A Comparison Between Multisonic and Ultrasonic Irrigant Activation Techniques for Multispecies Biofilm Removal During Root Canal Disinfection: A Systematic Review
Preethi Varadan, Sangavi Ra, Mathan R Rajendran

TL;DR
This systematic review compares multisonic and ultrasonic techniques for removing biofilms during root canal disinfection.
Contribution
The study provides a comparative analysis of multisonic and ultrasonic methods for multispecies biofilm removal in root canals.
Findings
Three studies were included, evaluating biofilm removal in extracted teeth models.
The GentleWave® multisonic System outperformed ultrasonic activation in most studies.
Both techniques showed similar efficacy in reducing intraradicular biofilm.
Abstract
This systematic review aims to compare multisonic and ultrasonic irrigant activation techniques in polymicrobial biofilm removal. We conducted a literature search involving SCOPUS, PubMed, Cochrane, EBSCO host, and LILACS databases from inception to December 2024, in addition to a manual search using Google Scholar. The risk of bias assessment was done using the guidelines described for in vitro studies and the criteria for evaluation was based on JBI criteria and CRIS guidelines for quality assessment of in vitro studies. Three articles were included in the final analysis. The included studies evaluated biofilm removal in extracted teeth models incubated with biofilm; while two studies used quantitative polymerase chain reaction (qPCR) methodology, one used colony forming unit (CFU). Except in the study by Llerena et al., the GentleWave® multisonic System (GWS) outperformed ultrasonic…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
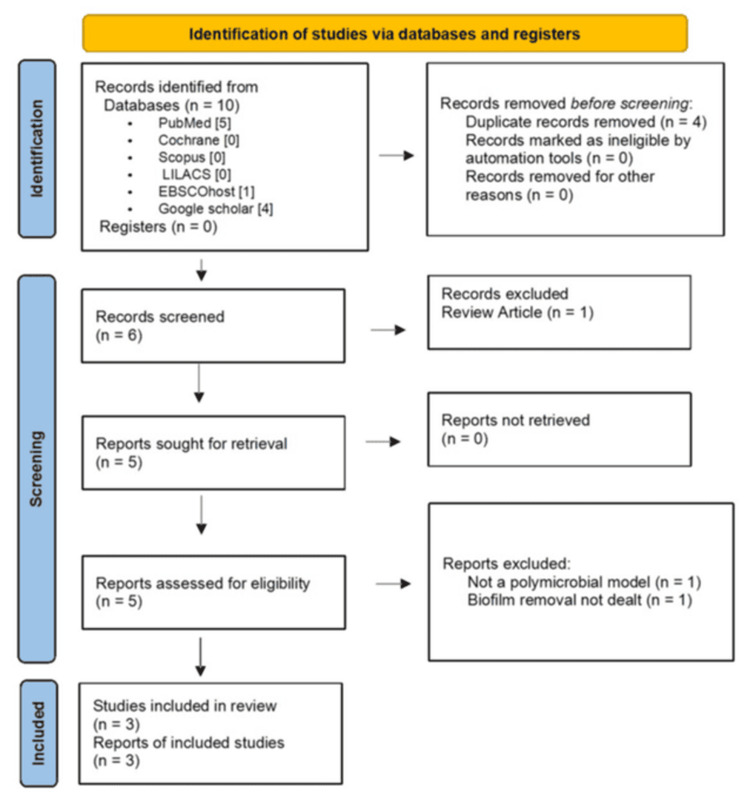 Figure 1
Figure 1|
| Author and year of publication | Reason for exclusion |
| 1 | Choi et al., 2019 [ | The study used monospecies biofilm model |
| 2 | Velardi et al., 2022 [ | The study did not evaluate biofilm removal |
| Study | Type of teeth | Sealing of apex | Species tested | Culture medium | Incubation period | Groups | Apical preparation size | Results | Conclusions |
| Coaguila-Llerena et al., 2022 [ | 22 lower molars (Vertucci type II) | Sealed | 10 bacterial taxa, including Streptococcus, Parvimonas, Fusobacterium, Prevotella, Veillonella, Mogibacterium, Slackia, Selenomonas, Stomatobaculum, and Lancefieldella, were tested | BHI broth | 2 weeks | Group GWS (n = 11); Group PUI (n = 11) | For GWS: V-Taper 20.06. For ultrasonic: Vortex Blue 35.04 | Both groups had no differences in results between pre- and post-treatment samples. Pre-treatment communities differed from post-treatment samples in both groups regarding bacterial taxa reduction | GWS and PUI showed a similar bacterial reduction |
| Zhang et al., 2018 [ | 20 extracted human molars | Sealed | E. faecalis and Streptococcus mutans were tested | BHI broth | 2 weeks | Group GWS (n = 26 canals); Group PiezoFlow (n = 30 canals) | For GWS: Vortex Blue 15.04. For PiezoFlow: Vortex Blue 35.04 | The reduction in the mean number of bacteria was 99.91% for GWS and 98.01% for the PiezoFlow system | GWS showed a high level of bacterial DNA reduction in comparison to the PiezoFlow system |
| Alquria et al., 2023 [ | 70 single-rooted lower premolars (Vertucci type I) | Not reported | E. faecalis and E. coli were investigated | BHI broth | 3 weeks | 1) Positive control group (n = 14); 2) GWS + minimally invasive technique group (MIT) (n = 14); 3) PUI (ProUltra) + conventional instrumentation technique group (n = 14); 4) XP-Endo Finisher (XPEF) + conventional instrumentation technique group (n = 14) | For GWS: Vortex Blue 20.04. For PUI: Vortex Blue 35.04 | PUI + conventional instrumentation technique, XPEF + conventional instrumentation technique, and GWS + minimally invasive technique were highly effective against bacteria with GWS with MIT being the most effective | GWS + minimally invasive technique was the most effective |
