Paediatric urachal rhabdomyosarcoma: the role of radiotherapy about a case report and review
Salem Ouaddane Alami, Fatima-Zahra Abdelli, Samia Khalfi, Zenab Alami, Touria Bouhafa

TL;DR
This case report highlights the successful use of radiotherapy in treating a rare pediatric cancer called urachal rhabdomyosarcoma.
Contribution
The paper emphasizes the role of radiotherapy in managing urachal rhabdomyosarcoma, a rare pediatric malignancy.
Findings
The patient showed a 70% tumor reduction after chemotherapy and successful surgical resection.
Radiotherapy targeting the primary tumor and metastases was well-tolerated with no significant side effects.
The patient remained recurrence-free for one year following treatment.
Abstract
This report discusses the case of a 10-year-old girl diagnosed with rhabdomyosarcoma (RMS) of the urachus, a rare form of soft tissue cancer in paediatric oncology. RMS, representing 3%–4% of paediatric cancers, arises from primitive muscle cells and requires a multidisciplinary treatment approach. The goal of this case is to enhance understanding of radiotherapy's role in treating RMS in children, particularly in rare sites like the urachus. The patient, with no significant medical history, presented with right lower abdominal pain and was found to have a large abdominal mass. Imaging revealed a massive necrotic tumour and pulmonary metastases. The tumour was initially deemed unresectable, and a biopsy confirmed RMS. Chemotherapy was initiated using the RMS 2005 protocol, which resulted in a 70% tumour reduction. Surgical resection was then performed, and the patient received…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
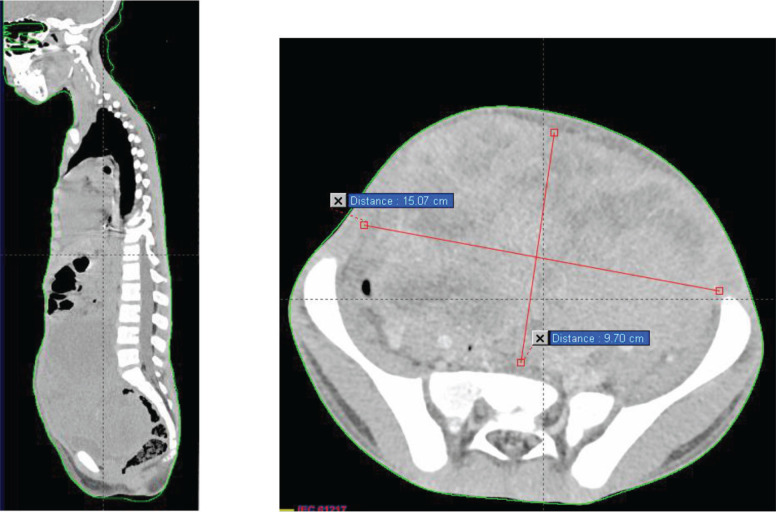 Figure 1
