Determinants associated with receiving a medical appointment through the primary care access points for unattached adults in Quebec: A cross-sectional study
Mylaine Breton, Catherine Lamoureux-Lamarche, Véronique Deslauriers, Djamal Berbiche, Maude Laberge, Mélanie Ann Smithman, Annie Talbot, Isabelle Gaboury, Marie-Pascale Pomey, Marie Beauséjour

TL;DR
This study explores factors influencing whether unattached adults in Quebec receive medical appointments through primary care access points.
Contribution
This is the first study to document the characteristics and needs of patients using primary care access points in Quebec.
Findings
Younger patients and those with acute health problems are more likely to receive medical appointments through the access points.
Patients seeking medication renewal or administrative help also have a higher likelihood of receiving appointments.
GAP A users are more likely to receive appointments compared to GAP B users.
Abstract
Canada is experiencing an unprecedented primary care crisis, with 6.5 million Canadians reporting lacking a family physician, including 31% of the Quebec population. To address this problem, the province of Quebec implemented primary care access points (in French, they are Guichets d’accès à la première ligne, or GAPs) to help unattached patients navigate and access primary care services while awaiting attachment. We aimed to examine the determinants associated with unattached patients receiving a medical appointment compared to another service through the GAP. Cross-sectional data (n = 13,291) from two GAPs were collected (June 2022 to March 2023). Multivariable logistic regression was carried out. Being younger, calling for an acute health problem, medication renewal or to have administrative documentation filled, having a physical or mental health problem, and using GAP A (compared…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
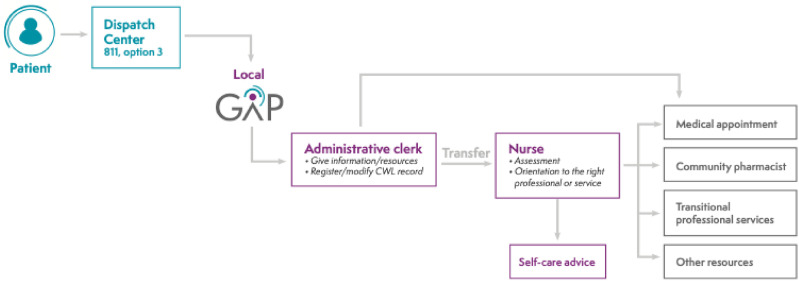 Figure 1
Figure 1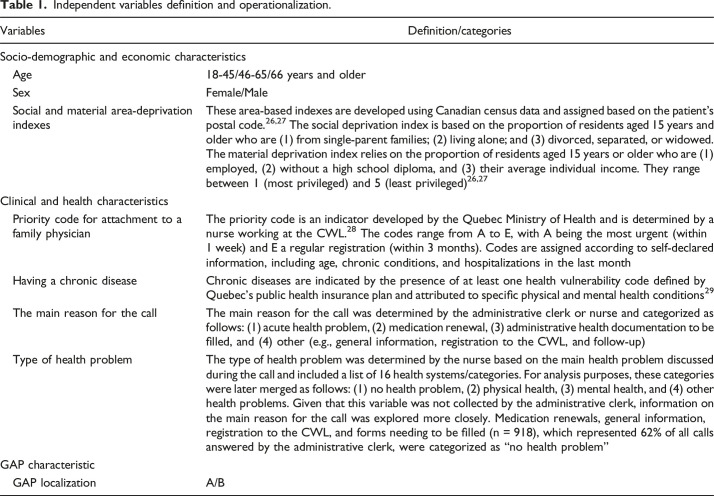 Figure 2
