Effect of a Single Preventive Intravenous Dose of Ketorolac and Paracetamol on Reducing Postoperative Pain in Septorhinoplasty Patients: Double-Blind Randomized Clinical Trial
Laleh Dehghanpisheh, Fatane Jamshidi, Saeid Khademi, Shirin Farokhiani, Mohammad Reza Cheraghi, Mahsa Emadi, Reza Kaboodkhani, Ali Akbari, Naeimehossadat Asmarian, Mahsa Banifatemi

TL;DR
This study found that a single dose of IV paracetamol or ketorolac before surgery reduced postoperative pain in septorhinoplasty patients compared to a placebo.
Contribution
The study demonstrates that IV paracetamol is a viable alternative to ketorolac for postoperative pain management in septorhinoplasty.
Findings
Both ketorolac and paracetamol significantly reduced pain scores compared to placebo one hour post-surgery.
The need for rescue analgesic pethidine hydrochloride was significantly lower in the treatment groups.
Paracetamol and ketorolac showed similar efficacy in pain reduction after septorhinoplasty.
Abstract
Effective pain management is crucial in septorhinoplasty and remains a significant challenge. This study investigated the effect of ketorolac and paracetamol on pain control in septorhinoplasty patients and assessed their efficacy in reducing the need for rescue analgesics. This double-blind randomized clinical trial was conducted at Madar-Koodak Hospital (Shiraz, Iran), in 2022. Ninety-nine patients were randomly assigned to three groups to receive ketorolac 30 mg (n=33), paracetamol 1000 mg (n=33), and normal saline (n=33), respectively. All the medications were administered intravenously (IV) 30 min before surgery. The randomization procedure followed the block randomization method. If the pain did not subside, patients were also given a single dose of pethidine hydrochloride (25 mg). Pain intensity was measured using visual analog scale (VAS) 1 hour and 6 hours after surgery. The…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
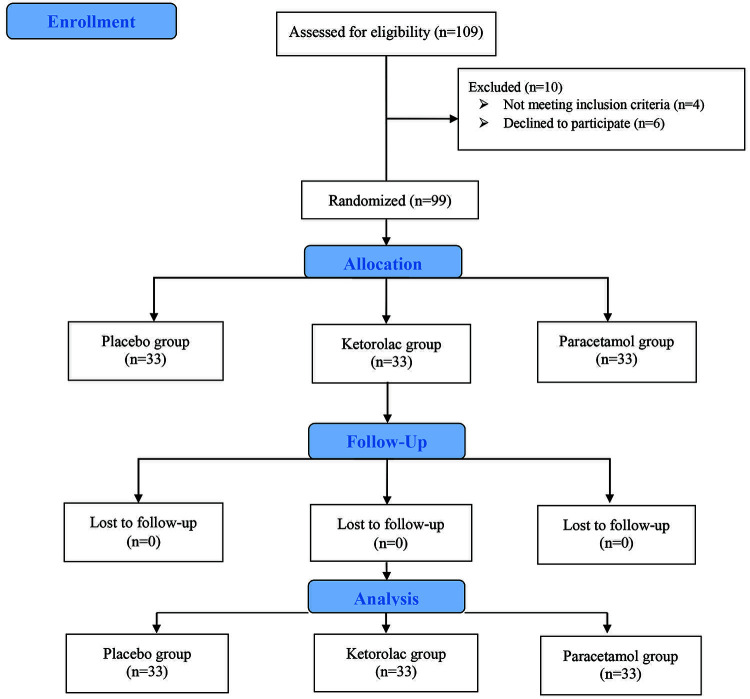 Figure 1
Figure 1| Variables | Ketorolac (n=33) | Paracetamol (n=33) | Placebo (n=33) | P value | |
|---|---|---|---|---|---|
| Age | 27.12±7.01 | 31.21±7.52 | 30.42±7.21 | 0.057 | |
| Sex | Male | 5 (15.2) | 8 (24.2) | 4 (12.1) | 0.397 |
| Female | 28 (84.8) | 25 (75.8) | 29 (87.9) | ||
| Ketorolac (n=33) | Paracetamol (n=33) | Placebo (n=33) | P value between groups | Mean Difference (95% CI) (Ketorolac-Placebo) | Mean Difference (95% CI) (Paracetamol-Placebo) | |
|---|---|---|---|---|---|---|
| VAS 1 hour | 2.87±0.78 | 2.67±0.64 | 3.45±0.71 | <0.001 | -0.57 (-0.94, -0.21) | -0.79 (-1.12, -0.45) |
| VAS 6 hours | 2.82±0.73 | 2.57±0.79 | 2.61±0.83 | 0.394 | 0.21 (-0.17, 0.59) | -0.03 (-0.43, 0.37) |
| P value within group | 0.160 | 0.263 | <0.001* |
| Variable | Ketorolac (n=33) | Paracetamol (n=33) | Placebo (n=33) | P value |
|---|---|---|---|---|
| Number of pethidine (dose 25) | 1 (3) | 0 (0) | 19 (57.6) | <0.001 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsInflammatory mediators and NSAID effects · Olfactory and Sensory Function Studies · Anesthesia and Sedative Agents
What’s Known
- Septorhinoplasty frequently causes severe postoperative pain, demanding effective pain management strategies.