Figure 1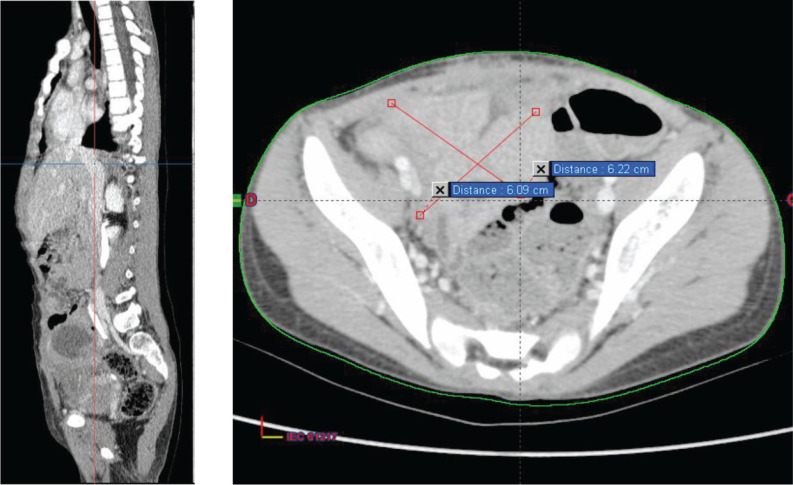 Figure 2
Figure 2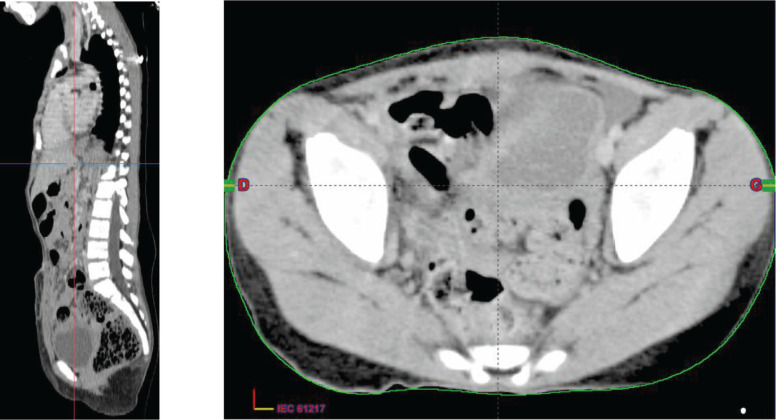 Figure 3
Figure 3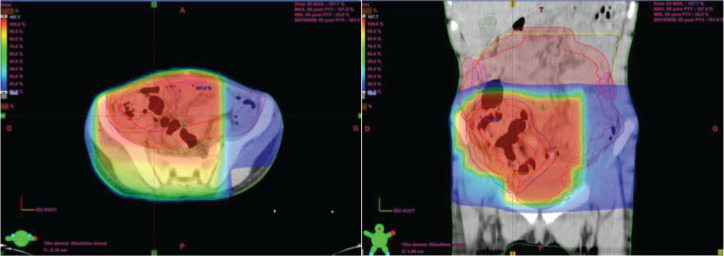 Figure 4
Figure 4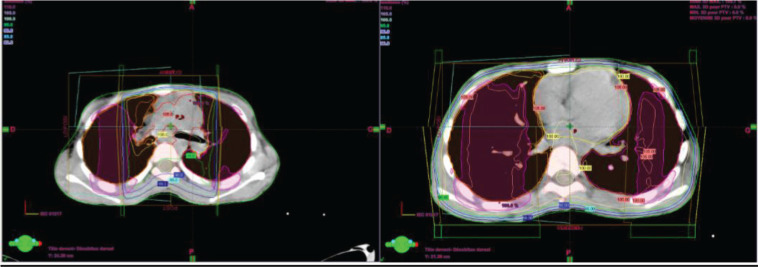 Figure 5
Figure 5Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsUrinary and Genital Oncology Studies · Urological Disorders and Treatments · Urologic and reproductive health conditions
Introduction
This report delves into the clinical case of a 10-year-old girl diagnosed with rhabdomyosarcoma (RMS) of the urachus, a rare manifestation of soft tissue cancer that poses a particular challenge in the field of paediatric oncology. RMS, which represents about 3%–4% of all paediatric cancers [1], is characterized by the proliferation of primitive muscle cells, and it requires a complex and multidisciplinary approach to management. Through this case, we aim to deepen the understanding of radiotherapy in the context of rhabdomyosarcoma in children, thereby contributing to the enhancement of knowledge and improvement of treatment strategies for this rare localization.
Case
It is about a 10-year-old girl with no notable medical history, admitted for further management of an alveolar-type rhabdomyosarcoma of the urachus, classed high risk, which started approximately 10 months prior to admission with right lower quadrant abdominal pain, prompting her parents to consult a paediatrician.
On initial clinical examination by paediatricians, a large abdominopelvic mass was found, occupying the entire abdomen, measuring 14 cm in its longest axis and 8 cm in its shortest axis, with no precise determination of its origin. The abdominal circumference was 54 cm, with the presence of a right inguinal lymph node measuring approximately 1 cm.