Figure 2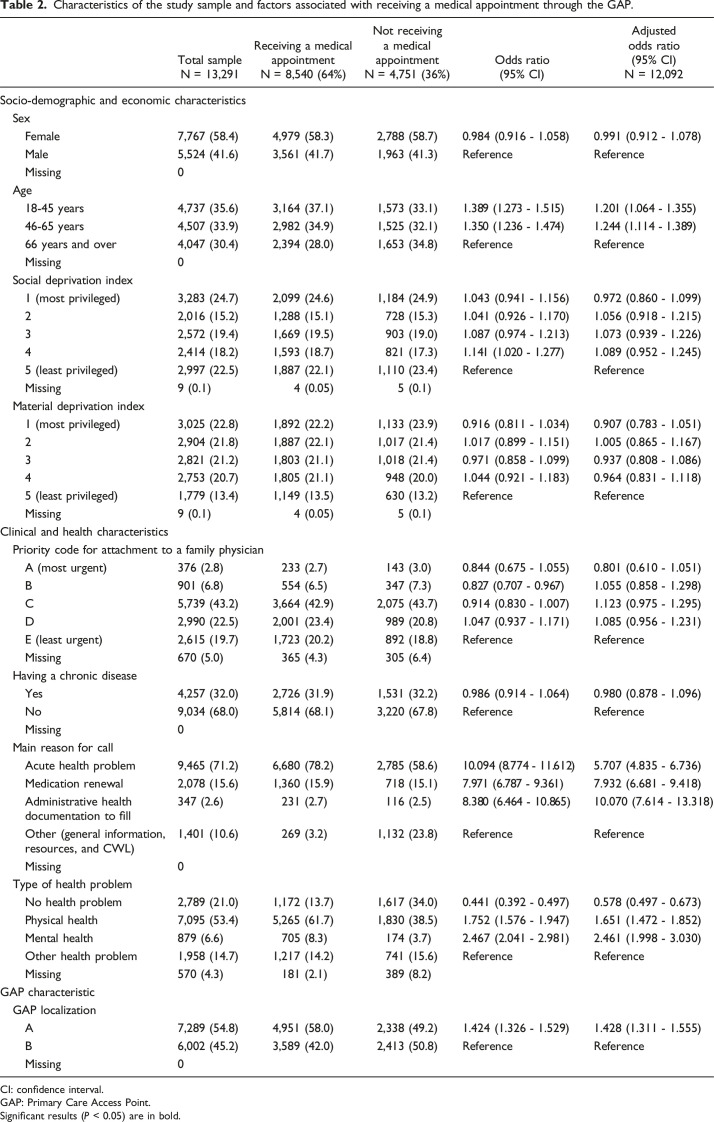 Figure 3
Figure 3- —Fonds de Soutien à l’innovation en santé et services sociaux
- —Canadian Institutes of Health Research
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPrimary Care and Health Outcomes · Healthcare Policy and Management · Patient Satisfaction in Healthcare
Introduction
Canada is experiencing an unprecedented primary care crisis with access challenges at the centre.^1,2^ An estimated 6.5 million Canadians do not have a regular Primary Care Provider (PCP), with the province of Quebec having the highest rate of unattachment (31%).^3,4^ Attachment to a PCP and access to care are key components of high-performing primary care system,^5-7^ contributing to better health outcomes, continuity and coordination of care, and lower emergency department use and healthcare costs.^8-14^ Although access issues in Quebec are not new, they are currently exacerbated by the primary healthcare labour shortage, including increasing numbers of family physicians retiring, vacant family medicine residency positions, and growing numbers of unattached patients.^15-17^
To address this access challenge, over the past 15 years, 8 Canadian provinces, including Quebec, implemented centralized waiting lists (CWLs) for unattached patients.^18,19^ These CWLs are designed to centralize all requests for attachment and match patients with a PCP based on territory, priority criteria and PCP availability.^ 18 ^ As of May 2024, 1.55 million Quebecers (17% of the population) were registered on the CWL awaiting attachment.^20,21^
Although the CWL in Quebec has led to the attachment of over a million patients since its implementation, the number of unattached patients and the waiting time to be attached have continued to rise in the last few years.^22,23^ The Quebec Ministry of Health mandated, in 2022, province-wide implementation of primary care access points (Guichets d’accès à la première ligne; GAP) for unattached patients and incentivized family physicians to offer medical appointments.
