Endoscopic management of gastric band erosion using argon plasma coagulation
Emmanuel Palomera-Tejeda, Kalpesh Patel, Farid Abushamat, Salmaan Jawaid

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
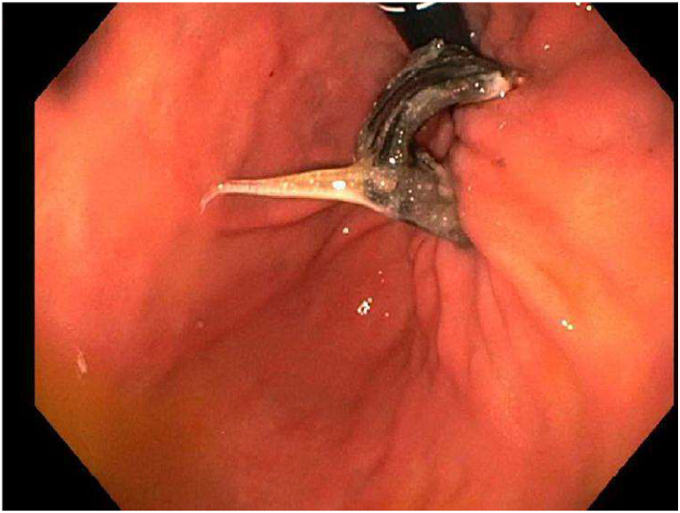 Figure 1
Figure 1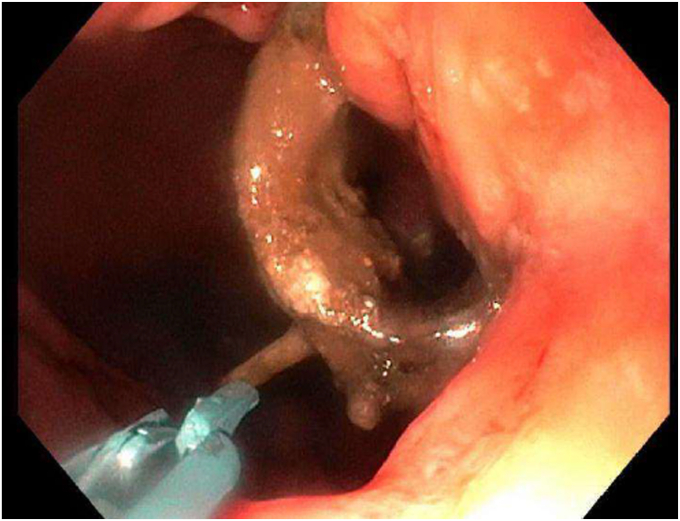 Figure 2
Figure 2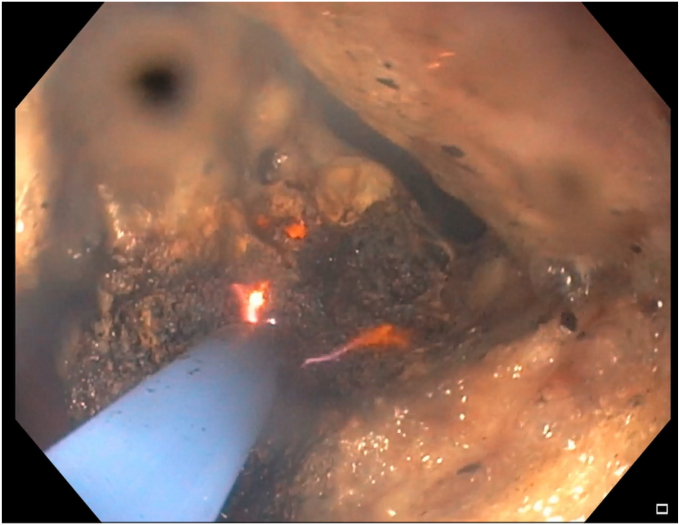 Figure 3
Figure 3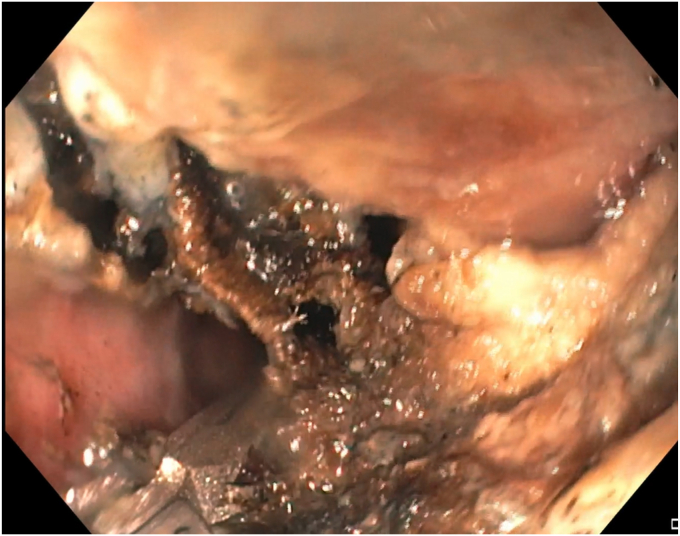 Figure 4
Figure 4 Figure 5
Figure 5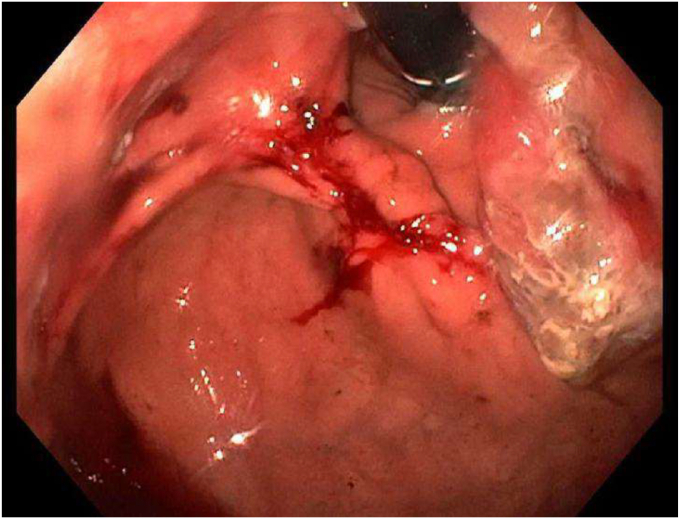 Figure 6
Figure 6Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsBariatric Surgery and Outcomes · Esophageal and GI Pathology · Gastroesophageal reflux and treatments
Gastric banding emerged as one of the first bariatric procedures; however, its use has significantly decreased in favor of more modern interventions.1, 2, 3 Gastric banding accounted for less than 1% of total bariatric interventions in the United States in 2019, compared with 35.4% in 2011.1 This decline is primarily the result of limited weight loss and a high rate of adverse events, such as gastric band erosion (GBE). GBE is a rare but well-known and dangerous adverse event in which the band erodes into the stomach and may further migrate, causing biliary or bowel obstruction.2 The management of GBE involves band removal, which can be performed using an endoscopic and/or surgical approach. However, an initial endoscopic approach is preferred to monitor for adverse events in real time, as the external aspect of the band usually is encapsulated in fibrosis, and a laparoscopic approach carries a risk of inadvertent gastric perforation.3, 4, 5
Aim
The objective of this video case report is to demonstrate the use of argon plasma coagulation (APC) to facilitate the endoscopic removal of an eroded gastric band.
Case report
A 68-year-old woman presented for evaluation of gastric band removal. She had the band placed approximately 30 years previously, with an initial rapid loss of 70 lbs reported. Over time, she experienced chronic abdominal discomfort and intermittent nausea and vomiting, with recent worsening symptoms. Previous investigations included an EGD with a reported eroded band. She was referred to our medical center for further management and was scheduled for an index EGD with possible band removal.
Procedure
During the EGD (GIF-HQ190; Olympus Corp, Center Valley, Pa, USA), an eroded lap band, 75% exposed, was found in the gastric fundus (Fig. 1 and Video 1, available online at www.videogie.org). An endoscopic knife (SB knife; Olympus Corp) was used as an initial attempt to sever the band, but progress was slow (Fig. 2). To minimize tissue manipulation of the already damaged gastric mucosa, forced APC at 100 W using straight-fire axial beam (VIO 3; Erbe USA, Marietta, Ga, USA) was applied to the band to facilitate transection (Fig. 3), with a total APC duration of 3.5 minutes. Complete