| Study | Irrigation protocol | Volume of irrigants | Methods of sampling | Evaluation methods |
| Coaguila-Llerena et al., 2022 [ | For PUI, a 20.02 size ultrasonic tip was coupled to a piezoelectric device (EndoUltra), and 2 ml of the solution was activated for 20 secs. The procedure was repeated thrice for a total final irrigation time of 1 minute. The same procedure was repeated for 17% ethylenediaminetetraacetic acid (EDTA). GWS was used at a 1-min cycle with distilled water, a 4-min cycle with 3% sodium hypochlorite (NaOCl), a 1-min cycle with 8.5% EDTA, and a 1-min cycle with distilled water finally. After final irrigation, all the canals were irrigated with 2 ml of 10% sodium thiosulfate (STS) for 3 min to inactivate the NaOCl | For PUI, the total NaOCl volume of final irrigation per canal was 6 ml. However, for GWS, the volume was not reported | Paper point sampling method | Quantitative polymerase chain reaction (qPCR), 16S ribosomal RNA gene sequencing (next-generation sequencing) method was used |
| Zhang et al., 2018 [ | For ProUltra PiezoFlow, the irrigation protocol used was 3% NaOCl for 1 min per canal, sterile water for 10 s per canal, 8% EDTA for 1 min per canal, and sterile water for 10 s per canal. For GWS, the irrigation protocol used was 3% NaOCl for 3 mins, sterile water for 30 s, 8% EDTA for 2 min, and final irrigation with sterile water for 15 secs | Not reported | Paper point sampling method | Both the 16S ribosomal RNA gene-targeted qPCR method and culturing method were used |
| Alquria et al., 2023 [ | For PUI, 5 ml of 3% NaOCl for 3 mins followed by 5 ml of 17% EDTA for 3 mins, and a final flush of 5 ml of 3% NaOCl for 3 mins was used. To inactivate NaOCl, 5 mL sterile 0.5% STS for 1 min was used. For GWS, an irrigation protocol of 3% NaOCl for 5 min, sterile water for 15 s, 17% EDTA for 2 min, and a final flush of sterile water for 15 s was used. The root canals were finally irrigated with 5 mL sterile 0.5% STS for 1 min and rinsed with sterile saline solution (SSL) to inactivate NaOCl. For XP-Endo Finisher, the irrigation protocol was 17% EDTA for 1 min and 5 mL of 3% NaOCl. This protocol was repeated 2 times. A final flush of 3% NaOCl was performed and the NaOCl effect was inactivated with 5 mL sterile 0.5% STS for 1 min | Not reported | Paper point sampling method | Colony forming unit (CFU) method was used |
| Author | Sample size calculation | Tooth randomization | Sample preparation and handling | Biofilm standardization | Incubation period | Control group | Appropriate statistical analysis | Total score |
| Coaguila-Llerena et al., 2022 [ | - | - | + | + | + | - | + | 4 |
| Duo et al., 2018 [ | - | - | + | + | + | - | + | 4 |
| Alquria et al., 2023 [ | - | + | + | + | + | + | + | 6 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsEndodontics and Root Canal Treatments · Nosocomial Infections in ICU · Oral microbiology and periodontitis research
Introduction and background