The GAP is an organizational innovation, implemented within regions, aiming to help unattached patients navigate and access primary care services while awaiting attachment. It operates on a geographical basis and is linked to the local CWL. Figure 1 details GAP structure and functioning. First, unattached patients call the GAP dispatch centre. If the patient is eligible (i.e., already registered on the CWL), the call is transferred to their local GAP, where an administrative clerk gives information/resources and registers/modifies the patient’s CWL record, if needed. Then, if the patient needs a medical appointment or to be assessed by a nurse, the most appropriate of the following decisions is made based on a decision tree: (1) give a medical appointment without transferring the patient to a registered nurse, (2) transfer the patient to a GAP registered nurse, or (3) add the patient to a waiting list to be called by a GAP nurse. The patient is oriented to the most relevant professional or service according to their need and available professional resources, including a medical appointment with a family physician, referral to a community pharmacist, referral to GAP transitional professional services for patients with unstable chronic diseases, and advice to consult a community resource. This ensures better allocation of scarce medical appointments for patients requiring a family physician. Although the innovation was first piloted in a small region,^ 24 ^ data on its effects and the population using the service are scarce.Figure 1.Primary Care Access Point structure.
Our research team previously examined characteristics of 1,323 unattached paediatric patients using the GAP and associations with the need for a medical appointment.^ 25 ^ We found that being 0-5 years old, being first assessed by a nurse (Info-Health), and calling for medication renewal were associated with an increased likelihood of needing a medical appointment.^ 25 ^ Although this study was the first to document the determinants of needing a medical appointment in unattached GAP patients compared to another service through the GAP, it was limited to the paediatric population (aged <18 years), which has different characteristics and needs than the adult population. Therefore, we aim to examine, in unattached adults, the socio-demographic, economic, and clinical characteristics associated with receiving a medical appointment compared to another service through the GAP. Our study will enable a better understanding of who uses GAP services in order to improve access in case of clinical needs.
Method
This retrospective study was conducted in a region with two local health territories and two GAPs (one per local health territory) with over 78,000 eligible unattached patients. Cross-sectional data were extracted from GAP Electronic Medical Records (EMRs), which includes data collected during the call and from CWL records.
The study sample included all patients aged over 18 years who called the GAP between June 2022 and March 2023. Given that nearly 70% of GAP patients called only once during the study period, and to facilitate data management and analysis, only one call per patient was included in the study. For patients with more than one call, the following strategy was used to identify the included call. For patients who received a medical appointment from the administrative clerk or nurse, the first call during the study period with a medical appointment was considered. For patients who never received a medical appointment, the first call assessed by a registered nurse was prioritized. If no calls were assessed by a registered nurse, the first call answered by the administrative clerk was considered. The study sample was n = 13,291.
Measures
Receiving a medical appointment
Receiving a medical appointment through the GAP was dichotomized (yes/no). Medical appointments are face-to-face consultations with a family physician in a primary care clinic located on the local health territory. Patients who did not have a medical appointment may have received other services or references from the GAP, including self-care advice, general information and referral to GAP transitional professional services, a community pharmacist, another health professional, or a community resource.
Independent variables
Socio-demographic and economic characteristics included age, sex, and social and material area-deprivation indexes.^26,27^ Clinical and health characteristics included priority code for attachment to a family physician, having a chronic disease, main reason for calling and type of health problem. The GAP was categorized as GAP A or GAP B depending on the patient’s address. Each variable’s definition and operationalization are detailed in Table 1.Table 1.Independent variables definition and operationalization.VariablesDefinition/categoriesSocio-demographic and economic characteristics Age18-45/46-65/66 years and older SexFemale/Male Social and material area-deprivation indexesThese area-based indexes are developed using Canadian census data and assigned based on the patient’s postal code.^26,27^ The social deprivation index is based on the proportion of residents aged 15 years and older who are (1) from single-parent families; (2) living alone; and (3) divorced, separated, or widowed. The material deprivation index relies on the proportion of residents aged 15 years or older who are (1) employed, (2) without a high school diploma, and (3) their average individual income. They range between 1 (most privileged) and 5 (least privileged)^26,27^Clinical and health characteristics Priority code for attachment to a family physicianThe priority code is an indicator developed by the Quebec Ministry of Health and is determined by a nurse working at the CWL.^ 28 ^ The codes range from A to E, with A being the most urgent (within 1 week) and E a regular registration (within 3 months). Codes are assigned according to self-declared information, including age, chronic conditions, and hospitalizations in the last month Having a chronic diseaseChronic diseases are indicated by the presence of at least one health vulnerability code defined by Quebec’s public health insurance plan and attributed to specific physical and mental health conditions^ 29 ^ The main reason for the callThe main reason for the call was determined by the administrative clerk or nurse and categorized as follows: (1) acute health problem, (2) medication renewal, (3) administrative health documentation to be filled, and (4) other (e.g., general information, registration to the CWL, and follow-up) Type of health problemThe type of health problem was determined by the nurse based on the main health problem discussed during the call and included a list of 16 health systems/categories. For analysis purposes, these categories were later merged as follows: (1) no health problem, (2) physical health, (3) mental health, and (4) other health problems. Given that this variable was not collected by the administrative clerk, information on the main reason for the call was explored more closely. Medication renewals, general information, registration to the CWL, and forms needing to be filled (n = 918), which represented 62% of all calls answered by the administrative clerk, were categorized as “no health problem”GAP characteristic GAP localizationA/B
Analysis
Descriptive analysis was conducted to describe the study sample. Bivariate and multivariable binomial logistic regressions were used to assess the socio-demographic, economic, and clinical factors as well as the GAP-related characteristic associated with receiving a medical appointment. Adjusted Odds Ratios (AORs) are presented with 95% Confidence Intervals (CIs). Statistical analyses were carried out using SPSS V29.0 and SAS V9.4.