- Preventive analgesia can help reduce postoperative pain and opioid reliance in septorhinoplasty patients.
What’s New
- While non-steroidal anti-inflammatory medicines are known for preventive analgesia in some surgeries, no previous study has specifically evaluated ketorolac for septorhinoplasty and compared its effect with paracetamol.
- Patients who received these preemptive analgesics required almost no rescue opioids, indicating that they had the potential to reduce opioid dependency in septorhinoplasty patients.
Introduction
Septorhinoplasty, a combined surgical procedure, that includes rhinoplasty for aesthetic enhancements and septoplasty for airway canal improvement, is a prevalent intervention worldwide. ^ 1 ^ This procedure often causes significant postoperative pain for patients, particularly in the first 3 days. ^ 2 ^ Effective postoperative pain management is essential for patient care. Sufficient pain relief decreases morbidity, complications, and length of hospital stay while also contributing to cost-effective healthcare. ^ 3 ^ Pain control after rhinoplasty is associated with higher patient satisfaction and perceived surgical outcomes. ^ 4 ^ Acute pain management proves invaluable, considering the distinct characteristics of pain and the nature of diverse surgical procedures. ^ 5 ^
Although the advantages of effective postoperative pain management are widely acknowledged, developing a personalized strategy for pain control in the context of rhinoplasty remains a challenge. ^ 6 , 7 ^ Several clinical guidelines have been published to address this gap, aiming to assist physicians in providing optimal care for subsiding postoperative pain. ^ 3 , 8 ^ One commonly used medication in these conditions is opioids. With the availability of longer-acting opioids, misuse and overdose-related deaths are increasing. ^ 9 ^
There is a significant gap in pain management guidelines, especially in the field of plastic surgery, due to the heterogeneity in postoperative pain levels and the distinct impact of analgesics on different surgical procedures. Although rhinoplasty, with or without septoplasty, is one of the most routine plastic surgery interventions, the available data on effective pain reduction strategies following nose surgery remains insufficient. ^ 10 ^ Guidelines do not offer specific recommendations for pain management following head and neck surgeries, such as septorhinoplasty and rhinoplasty. ^ 11 ^
Preventive pain reduction is a therapeutic approach applied before tissue injury to minimize the activation of the peripheral and central nervous system. ^ 12 ^ This method aims to reduce nervous system activation, which lowers postoperative pain. ^ 13 ^ In a systematic review, it was indicated that cyclooxygenase-2 (COX-2) inhibitors and gabapentin were the most effective preventive analgesics for postoperative pain. ^ 14 ^ In this way, this study aimed to compare the effectiveness of a single intravenous (IV) dose of ketorolac versus paracetamol in reducing postoperative pain and rescue analgesic requirements for patients who underwent septorhinoplasty.
Patients and Methods
This single-center randomized, double-blind, clinical trial was registered in the Iranian Registry of Clinical Trials (IRCT20180922041084N6) and conducted in the Madar-Koodak Hospital, affiliated with Shiraz University of Medical Sciences (Shiraz, Iran), in 2022. The study protocol was approved by the Ethics Committee of Shiraz University of Medical Sciences (IR.SUMS.MED.REC.1400.603) and conformed to the ethical guidelines of the Declaration of Helsinki (1975). All patients provided written informed consent before their enrollment.
Sampling and Study Population
This randomized, double-blind, clinical trial enrolled 99 patients classified as American Society of Anesthesiologists (ASA) physical status I or II, aged between 18 and 50 years, who were candidates for elective septorhinoplasty surgery at Madar-Koodak Hospital, affiliated with Shiraz University of Medical Sciences (Shiraz, Iran). The exclusion criteria included allergic reaction to ketorolac or paracetamol, history of prolonged use of opioids and non-steroidal anti-inflammatory drugs (NSAIDs) consumption, previous occurrence of gastrointestinal (GI) bleeding, presence of peptic ulcer disease or inflammatory bowel disease, diagnosis of diabetes mellitus, history of neuropathic disease, intraoperative bleeding exceeding 500 mL, surgical duration exceeding 4 hours, necessity to discontinue the analgesics administered in this research.
Sample Size
The sample size for this study was calculated based on a minimum difference in the mean of visual analog scale (VAS) score after 2 hours in the ibuprofen and placebo groups (mean±SD=5.00±2.13 and 3.63±1.75, respectively) with the power of 80% and type I error of 0.05 from the previous research. ^ 15 ^ In the end, 99 patients who met the criteria were enrolled in the study.
Randomization Procedure
Patients were randomly assigned to one of three groups using block randomization in 11 blocks of size 9. The blocks list was extracted from www.sealedenvelope.com. A staff member, who was not involved in any other aspects of the study but had access to the randomization list, prepared the patients’ names for each group and put them in sealed envelopes. The colleagues, including anesthesiologists, surgeons, and members of the data collection team were all blinded to the sizes of the blocks and the allocation of research groups to the patients.