Endodontic infections are caused by different bacterial species organized in a mixed biofilm community, similar to most human endogenous infections, dental caries, and marginal periodontitis [1]. The canal irregularities such as apical ramifications, lateral canals, isthmuses, dentinal tubules, and recesses harbor bacteria, often organized in biofilm-like structures [2]. Planktonic cells and flocs in the main root canal are easily accessed and eliminated by instrumentation and irrigants. However, the biofilm adherent in the inaccessible areas distant from the main canal is challenging to remove. Biofilms persist due to their various mechanisms for evading treatment such as protection by the enclosing polysaccharide matrix, intrinsic resistance to endodontic disinfectants, and ability to survive and adapt to new environments by activating survival genes and following alternate metabolic pathways. Partial elimination of such endodontic microbes might result in the reorganization of species, predisposing to unfavorable treatment outcomes and flare-ups [1].
Root canal rendered free of biofilm is favored for obturation. However bacterial load reduction conducive to healing is the primary goal. From a microbiological standpoint, eradication or significant disruption of biofilm architecture is difficult. This is further challenged by the anatomical complexities of root canals which are impossible to sterilize [2]. Mechanical disruption of the tenacious biofilm structure and smear layer is required for broad-spectrum chemical disinfectants to exert their action on cells inside the matrix. Strategic delivery of irrigants to the canals is needed to potentiate the chemical effects of disinfectants [2].
Ultrasonic activation acts mainly by the agitation of the surrounding irrigant rather than a direct physical effect confined to the main root canal. At 30 kHz, the oscillatory motion of the tip generates acoustic streaming, which transports the irrigant from the main root canal to the remote zones. It increases the wall shear stress to improve the mechanical effect. Under certain circumstances, the swiftly changing irrigant pressure might foster transient acoustic cavitation. The higher shear wall stress along with locally increased pressure and temperature evoke sonochemical effects by accelerating the chemical reactions. Two types of ultrasonic irrigation have been elucidated in the literature: continuous ultrasonic irrigation (CUI) and passive ultrasonic irrigation (PUI) [3].
The mechanical efficacy of ultrasonic irrigant activation in biofilm removal from lateral morphological features in root canals and decontaminating dentinal tubules has been studied in monospecies, dual-species, and multispecies biofilm [4]. However, several studies have focused on bacterial load reduction in Enterococcus faecalis (E. faecalis) biofilm models, which is not representative of the antimicrobial efficacy in vivo [5]. GentleWave® System (GWS), a new irrigant activation system combining multisonic frequencies and negative apical pressure has been introduced for root canal disinfection with minimal preparation sizes. This multisonic system creates a broad range of frequencies that traverse the entire root through the irrigant. These broad-spectrum acoustic waves are believed to impart root canal cleanliness during the collapse of hydrodynamic cavitation bubbles [5]. Studies have demonstrated favorable results for GWS in removing biofilm, intracanal bacterial DNA, calcium hydroxide medication, residual debris, separated instruments, gutta-percha/sealer in retreatment, and calcifications [6].
The key difference between the two systems is that ultrasonic activation is performed in each canal separately, whereas GWS actively circulates the irrigant simultaneously in all root canals, thereby minimizing the working time. Ultrasonics solely depend on the acoustic streaming of an oscillating file whose effect is limited when used in narrow canals. However, with regard to multisonic systems such as GWS, irrigant activation is achieved by the production of a broad spectrum of sound waves that deliver irrigants throughout the root canal [6,7].