Results
The study sample was mostly female (58.4%) with a mean age of 53.7 years. Over 50% of the sample was considered vulnerable based on their priority code (codes A, B, and C), and 32% had at least one chronic disease. The main reason for calling was an acute health problem (71%), whereas physical and mental health problems represented 53% and 7% of cases, respectively. GAP A received 55% of requests. A total of 64% of the sample received a medical appointment.
Table 2 presents bivariate logistic regression models. Age, social deprivation index, priority code for attachment to a family physician, main reason for calling, type of health problem, and GAP localization were associated with receiving a medical appointment.Table 2.Characteristics of the study sample and factors associated with receiving a medical appointment through the GAP.Total sample N = 13,291Receiving a medical appointment N = 8,540 (64%)Not receiving a medical appointment N = 4,751 (36%)Odds ratio (95% CI)Adjusted odds ratio (95% CI) N = 12,092Socio-demographic and economic characteristics Sex Female7,767 (58.4)4,979 (58.3)2,788 (58.7)0.984 (0.916 - 1.058)0.991 (0.912 - 1.078) Male5,524 (41.6)3,561 (41.7)1,963 (41.3)ReferenceReference Missing0 Age 18-45 years4,737 (35.6)3,164 (37.1)1,573 (33.1)1.389 (1.273 - 1.515)1.201 (1.064 - 1.355) 46-65 years4,507 (33.9)2,982 (34.9)1,525 (32.1)1.350 (1.236 - 1.474)1.244 (1.114 - 1.389) 66 years and over4,047 (30.4)2,394 (28.0)1,653 (34.8)ReferenceReference Missing0 Social deprivation index 1 (most privileged)3,283 (24.7)2,099 (24.6)1,184 (24.9)1.043 (0.941 - 1.156)0.972 (0.860 - 1.099) 22,016 (15.2)1,288 (15.1)728 (15.3)1.041 (0.926 - 1.170)1.056 (0.918 - 1.215) 32,572 (19.4)1,669 (19.5)903 (19.0)1.087 (0.974 - 1.213)1.073 (0.939 - 1.226) 42,414 (18.2)1,593 (18.7)821 (17.3)1.141 (1.020 - 1.277)1.089 (0.952 - 1.245) 5 (least privileged)2,997 (22.5)1,887 (22.1)1,110 (23.4)ReferenceReference Missing9 (0.1)4 (0.05)5 (0.1) Material deprivation index 1 (most privileged)3,025 (22.8)1,892 (22.2)1,133 (23.9)0.916 (0.811 - 1.034)0.907 (0.783 - 1.051) 22,904 (21.8)1,887 (22.1)1,017 (21.4)1.017 (0.899 - 1.151)1.005 (0.865 - 1.167) 32,821 (21.2)1,803 (21.1)1,018 (21.4)0.971 (0.858 - 1.099)0.937 (0.808 - 1.086) 42,753 (20.7)1,805 (21.1)948 (20.0)1.044 (0.921 - 1.183)0.964 (0.831 - 1.118) 5 (least privileged)1,779 (13.4)1,149 (13.5)630 (13.2)ReferenceReference Missing9 (0.1)4 (0.05)5 (0.1)Clinical and health characteristics Priority code for attachment to a family physician A (most urgent)376 (2.8)233 (2.7)143 (3.0)0.844 (0.675 - 1.055)0.801 (0.610 - 1.051) B901 (6.8)554 (6.5)347 (7.3)0.827 (0.707 - 0.967)1.055 (0.858 - 1.298) C5,739 (43.2)3,664 (42.9)2,075 (43.7)0.914 (0.830 - 1.007)1.123 (0.975 - 1.295) D2,990 (22.5)2,001 (23.4)989 (20.8)1.047 (0.937 - 1.171)1.085 (0.956 - 1.231) E (least urgent)2,615 (19.7)1,723 (20.2)892 (18.8)ReferenceReference Missing670 (5.0)365 (4.3)305 (6.4) Having a chronic disease Yes4,257 (32.0)2,726 (31.9)1,531 (32.2)0.986 (0.914 - 1.064)0.980 (0.878 - 1.096) No9,034 (68.0)5,814 (68.1)3,220 (67.8)ReferenceReference Missing0 Main reason for call Acute health problem9,465 (71.2)6,680 (78.2)2,785 (58.6)10.094 (8.774 - 11.612)5.707 (4.835 - 6.736) Medication renewal2,078 (15.6)1,360 (15.9)718 (15.1)7.971 (6.787 - 9.361)7.932 (6.681 - 9.418) Administrative health documentation to fill347 (2.6)231 (2.7)116 (2.5)8.380 (6.464 - 10.865)10.070 (7.614 - 13.318) Other (general information, resources, and CWL)1,401 (10.6)269 (3.2)1,132 (23.8)ReferenceReference Missing0 Type of health problem No health problem2,789 (21.0)1,172 (13.7)1,617 (34.0)0.441 (0.392 - 0.497)0.578 (0.497 - 0.673) Physical health7,095 (53.4)5,265 (61.7)1,830 (38.5)1.752 (1.576 - 1.947)1.651 (1.472 - 1.852) Mental health879 (6.6)705 (8.3)174 (3.7)2.467 (2.041 - 2.981)2.461 (1.998 - 3.030) Other health problem1,958 (14.7)1,217 (14.2)741 (15.6)ReferenceReference Missing570 (4.3)181 (2.1)389 (8.2)GAP characteristic GAP localization A7,289 (54.8)4,951 (58.0)2,338 (49.2)1.424 (1.326 - 1.529)1.428 (1.311 - 1.555) B6,002 (45.2)3,589 (42.0)2,413 (50.8)ReferenceReference Missing0CI: confidence interval.GAP: Primary Care Access Point.Significant results (P < 0.05) are in bold.
Table 2 presents multivariable logistic regression models. Younger patients (≤65 years) were more likely to receive a medical appointment than older adults. Patients calling for acute health problems (AOR: 5.707, 95% CI: 4.835-6.736), medication renewals (AOR: 7.932, 95% CI: 6.681-9.418), or to have administrative health documentation filled (AOR: 10.070, 95% CI: 7.614-13.318) were more likely to receive an appointment than patients calling for another reason. Compared to other health problems, patients with a physical (AOR: 1.651, 95% CI: 1.472-1.852) or mental health problem (AOR: 2.461, 95% CI: 1.998-3.030) were more likely to receive an appointment, whereas those without a health problem (AOR: 0.578, 95% CI: 0.497-0.673) were less likely. Patients who received services from GAP A were more likely to receive a medical appointment (AOR: 1.428, 95% CI: 1.311-1.555).
Discussion
Building on a unique clinical-administrative dataset, this paper examined the socio-demographic, economic, and clinical characteristics of unattached adult patients and one GAP characteristic associated with receiving a medical appointment through the GAP. Results revealed that younger patients, those calling for acute health problems, medication renewals, or to have an administrative health form filled and those with physical or mental health problems were significantly more likely to receive medical appointments through the GAP. Additionally, patients from GAP A (vs. B) had higher odds of receiving a medical appointment. These findings are valuable to better understand the characteristics of individuals who use GAP services to improve the appropriate use of scarce healthcare resources in Quebec.