A thoraco-abdominopelvic CT scan (Figure 1) revealed a large mass and pulmonary macronodules involving both lung fields, more prominently on the right side. The two largest masses measured 43 × 25 mm in the right lower lobe and 38 × 30 mm in the right upper lobe. Additionally, there were mediastinal, pre, subcarinal and pre-tracheal lymph nodes, massively necrotic, with the two largest measuring 42 × 32 mm at the right hilum and 46 × 25 mm at the subcarina. These lymph node masses exhibited similar enhancements to the previously described pulmonary masses and macronodules.
Moving to the abdominal–pelvic region, a large, massively necrotic abdominopelvic mass was observed, occupying almost the entire abdomen and pelvis, lateralized to the right, polylobed and peripherally vascularized, measuring roughly 136 × 93 × 170 mm. This mass compressed all adjacent digestive structures laterally and inferiorly, causing significant bladder displacement towards the left side. It also compressed the uterus posteriorly, as well as the rectum and rectosigmoid region.
Furthermore, compression of the right ureter with dilation of the upstream collecting system was noted, with the right renal pelvis measuring 15 mm in transverse diameter and a parenchymal index measuring 9 mm in diameter on the right. External and common iliac lymph nodes were also observed, more pronounced on the right side, the largest measuring 13 mm in diameter.
The tumour was considered unresectable, and therefore, it was decided to perform a surgical biopsy. The histopathological and immunohistochemical examination revealed an aspect of an NOS rhabdomyosarcoma.
The decision made during the multidisciplinary team meeting was to proceed with the RMS 2005 protocol. Chemotherapy based on the IVA regimen was initiated 15 days after her admission. The patient received four cycles with good clinical tolerance, showing no mucositis, proctitis, diarrhoea, or signs of infection. Clinical examination revealed a reduction in tumour size from 10 to 7 cm, prompting the performance of a second thoraco-abdominopelvic CT scan (Figure 2) that shows a significant regression of the abdominopelvic tumour process, as well as pulmonary and nodal metastases, estimated to be over 70%.
Then, it was decided to add 2 additional cycles of chemotherapy at 21-day intervals (CEV+IVE) and to reassess with a CT scan for surgical planning. After completion of chemotherapy, a third thoraco-abdominopelvic CT scan showed that the tumour had become resectable.
Then, a surgical procedure was conducted to remove a mass measuring 6 cm in its largest dimension originating from the urachus (Figure 3).
Two weeks after surgery, the child was referred to our radiotherapy department. The approach was to proceed with three-dimensional conformal radiotherapy (3DCRT) targeting the primary tumour volume along with the bilateral internal and iliac areas, at a dose of 41.4 Gy delivered in 23 fractions at 1.8 Gy per fraction (Figure 4). In addition, sequential 3DCRT irradiation of the pulmonary and mediastinal metastases was planned at a dose of 15 Gy, administered in 10 fractions at 1.5 Gy per fraction (Figure 5).
No side effect was observed with radiation therapy, notably neither diarrhoea nor vomiting or other complications.
The follow-up every 3 months for 1 year was marked by an improvement in the general condition of the girl without any clinical or radiological signs of recidivism.
Discussion
RMS is a paediatric soft tissue malignancy with poor survival rates for high-risk and recurrent diseases and has the potential for significant morbidity associated with treatment [2]. It accounts for 4.5% of all cases of childhood cancer [3]. This is the third most common extracranial solid tumour of childhood after Wilms’ tumour and neuroblastoma. The median age of presentation is 6 years; however, this disease follows a bimodal distribution with peak incidences between 2 and 6 years and again between 10 and 18 years of age [4].
Although the prognosis of RMS has improved over the past 30 years due to multimodal therapies [5], the urachal origin of RMS is still extremely rare and insufficiently identified.
Few single cases were reported in the literature with only one paediatric series, including eight cases of urachal RMS in children 6]. Details about the only 13 cases of urachal RMS reported in the English literature are provided in Table 1.