The decontamination of infected root canals is a crucial aspect of endodontic treatment, with effective antimicrobial strategies being essential for preventing persistent infections. Previous studies have compared the effectiveness of multisonic and ultrasonic activation techniques in reducing polymicrobial load. Some studies have reported the superiority of multisonics over ultrasonics, while others have demonstrated no significant difference in the reduction of microbial contamination. However, there remains a lack of consensus on the most effective technique for biofilm disruption and decontamination. Additionally, there are no comprehensive systematic reviews in the literature comparing the antibiofilm efficacy of these techniques when used with different endodontic irrigants. This systematic review aims to compare the antibiofilm efficacy of different ultrasonic and multisonic activations of endodontic irrigants in multispecies biofilms.
Review
Research proposal and research question
The research proposal was registered in the PROSPERO database with the PROSPERO ID: CRD42024583277. The review question per Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines was as follows: “Does multisonic irrigant activation effectively remove intraradicular biofilm when compared to ultrasonic irrigant activation?”
Materials and methods
PICO(S) Analysis
Population (P): Polymicrobial biofilm models
Intervention (I): Multisonic irrigant activation
Comparison (C): Ultrasonic irrigant activation
Outcome (O): Biofilm removal Study design
Study design (S): In vitro studies
Eligibility Criteria
In vitro studies comparing ultrasonic and multisonic irrigant activation techniques performed exclusively on polymicrobial biofilm models were included in this systematic review. Studies with no available full text, review articles, conference abstracts, case reports, and studies evaluating monospecies biofilm removal were excluded.
Study Selection and Data Extraction
A literature search was undertaken involving the databases PubMed, Cochrane, LILACS, SCOPUS, and EBSCO host from inception to December 2024, and a manual search was performed using Google Scholar from inception to December 2024. Two independent reviewers (PV and SR) screened the titles and abstracts of articles obtained from the preliminary search. Complete texts of the relevant studies were evaluated based on the inclusion criteria. A PRISMA flowchart detailing the study selection is depicted in Figure 1. The data extracted from the finalized articles included author name, year of publication, tooth type, sealing of apex, species tested, culture medium, incubation period, comparison groups, sample size, NiTi instrument used, apical preparation size (diameter and taper), irrigation protocol (duration, time, volume of irrigant), sample collection method, evaluation method for biofilm removal, results obtained and conclusion of the studies. Any disagreement in study selection was resolved by consulting with a third reviewer (MR).
PRISMA flowchart illustrating the study selection processPRISMA: Preferred Reporting Items for Systematic Reviews and Meta-Analyses
Search Terms
The studies were selected with the use of search terms such as “Biofilm removal” OR “Biofilm eradication” OR “Biofilm disruption” OR “Biofilm detachment” OR “Biofilm disassembly” OR “Microbial reduction” OR “Multispecies biofilm” OR “Polymicrobial biofilm” OR “Dual species biofilm” OR “Polymicrobial biofilm models” “Ultrasonically activated irrigation” OR “Ultrasonic activation” OR “Passive ultrasonic irrigation” OR “CK file” OR “IrriSafe” OR “Endosonic Blue” “Multisonic irrigant activation” OR “Gentlewave system” OR “Cleanflow technology”.
Qualitative Analysis of the Included Studies
Three independent analysts evaluated the methodological quality of the studies using the guidelines reported for in vitro studies. The evaluation criteria adopted were modified from the CRIS and JBI guidelines for quality assessment of in vitro studies. In case of discrepancies between the two examiners, a third reviewer was consulted to sort out the disagreement. The risk of bias assessment criteria included sample size estimation, sample preparation and handling, randomization of samples, biofilm standardization, incubation period, presence of a control group, and appropriate statistical analysis.
Results
Ten articles were identified from the preliminary search. After removing duplicates, the screening of titles and abstracts was performed for five studies, after which one article was excluded as it did not meet the inclusion criteria. The excluded studies and the reason for their exclusion are summarized in Table 1. On full-text screening of the remaining four articles, one article was excluded as it did not evaluate biofilm removal. Finally, three articles [5,7,8] were included for qualitative analysis. The clinical characteristics of the included studies are summarized in Tables 2-3.