Differences related to patient age
Patients aged 18-65 were more likely to receive a medical appointment than older adults (≥66 years). Although health does not change linearly and equally in older adults, this result seems counter-intuitive given that physical health problems, chronic illnesses, and cognitive impairments requiring medical follow-up are more prevalent in this population.^30-33^ In fact, older adults in our study were more likely to have a chronic disorder and be considered vulnerable (priority code A, B, or C). A possible explanation is that the GAP was mainly designed to address acute health problems, and more complex needs requiring follow-up care (multiple chronic disorders, polypharmacy, home care, etc.) might not fit well in this model. These hypotheses are supported by data (not shown) indicating that older adults’ requests more likely resulted in orientation to GAP transitional professional services for unstable chronic illnesses and home care support. The interaction between age and main reason for calling was also significant. In fact, younger adults were more likely to receive a medical appointment than older adults with the same reason for calling. Although the GAP has improved access to primary care services in Quebec, it might not be suitable for older adults with chronic conditions requiring follow-up care and raises questions about lack of relational continuity. Therefore, efforts are needed to ensure the GAP and its complementary services (e.g., transitional professional services) respond to the needs of older unattached patients, which represented 30% of our study sample. Also, younger people might wait longer before calling the GAP, leading to worse health problems that more likely necessitate a medical appointment. Work schedules can leave little room for calling the GAP, which can take several hours before being assessed by a nurse. Conversely, older adults might have more time to call or be curious about the service’s mission or functioning. After the study period, in fall 2023, a digital GAP (https://gap.soinsvirtuels.gouv.qc.ca/en)—an on-line platform where patients can fill a request regarding their health need—was implemented province-wide to reduce phone wait times and standardize GAP processes and trajectories. This solution will likely increase access to GAP services for all age groups and occupations.
Variable medical capacity across GAPs
Patients calling GAP A were more likely to receive a medical appointment than patients calling GAP B. One possible explanation is differences in medical appointment availability for GAP patients. In fact, the characteristics of the local health territories showed that no medical appointment was available in 0.8% of cases in GAP A compared to 11.4% in GAP B. Within the GAP A territory, a medical clinic opened a site with a large appointment capacity especially for GAP patients. This might have led to patients that could have been seen by another health professional being granted a medical appointment, suggesting that available resources influence the orientation of GAP patients. In the GAP context, the responsibility for caring for unattached patients and the allocation of appointments to these patients has always relied on the voluntary participation of clinics and family physicians, which creates territorial inequalities in access. A recent provincial report highlighted territorial differences in terms of available medical appointments for GAP patients impacting the capacity of GAPs to respond to local needs.^ 34 ^ Indeed, in our study, 6% of GAP A patients who needed an appointment did not receive one, compared to 14% in GAP B.
Main reasons for receiving a medical appointment
Our findings showed that acute health problems, medication renewals, and filling an administrative health form were associated with a greater likelihood of receiving a medical appointment. Similarly, Bergeron et al. showed that acute health problems and medication renewals were determinants of needing a medical appointment in paediatric patients.^ 25 ^ In Quebec, the scope of practice of community pharmacists was recently extended to increase flexibility and autonomy to initiate and modify medications and renew prescriptions.^ 35 ^ This new legislation seems particularly beneficial for unattached patients given that community pharmacists are easy to access.^ 36 ^ As part of the GAP, efforts were made in the region under study to collaborate with community pharmacists and orient patients to these services when appropriate.^ 37 ^ Thus, our finding regarding the increased likelihood of receiving a medical appointment for medication renewals may be surprising. However, community pharmacists cannot renew prescriptions beyond 12 months.^ 35 ^ Further, community pharmacists’ scope of practice was expanded around the same time as the GAP and involved important practice changes that could take time to implement. Sustained efforts are needed to support and collaborate with community pharmacists to maximize the use of their expertise and increase their role in patient care.