While there are no known tumour markers or distinct known causes, some studies have found an association between RMS and certain environmental exposures such as prenatal X-rays and parental recreational drug use [7]. It can also be seen with increased frequency in those with Neurofibromatosis type 1, Li-Fraumeni, Beckwidth Widemann, DICER-1 syndrome, Costello syndrome and Noonan syndrome [7, 8].
The preperitoneal location permits significant asymptomatic spread within the Retzius space. This silent progression leads to a delayed diagnosis. Symptoms manifest only when the tumour reaches a large size, causing compression of adjacent organs. Urachal tumours are discovered as a hypogastric palpable mass without haematuria, except adenocarcinomas [9]. The size of the mass can make it challenging to identify its primary origin. Management of RMS should aim for a cure with minimal morbidity. Block radical cystectomy is no longer the primary treatment. Instead, the most appropriate surgical approach is considered to be total mass resection while preserving quality of life. Given that urachal RMS is often extensive, surgery is typically preceded by chemotherapy to reduce the tumour size and facilitate a less aggressive resection. Surgery and radiotherapy are the cornerstones of local treatment for RMS. Their primary goal is to cure patients while ensuring minimal long-term sequelae.
Conclusion
Although rhabdomyosarcoma is the most common soft tissue tumour in children, tumours originating from the urachus are extremely rare. Treatment primarily involves surgery, with radiotherapy also playing a role in managing RMS. Additional research is needed to standardize the management protocol for these tumours.
Conflicts of interest
There are no conflicts of interest.
Funding
This article was funded by ecancer.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Mc Evoy MT Siegel DA Dai S Pediatric rhabdomyosarcoma incidence and survival in the United States: an assessment of 5656 cases, 2001–2017 Cancer Med 202312336443656[https://www.ncbi.nlm.nih.gov/pmc/articles/PMC 9939205/#:~:text=Rhabdomyosarcoma%20(RMS)%20is%20a%20malignant,annually%20in%20the%20United%20States]10.1002/cam 4.521136069287 PMC 9939205 · doi ↗ · pubmed ↗
- 2Zarrabi A Perrin D Kavoosi M Rhabdomyosarcoma: current therapy, challenges, and future approaches to treatment strategies Cancers 202315215269[https://www.mdpi.com/2072-6694/15/21/5269]10.3390/cancers 1521526937958442 PMC 10650215 · doi ↗ · pubmed ↗
- 3Ries LAG Melbert D Krapcho MSEER Cancer Statistics Review (1975–2004)2007 Bethesda National Cancer Institute
- 4Miller RW Young JL Novakovic B Childhood cancer Cancer 1995751 Suppl 39540510.1002/1097-0142(19950101)75:1+<395::AID-CNCR 2820751321>3.0.CO;2-W 8001010 · doi ↗ · pubmed ↗
- 5Gartrell J Pappo A Recent advances in understanding and managing pediatric rhabdomyosarcoma F 1000 Res 20209 F 1000 Faculty Rev-685 [https://pubmed.ncbi.nlm.nih.gov/32695311/]10.12688/f 1000 research.22451.1PMC 734417432695311 · doi ↗ · pubmed ↗
- 6Cheikhelard A Irtan S Orbach D Urachal rhabdomyosarcoma in childhood: a rare entity with a poor outcome J Pediatr Surg 201550813291333[https://pubmed.ncbi.nlm.nih.gov/25913896/]10.1016/j.jpedsurg.2014.12.02325913896 · doi ↗ · pubmed ↗
- 7Skapek SX Ferrari A Gupta AA Rhabdomyosarcoma Nat Rev Dis Primers 2019511[https://www.ncbi.nlm.nih.gov/pmc/articles/PMC 7456566/]10.1038/s 41572-018-0051-230617281 PMC 7456566 · doi ↗ · pubmed ↗
- 8Townsend MF Gal AA Thoms WW Ureteral rhabdomyosarcoma Urology 1999543561[https://www.sciencedirect.com/science/article/abs/pii/S 0090429599001612]10.1016/S 0090-4295(99)00161-210754139 · doi ↗ · pubmed ↗