All the studies were published between 2018 to 2023. Among the included studies, two used molars, while Alquria et al. [8] utilized premolars for biofilm incubation. Regarding the biofilm models, two studies sealed the apex of the tooth, whereas Alquria et al. [8] did not mention whether the apex was sealed in their study. Zhang et al. [7] grew three-week-old E. faecalis and Streptococcus biofilms while Alquria et al. [8] used two-week-old E. faecalis and E. coli dual-species biofilms in their study. Llerena et al.'s study [5] study predominantly focused on 10 bacterial taxa (Streptococcus, Parvimonas, Veillonella, Mogibacterium, Fusobacterium, Prevotella, Slackia, Selenomonas, Stomatobaculum, and Lancefieldella) for two weeks. All the studies used BHI broth, which is an anaerobic culture medium. Except in the study by Alquria et al. [8], a control group was not included, and randomization of samples was not performed.
For both CUI & PUI, all the studies used Vortex blue NiTi instruments till 35.04 for canal preparation. For GWS, the apical preparation size was different for each study. Llerena et al. [5] had used V-taper till 20.06. Vortex blue had been used till 35.04 by Alquria et al. [8] and 15.04 by Zhang et al. [7]. None of the studies mentioned the final irrigant volume used for each group [5,7,8]. After final irrigation, all canals were irrigated with sodium thiosulfate to inactive the sodium hypochlorite (NaOCl) carry-over effect, except Zhang et al. [7]. All the studies had collected samples from the region of interest using paper points.
All of the included studies evaluated biofilm removal in extracted teeth models incubated with biofilm; two studies used quantitative polymerase chain reaction (qPCR) methodology, and the other study used colony forming units (CFU). In all studies except Llerena et al. [5], GWS outperformed PUI in biofilm removal.
Risk of Bias Assessment
The evaluation criteria were revised based on the CRIS and JBI guidelines for assessing the quality of in vitro studies. Two of the three included studies displayed a high risk of bias while one showed a moderate risk of bias. None of the authors had revealed the sample size derivation. Tooth randomization was done in Alquria et al.'s [8] study. All the studies had specified details about sample preparation and handling, biofilm standardization, incubation period and statistical analysis performed. Alquria et al. [8] had a control group while the remaining studies had no control group. Regarding irrigation protocols in treatment groups, Alquria et al. [8] did not mention the working length till the ultrasonic tip was inserted and the frequency with which PUI was operated. In Llerena et al. (2022) [5] and Zhang et al. (2019) [7], the power setting of PUI is not specified. The quality assessment of the included articles is presented in Table 4.
Discussion
None of the selected studies included a priori sample size calculation in the study design. Inadequate sample size and methodological flaws in sampling and detection lead to erroneous inferences about different automated irrigant activation techniques. This mandates researchers to effectuate changes in in vitro models to study the root canals relevant to the clinical scenario. Culture methods allow either an absolute or partial quantification of culturable bacteria. However, under laboratory conditions, a significant number of microbiotas in the root canal space cannot be cultured. E. faecalis appeared to be commonly associated with persistent or secondary endodontic infections based on culture and closed-end methods such as PCR during the last two decades [8-12]. This has been challenged by contemporary studies that shed light on a complex bacterial composition evident in failed cases. Mature biofilm differs from an early biofilm with respect to biomass and antimicrobial resistance. All the included studies in this review designed mature biofilm models.
Gram-negative species are uncommon in post-instrumentation or medication samples, which indicates that they are easily eliminated, unlike gram-positive bacteria. Since gram-positive species are the most challenging to eliminate, their usage is justifiable. Because a given treatment might have different effects on gram-negative and gram-positive bacteria, studies have included both species [13]. Llerena et al. [5] used dental plaque samples, which are undefined natural biofilms, as well as a CDC reactor to generate reproducible microcosm biofilms [14]. Zhang et al.'s [7] study used a multispecies biofilm comprising E. faecalis and Streptococcus mutans. Alquria et al. [8] used a dual-species biofilm model comprising E. coli LPS, which is commercially available and accessible. However, this gram-negative species is not usually found in root canal infections.
