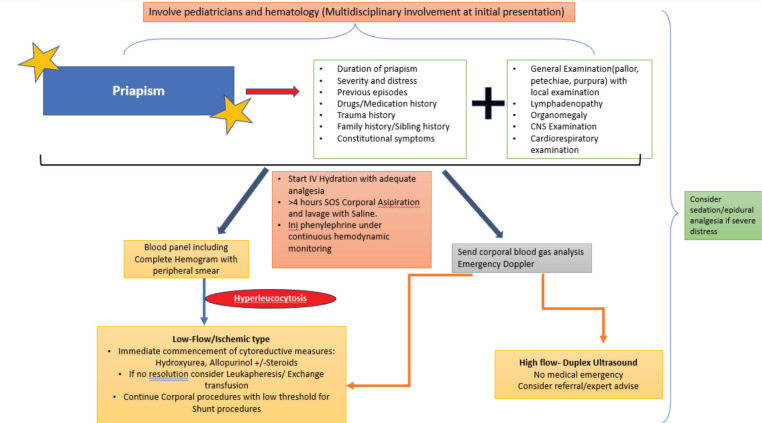 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGenital Health and Disease · Sexual function and dysfunction studies · Urinary Bladder and Prostate Research
Introduction
Priapism refers to the prolonged and persistent erection of the penis, hours beyond (>4 hours) or unrelated to sexual stimulation [1,2]. This persistent erection is due to persistently engorged corpus cavernosum secondary to a vascular disturbance that typically controls penile rigidity. Sickle cell disease is the most common cause of priapism in children (65%), whereas leukaemia-associated priapism in children (LAPC) incidence rates are 10% [3]. Data on LAPC are sparse, and so are the outcomes of its management.
The present review is undertaken to (a) assess the characteristics and types of leukaemia and their role in LAPC, (b) describe the management options available and (c) investigate the outcomes.
Methodology
We researched English literature from January 1990 to 2024 (PubMed, Google Scholar, Cochrane, Scopus and Embase) for original articles, reviews, case series and case reports for search terms ‘Priapism’ and (‘Leukaemia’ or ‘Lymphoma’) and (‘childhood’ or ‘all children (birth-18 years)’), excluding terms ‘sickle cell’, ‘female’ and ‘Adult’. We also excluded grey literature data from this review. Thirty-one studies were finally included in our review after excluding duplicates, including those with no full text, and applying our limiters (Figure 1). Our study was registered with PROSPERO ‘CRD42024519022’, and PRISMA-ScR reporting guidelines [4] were adhered to.
Results
We reviewed a total of 51 cases in 31 different studies. The overall data on LAPC are quite scarce, and this is noted in numerous case reports (28 out of 31 studies). The remaining three studies are case series (≥3 cases), which include a population-based registry study on chronic myeloid leukaemia (CML) and another paper studying the impact of leukapheresis in acute myeloid leukaemia (AML) [5–7]. One case report mentions two cases, one of which was of an adult. Hence, only the paediatric case has been included [8].
The median age in our review was 12 years (3–17 years), and the median duration, in 37.3% of cases after the onset of priapism to presentation in the hospital, was 24 hours (n = 19). However, various reports mention recurring or stuttering priapism occurring a few days or a few weeks before the presentation, with no mention of the exact time of presentation from the latest episode of priapism [5, 9, 10]
The search showed the most frequent disorder being CML, 68.9% (n = 35). The chronic phase of CML was the most common phase of onset of priapism and presentation to the clinician (71.4%), followed by blast crisis and accelerated phase (11.4% and 8.6%, respectively). The four remaining reports did not mention the blast percentages or the phase of CML. The median age of the CML cohort was 14 years (4–17 years) Of the 35 cases, 32 cases had palpable splenomegaly, and three reports failed to mention the examination findings. The median white blood cell (WBC) count was 450,000/μL (135,000/μL–899,000/μL). Table 1 reviews chronic leukaemia cases and their characteristics, and Table 2 reviews the priapism-directed management and eventual outcomes. Apart from imatinib, hydroxyurea, allopurinol and steroids were recorded medications in these case reports. Thirty-seven percent of cases (n = 13) report using corporal lavage with saline or phenylephrine injections and adequate hydration as the initial management step. Surgical intervention in the form of a distal shunt (Winter and Ebbehoj) was performed in six cases, of which one needed revision to a proximal shunt procedure for eventual detumescence [11]. One case documented bilateral internal iliac artery embolization [12]. Very few of these studies mentioned the eventual follow-up outcomes. Of those, three cases of erectile dysfunction [12–14] were mentioned, along with one death secondary to pneumonitis post-stem cell transplant [5].