separation from the gastric wall and retrieval of the transected band (Figs. 4 and 5) were successfully accomplished with a foreign body–grasping forceps (Raptor; Steris, Mentor, Ohio, USA).Figure 1. Migrated gastric band with 75% of its circumference eroding into the stomach fundus.Figure 2. Initial transection attempt using an endoscopic knife.Figure 3. Application of argon plasma coagulation to facilitate the transection of the band.Figure 4. Final separation from the gastric wall using a Raptor grasping device.Figure 5. Transected gastric band after retrieval.
Outcome
The patient's course was satisfactory (Fig. 6), and she was discharged on the same day as the procedure. She continued follow-up with the bariatric service for further management of the subcutaneous port, and her symptoms had already improved by her next visit.Figure 6. Gastric fundus after endoscopic band removal.
Conclusions
In conclusion, gastric band migration is a rare but still-encountered adverse event of gastric banding. Prompt removal of the eroded band is essential to prevent further adverse events. Endoscopic removal can be achieved using various endoscopic tools; however, it can be quite challenging because of the resistance of the band. In this video case report, we demonstrate the feasibility of using APC to facilitate the endoscopic transection of an eroded band and potentially reduce the risk of intraprocedural adverse events. Although APC is a useful adjunctive tool that is easy to operate and widely available, its success is not guaranteed and may necessitate additional removal techniques. Effective alternatives include endoscopic scissors and mechanical lithotripters with guidewire assistance.3^,^5
Patient Consent
The patient in this article has given informed consent to publication of the case details.
Disclosure
All authors disclosed no financial relationships.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1American Society for Metabolic and Bariatric Surgery Estimate of bariatric surgery numbers Available at:https://asmbs.org/resources/estimate-of-bariatric-surgery-numbers
- 2Nasser H.Ivanics T.Leonard-Murali S.A case report of an adjustable gastric band erosion and migration into the jejunum resulting in biliary obstruction Int J Surg Case Rep 6420191391423165528310.1016/j.ijscr.2019.10.025PMC 6818341 · doi ↗ · pubmed ↗
- 3Spann M.D.Aher C.V.English W.J.Endoscopic management of erosion after banded bariatric procedures Surg Obes Relat Dis 132017187518792887076010.1016/j.soard.2017.07.025 · doi ↗ · pubmed ↗
- 4Manos T.Nedelcu A.Noel P.Endoscopic gastric band removal J Clin Med 1220236173667554810.3390/jcm 12020617 PMC 9867319 · doi ↗ · pubmed ↗
- 5Hanscom M.Sayegh L.Sharma I.Endoscopic removal of 2 types of eroded gastric bands using endoscopic scissors Video GIE 920242712733888773210.1016/j.vgie.2024.03.005PMC 11180373 · doi ↗ · pubmed ↗