All the included studies employed sterile paper points for sample collection. Although paper point samples are routinely used for intracanal microbiological studies, they do not reach inaccessible regions like accessory canals, fins, and dentinal tubules where residual biofilms persist. Underestimation of the intraradicular infection levels and biofilm removal from those inaccessible regions is likely to result from this technique. To overcome that limitation, cryogenic grinding was used in Alquria et al. [8]. However, if the tooth is pulverized, sequential sampling cannot be done.
Desired features of ideal irrigation methods include the ability to deliver the irrigant to the complete root canal system, refresh the irrigants to compensate for consumption, and apply shear stress on targets to detach them from the canal wall, thus manifesting a reverse flow to carry detached materials and depleted irrigant out of the canals and prevent inadvertent extrusion. Although irrigation protocol and biofilm model were standardized in terms of canal anatomy and microbiology, it is impractical to match the irrigant volume, canal preparation diameter, and taper, as different numbers of files were used in each group.
PUI should be carried out with an apical preparation size of 30-35 for unobstructed oscillation. A higher power setting leads to more intense streaming, but the dentist should be mindful of instrument separation and inadvertent dentin removal. Most manufacturers recommend 30-35 % of maximum available power. Shorter periods of intermittent activation combined with irrigant replenishment is commonly used than a high-flow rate continuous delivery system. Intermittent activation involving three cycles of 20 seconds is a popular protocol, though a shorter time of 10 seconds can also be employed. Continuous ultrasonic activation creates high shear wall stress at the apical third resulting in an improved reduction of adherent biofilm than intermittent ultrasonic irrigation and conventional syringe irrigation. However, the PUI power setting is not mentioned in the studies by Llerena et al. [5] and Zhang et al. [7].
Multisonic activation was promoted as a stand-alone irrigation method and the GW system is designed to work on minimal (apical enlargement to size 15-25) or even uninstrumented canals. Conversely, a study by Lee et al. (2019) [14] stated that apical diameter is not a relevant factor if irrigants are activated. Hence, the results with the minimal preparation sizes with GWS are favorable in preserving the pericervical dentin without compromising the disinfection, ultimately retaining the resistance against tooth fracture. Also, it produces negative apical pressure, which is believed to prevent irrigant extrusion significantly. To eliminate the dissolved gas present in the solution and eliminate the vapor lock effect, the irrigants undergo a degassing process. When the irrigant moves from the GW handpiece into stagnant fluids in the pulp chamber, the shear forces trigger hydrodynamic cavitation, and cavitation clouds are formed. The implosion of these microbubbles generates sound waves that reverberate via the root canal. The handpiece has a 5-point vented suction system to collect excess irrigant from the pulp chamber [12].
The recommended protocol involves 3% NaOCl irrigant activation for three or five minutes, subsequently irrigated with water for 15 or 30 seconds, 8% EDTA for two minutes, and finally distilled water rinse for 15 or 30 seconds [12]. In Alquria et al.'s study [8], 17% EDTA is used. The interplay of multisonic energy, vortical fluid dynamics, and irrigant chemistry is believed to enhance the removal of organic debris from the root canal system [12]. This could have possibly been attributed to the leverage in disinfection as seen in the studies of Zhang et al. [7] and Alquria et al. (2022) [8].
GWS handpiece dispenses irrigants at a high-speed shear force of about 45 ml/min flow rate. Thus 180 ml of NaOCl and a total volume of 270 ml irrigants are utilized. Matching this irrigant volume in an ultrasonic system by increasing the activation time increases the risk of ultrasonic tip separation, ledge, and uncontrolled dentin removal. Despite the different mechanisms of action, bacterial reduction was similar in both GWS and ultrasonic activation groups in the study by Llerena et al. [5].