Of the acute leukaemias (Table 3) associated with priapism, the median age was younger (9.3 years and 3–16 years), and the most common subtype was B cell acute lymphoblastic leukaemia (ALL) followed by T cell ALL and AML. Of the 16 cases of acute leukaemias, 11.8% (n = 6) were B-ALL cases, 9.8% (n = 5) cases were T-ALL, 5.9% (n = 3) AML and 2 cases were ALL with subtype not mentioned. The median WBC in acute leukaemia cases noted was 423,500/μL (27,300/μL–693,000/μL). Acute leukaemias were overall associated with a rapid progression of the underlying disease with an earlier presentation (<24 hours in 43.8% of acute cases, n = 7) and two reports of death due to central nervous system (CNS) leukaemia [15] and septic shock [16]. From the available data, 7 cases (43.8%) of acute leukaemias were in remission. However, the overall long-term erectile function outcomes in this cohort are not available (except in one case where the erectile function was preserved [6]).
Discussion
Etiopathogenesis
Hinman [17] first reported the ischemic nature of priapism based on aspiration of deoxygenated blood due to increased viscosity, congestion and reduced flow. Eponymous with the Greek–Roman mythological figure Priapus, son of Aphrodite, priapism was first described in the literature in 1616 by Petraens. It was almost 260 years later; this condition was first recorded in a child [18, 19]
Priapism is subdivided into three types: high-flow/non-ischemic/arterial type, low-flow/ischemic type and stuttering/recurring type (common in sickle cell disease). It is the low-flow/ischemic type that is painful, may result in irreversible damage through fibrosis if left untreated for 24–36 hours and has been strongly implicated with leading to impotence in 35%–90% of men [20–24]. It becomes essential to differentiate the clinical type of priapism to prevent long-term, irreversible effects [1, 25–27].
Priapism in leukaemia is hypothesised to occur via different mechanisms [28–30]. The most likely mechanism could occur due to venous obstruction secondary to microemboli/thrombi and increased microviscosity due to increased circulating blood cells (‘symptomatic hyperleukocytosis’, also known as ‘leukostasis’). Hyperleukocytosis is defined as a WBC greater than 1,00,000/μL in patients affected by leukaemias. The incidence of hyperleukocytosis ranges from 5% to 13% in AML and from 10% to 30% in ALL [31]. However, symptomatic hyperleukocytosis is higher in AML than in ALL [32] and also typically occurs with much higher WBC counts in the case of ALL than in patients with AML. The reason is that myeloid blasts are larger and more rigid than lymphoid blasts, and myeloid blasts secrete cytokines, which upregulate endothelial cell adhesion, whereas in chronic leukaemia such as CML, WBCs are usually segmented neutrophils, metamyelocytes and myelocytes, which are smaller and more deformable. Hence, symptomatic hyperleukocytosis is very rare in this patient population and is mostly seen in the accelerated phase or blast crisis or the overall leukocyte counts are extremely high for the symptoms of LAPC to occur [29, 30, 33, 34].
In addition, increased mechanical pressure from veins draining the spleen, which is often enlarged in paediatric CML, and infiltration of the nervous system by leukemic cells, more so in acute leukaemias, have also been implicated in causing priapism [5]. Microscopically, the release of cytokines by malignant cells causes endothelial cell activation, which further causes increased sequestration of leukemic cells in the microvasculature. One report also suggests the isolation of leukemic cells that directly infiltrated into the penile tissue, leading to penile mass in AML [35], while another suggests an involvement of the hypothalamus in LAPC [16]
Incidence and clinical presentation
CML is a myeloproliferative neoplasm of mature granulocytes. Three stages of CML exist: chronic phase, accelerated phase and blast phase. In one of the largest paediatric cohort studies on priapism in children due to CML, Suttorp et al [5] reported an incidence of priapism of 3.2%, with 75% in the chronic phase of CML. This is similar to the findings of our review (71.5%). Ninety percent of paediatric cases of CML are discovered during the chronic phase.
Acute leukaemias with priapism are an even rarer finding. During the initial presentation, some report concomitant CNS symptoms such as headaches and blurred vision with retinal bleeding [15, 36–38], while some report fatigability owing to anaemia, petechiae and rashes, renal insufficiency owing to tumour lysis syndrome, neck swelling and lower urinary tract symptoms [6, 10, 16, 37, 39]. The underlying disease progress is much more rapid in ALL patients, and hence, the incidence of LAPC recorded is much rarer in this subgroup of patients. Three cases are reported with AML, of which Salou et al [9] report the priapism associated with the deposition of leukemic cells in extramedullary sites leading to myeloid sarcoma of the sacral canal. Priapism is reported during treatment in this report; however, this finding was not substantiated in another study on conus medullaris syndrome due to myeloid sarcoma leading to urinary and defecation disorders [40].
Management and long-term outcomes
Priapism is a urological emergency that needs to be addressed early to prevent permanent risk of erectile dysfunction, which is predicted to be >90% if it lasts for more than 24 hours [41]. Children with underlying leukaemia need to be started on disease-directed therapy at the earliest, be it chemotherapy, tyrosine kinase inhibitor or cytoreductive measures with hydration, hydroxyurea and leukapheresis when warranted. However, these measures should not defer the emergency treatment of priapism itself.
Figure 2 depicts a proposed management algorithm for patients presenting with LAPC. The initial management is crucial as it dictates the erectile outcomes and long-term prognosis of these patients. In our study, 20 cases (39.2%) were reportedly subjected to corporal lavage in addition to disease-directed measures. The rest were managed with cytoreductive measures supplemented with adequate IV hydration and analgesia.