In Quebec, many administrative health forms, including from the Quebec Automobile Insurance Society, the Quebec Labour Standards Commission, private insurers, and employers, must be signed by a physician. Indeed, patients needing a form filled were ten times more likely to receive a medical appointment. This is worrying given the physician shortage and their increased administrative workload, which limits time for patient care. To tackle this issue, Quebec’s Ministry of Health recently started revising health administrative forms needing to be filled by physicians.^ 38 ^
Strengths and limitations
This study is the first to document the characteristics of adult GAP patients and the determinants of receiving a medical appointment through the GAP. Data were extracted retrospectively from EMR, and the reliability of administrative data for research purposes remains a challenge. Although the study was conducted in only one region, it included a large population of patients who called the GAP during the study period.
Given that data were not collected for research and information collected varied during the study period, multiple information was considered to determine if patients received an appointment. For ease of analysis, only one call per patient was considered. When identifying the call to include, we prioritized that which resulted in a medical appointment given that for the same health problem, a call can lead to a medical appointment up to several weeks later. This might have overestimated the associations given that appointments were more likely received during retained than excluded calls. However, this potential bias might be limited given that 67% of the sample called only once during the study period. As part of this study, we were not able to capture patient outcomes related to GAP service received such as patient satisfaction and ER visits. However, in the next part of our larger study, we will assess, through a self-reported survey, the patient experience associated with GAP services received including unmet healthcare needs, ER consultations and healthcare services that patients would have used if the GAP did not exist. This will inform whether GAP service trajectories (medical appointment, referral to community pharmacist and other professionals, orientation to emergency department) are meeting patients’ needs.
Conclusion
This is the first study to document the characteristics of patients using the GAP, an organizational innovation aiming to facilitate unattached patients’ navigation and access to primary care in Quebec. The findings can inform on the characteristics of patients with potential needs not being meet by the GAP in order to improve care trajectories. In addition to providing a socio-demographic portrait of patients receiving medical appointments through the GAP, the findings highlighted the reason of consultations for which unattached patients received medical appointments. Together, this information could support the development and improvement of care trajectories (e.g., filling administrative forms and medication renewal) and thus, make better use of scarce human and financial resources in primary healthcare systems. Future studies on patient-reported experience measures are needed to better understand if GAP services are meeting unattached patient needs.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Duong D . Primary care is facing a capacity crisis — can pandemic lessons help chart a path forward? CMAJ (Can Med Assoc J). 2022;194(43):E 1488. doi:10.1503/cmaj.109602336343948 PMC 9828995 · doi ↗ · pubmed ↗
- 2Flood CM Thomas B Mc Gibbon E . Canada’s primary care crisis: federal government response. Healthc Manag Forum. 2023;36(5):327-332. doi:10.1177/08404704231183863 PMC 1044829637424188 · doi ↗ · pubmed ↗
- 3Duong D Vogel L . National survey highlights worsening primary care access. CMAJ (Can Med Assoc J). 2023;195(16):E 592-E 593. doi:10.1503/cmaj.109604937094873 PMC 10125184 · doi ↗ · pubmed ↗
- 4Kiran T Daneshvarfard M Wang R , et al. Public experiences and perspectives of primary care in Canada: results from a cross-sectional survey. CMAJ (Can Med Assoc J). 2024;196(19):E 646-E 656. doi:10.1503/cmaj.23137238772606 PMC 11104576 · doi ↗ · pubmed ↗
- 5Aggarwal M Hutchison B Abdelhalim R Baker GR . Building high-performing primary care systems: after a decade of policy change, is Canada “walking the talk?”. Milbank Q. 2023;101(4):1139-1190. doi:10.1111/1468-0009.1267437743824 PMC 10726918 · doi ↗ · pubmed ↗
- 6Hutchison B Levesque JF Strumpf E Coyle N . Primary health care in Canada: systems in motion. Milbank Q. 2011;89(2):256-288. doi:10.1111/j.1468-0009.2011.00628.x 21676023 PMC 3142339 · doi ↗ · pubmed ↗
- 7Bodenheimer T Ghorob A Willard-Grace R Grumbach K . The 10 building blocks of high-performing primary care. Ann Fam Med. 2014;12(2):166-171. doi:10.1370/afm.161624615313 PMC 3948764 · doi ↗ · pubmed ↗
- 8Starfield B Shi L . The medical home, access to care, and insurance: a review of evidence. Pediatrics. 2004;113(Supplement_4):1493-1498. doi:10.1542/peds.113.S 4.149315121917 · doi ↗ · pubmed ↗