From this review, it can be noted that ultrasonic irrigant activation is on par with GWS in biofilm removal and is feasible. At the same time, GWS is highly effective in simultaneous irrigant activation in all the canals, thereby reducing the chairside time for disinfection though it requires a minimum time to build a platform at the cavosurface before beginning the endodontic disinfection. More importantly, maintenance issues and monitoring the long disinfection cycle of the entire GW console do not surface when it comes to ultrasonic units. Thus, GWS requires a brief learning curve to endorse it into routine clinical practice [12]. Future in vivo studies can deal with the skepticism regarding postoperative pain and hemorrhagic episodes following multisonic activation.
This review provides a good starting point to advocate for a customized irrigant activation protocol based on the microbiome and anatomy of the root canal system in each patient. In conjunction with an overly simplified bacterial killing and biofilm elimination approach with different irrigants and activation methods, future research can focus on a multifaceted strategy deploying targeted antimicrobial peptides to disrupt the EPS matrix, suppress the virulence factors and stress-associated bacterial genes, and kill dormant and persistent cells.
Highlights
Multisonic irrigant activation displayed similar efficacy in biofilm removal when compared to ultrasonic irrigant activation. Volume and duration of irrigant usage are inherently different in both GWS and ultrasonic activation, which influences biofilm removal. GWS is highly effective in simultaneous irrigant activation in all the canals, thereby reducing the duration of disinfection.
Conclusions
Multisonic irrigant activation demonstrated similar efficacy in reducing the biofilm when compared to ultrasonic irrigant activation. However, the multisonic system proved to be advantageous in reducing chairside time because of the simultaneous irrigant activation in all the canals. Future in vivo studies should focus on case-specific irrigation protocol by incorporating knowledge from chemistry, microbiology, and fluid dynamics.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Community as the unit of pathogenicity: an emerging concept as to the microbial pathogenesis of apical periodontitis Oral Surg Oral Med Oral Pathol Oral Radiol Endod Siqueira JF Jr Rôças IN 87087810720091946466010.1016/j.tripleo.2009.01.044 · doi ↗ · pubmed ↗
- 2Biofilms and apical periodontitis: study of prevalence and association with clinical and histopathologic findings J Endod Ricucci D Siqueira JF Jr 127712883620102064708110.1016/j.joen.2010.04.007 · doi ↗ · pubmed ↗
- 3Passive ultrasonic irrigation of the root canal: a review of the literature Int Endod J van der Sluis LW Versluis M Wu MK Wesselink PR 4154264020071744201710.1111/j.1365-2591.2007.01243.x · doi ↗ · pubmed ↗
- 4Chemical and mechanical influence of root canal irrigation on biofilm removal from lateral morphological features of simulated root canals, dentine discs and dentinal tubules Int Endod J Pereira TC Dijkstra RJ Petridis X Sharma PK van de Meer WJ van der Sluis LW de Andrade FB 1121295420213288098910.1111/iej.13399 PMC 7839520 · doi ↗ · pubmed ↗
- 5Multispecies biofilm removal by a multisonic irrigation system in mandibular molars Int Endod J Coaguila-Llerena H Ordinola-Zapata R Staley C Dietz M Chen R Faria G 125212615520223597610110.1111/iej.13813 PMC 9561058 · doi ↗ · pubmed ↗
- 6Comparison of Gentle Wave system and passive ultrasonic irrigation with minimally invasive and conventional instrumentation against LPS in infected root canals Sci Rep Velardi JP Alquria TA Alfirdous RA 48941220223531836510.1038/s 41598-022-08835-4PMC 8940914 · doi ↗ · pubmed ↗
- 7In vitro evaluation by quantitative real-time PCR and culturing of the effectiveness of disinfection of multispecies biofilms in root canals by two irrigation systems Clin Oral Investig Zhang D Shen Y de la Fuente-Núñez C Haapasalo M 91392023201910.1007/s 00784-018-2515-x 29948281 · doi ↗ · pubmed ↗
- 8Comparison of conventional and contemporary root canal disinfection protocols against bacteria, lipoteichoic acid (LTA), and lipopolysaccharide (LPS)Sci Rep Alquria TA Alfirdous RA Gupta S 12061320233668170210.1038/s 41598-022-26855-y PMC 9867776 · doi ↗ · pubmed ↗