Systemic interventions, such as cytoreductive measures with hydroxyurea, allopurinol and steroids, have been shown to reduce the white cell count [5, 42]. In cases where an acute control of leucocyte count is warranted or the cytoreductive measures fail to establish a reduced leucocyte count, leukapheresis or exchange transfusion methods are commonly employed [5, 43, 44]. Seventeen patients (33%) underwent leukapheresis, of which 12 were noted in CML cases. Suttorp et al [5], Ponniah et al [43] and Veljković et al [45] all demonstrate its usefulness for CML cases associated with priapism.
Certain adjunct treatments noted in our review worth revisiting were bilateral internal iliac artery embolization with urokinase [12] and epidural analgesia [37]. If a paediatric anaesthetist is present, low-dose ketamine has been suggested to resolve priapism in some cases and may help to relieve pain during corporal lavage and shunt procedures in these children [46–50]
From a surgical standpoint, a urologist must be aware of various types of shunt procedures that may be performed in cases of unresolved priapism. Distal shunts, such as the Winter, Ebbehoj and T-Shunt, are easier to create. Seideman and Gitlin [51] describe the successful use of a T-Shunt in refractory ischemic priapism in a paediatric patient. In this review, we report a similar use of distal shunts in refractory priapism [5, 14, 52–55]. Thakur et al [11] report failure of distal shunt, which was later converted to a proximal shunt with success.
Fifteen cases (29.4%) from the entire cohort reported a preserved erectile function on follow-up. Follow-up data are as sparse as the original literature on LAPC. However, it is of utmost importance that on the initial presentation itself, the patient’s family must be made aware of the possible loss of erectile function in the future, despite the clinician’s best efforts. Teenagers and their parents often do not discuss sexual health in boys [26, 42]. This was also witnessed in a cohort of boys with sickle cell disease with priapism, who reported embarrassment to report their complaints to their parents, even in the emergency room when it became a medical emergency [27].
There are definite limitations present in this review, the first of which is the prevalence of only case reports, as this condition is rare. This gives rise to varied management methods, which need streamlining, as we attempted in our study. Follow-up data on many children in terms of erectile status remain unknown. A multi-institutional collaboration with their respective registries may further help define a protocol to manage LAPC and help to trace and contact the patient or next of kin and provide follow-up data.
Conclusion
Though rare, priapism may be the only presenting symptom of haematological malignancies in children. Thus, it is essential to examine for organomegaly and do a complete hemogram with peripheral smear examination in all children presenting with priapism. Considering ischemic priapism, a urological emergency and the potential risk of permanent damage later in life, managing solely with systemic anti-leukaemia therapies (chemotherapy and/or leucopheresis) may not be sufficient for early resolution. Concurrent cavernosal management with corporal lavage and injectable sympathomimetics may help resolve the acute condition and prevent long-term erectile sequelae and psychosocial problems.
Conflicts of interest
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Funding
This research did not receive any specific grant funding agencies in the public, commercial or not-for-profit sectors.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Bivalacqua TJ Allen BK Brock GB The diagnosis and management of priapism: an AUA/SMSNA guideline 2022 executive summary J Urol 20222081435210.1097/JU.000000000000276735536142 · doi ↗ · pubmed ↗
- 2Salonia A Bettocchi C Boeri L European Association of Urology guidelines on sexual and reproductive health-2021 update: male sexual dysfunction Eur Urol 20218033335710.1016/j.eururo.2021.06.00734183196 · doi ↗ · pubmed ↗
- 3Burnett AL Bivalacqua TJ Priapism: current principles and practice Urol Clin North Am 200734463164210.1016/j.ucl.2007.08.00617983902 · doi ↗ · pubmed ↗
- 4Tricco AC Lillie E Zarin WPRISMA extension for scoping reviews (PRISMA-Sc R): checklist and explanation Ann Intern Med 201816946747310.7326/M 18-085030178033 · doi ↗ · pubmed ↗
- 5Suttorp M Sembill S Kalwak K Priapism at diagnosis of pediatric chronic myeloid leukemia: data derived from a large cohort of children and teenagers and a narrative review on priapism management J Clin Med 20231214477610.3390/jcm 1214477637510891 PMC 10380995 · doi ↗ · pubmed ↗
- 6Castagnetti M Sainati L Giona F Conservative management of priapism secondary to leukemia Pediatr Blood Cancer 20085142042310.1002/pbc.2162818506758 · doi ↗ · pubmed ↗
- 7Bruserud O Liseth K Stamnesfet S Hyperleukocytosis and leukocytapheresis in acute leukaemias: experience from a single centre and review of the literature of leukocytapheresis in acute myeloid leukaemia Transfus Med 20132339740610.1111/tme.1206723919332 · doi ↗ · pubmed ↗
- 8Gaye O Thiam NM Cassell A Unusual presentation of priapism associated with acute and chronic myeloid leukemia in two patients: emergency management Case Rep Urol 2020131510.1155/2020/4982432 PMC 744299132855834 · doi ↗ · pubmed ↗