Blinding and Intervention
All study participants adhered to an eight-hour fasting requirement and were prohibited from taking any analgesics for 24 hours preceding surgery. A designated staff member, who was not involved in other aspects of the study and had access to the randomization list, prepared medications in syringes with equivalent volumes. The syringes were then discreetly labeled for each group to maintain the study’s blind nature. The patients, anesthesiologists, surgeons, and data collection team members were blinded to the treatment they received. By randomization, participants in the ketorolac group (n=33) received ketorolac (30 mg/mL, diluted in 100 mL of normal saline 0.9%, equal to 100 mL; EXIR, Iran) 30 min prior to the procedure. Participants in the paracetamol group (n=33) were administered 1000 mg paracetamol (diluted in 100 mL normal saline 0.9%, equal to 100 mL; Varian Pharmed, Iran) 30 min before surgery. The Placebo group received 100 mL of normal saline 0.9% (Darou Pakhsh, Iran) 30 min before the procedure. All the medications were administered with a syringe pump over 15 min.
All patients were hydrated with 3-5 mL/Kg crystalloid solution containing 0.9% normal saline. Vital signs, such as heart rate (HR), blood pressure (BP), oxygen saturation (SpO_2_), electrocardiography (ECG), and capnography, were continuously monitored. A gauge 18 angiocatheter provided IV access. The anesthesia method was the same for all three groups. Anesthesia induction involved midazolam (Midamax^®^, Tehran Chemi, Iran; 0.03-0.06 mg/Kg), fentanyl (Darou Pakhsh, Iran; 2-4 µg/Kg), and morphine (Darou Pakhsh, Iran; 0.1 mg/Kg) as pre-anesthetic medications, followed by Thiopental (VUAB Pharma, Czech Republic; 5 mg/Kg) and Atracurium (Atracural^®^, Alborz Darou, Iran; 0.6 mg/Kg). Endotracheal intubation was performed successfully on the first attempt. Anesthesia maintenance involved isoflurane (Piramal Pharma, India), at a concentration of 1.25% of the minimum alveolar concentration (MAC), and remifentanil (EXIR, Iran), infused at a rate of 0.1-0.4 µg/Kg/min. In cases of severe bleeding, which required blood pressure reduction, an augmented remifentanil (EXIR, Iran) dosage (0.5-1 µg/Kg) was administered alongside Isoflurane. The remifentanil infusion was discontinued at the end of the surgery. The duration of the procedure was limited to a maximum of 4 hours. Following the operation, the neuromuscular block was reversed using neostigmine (Darou Pakhsh, Iran; 0.06 mg/Kg) and atropine (Alborz Darou, Iran; 0.03 mg/Kg). Patients were extubated in the operating room and then transferred to the recovery room. During recovery room and ward stays, patient pain was assessed using the VAS at 1 hour and 6 hours after surgery. If pain severity exceeded 40 in the recovery room, patients were administered 25 mg of pethidine hydrochloride (EXIR, Iran).
Study Assessments
For each participant, demographic data including age and sex were recorded. After extubation, patients were transferred to the recovery room. The nursing staff, who were blinded to the patient’s grouping, monitored their oxygen saturation, blood pressure, and ECG. Furthermore, monitoring of blood pressure, heart rate, and oxygen saturation were constantly monitored in the ward.
This study employed VAS, which consisted of a line ranging from 0 (no pain) to 100 (the greatest conceivable pain). A score of less than 30 was categorized as analgesic success, and a score of more than 70 indicates severe pain.
Statistical Analysis
The data were analyzed using SPSS software (version 22, SPSS Inc., Chicago, IL). The continuous variables were expressed as mean±SD, and categorical variables were summarized as numbers and percentages. A paired t test was used for within-group analysis and ANOVA for continuous variables, followed by Tukey’s multiple comparisons tests. Moreover, the Chi square test was used to assess the difference between the categorical outcome variables. P<0.05 was considered statistically significant.
Results
After excluding 10 patients out of 109 eligible participants, 99 patients were divided into three groups: ketorolac (30 mg IV), paracetamol (1000 mg IV), and placebo (normal saline). A flow diagram illustrating patient recruitment is shown in figure 1.
This figure represents the CONSORT flow diagram of the study.
Table 1 presents the demographic data of the patients. The mean age of the patients in the ketorolac, paracetamol, and placebo groups was 31±7.5, 30±7, and 27±7, respectively. There was no significant difference between the ages of the patients in the three groups (P=0.057). With regard to sex, the frequency of the patients was the same in all three groups (P=0.39). In addition, the frequency of women was higher than men in all three groups (women were almost three times as many as men or more).
One hour after surgery, the mean VAS score was significantly different in the three groups (P<0.001). The mean VAS score in the ketorolac and paracetamol group was less than 3, while in the placebo group (normal saline) was nearly 3.5. Furthermore, the VAS score was calculated 6 hours after surgery and no differences were found between groups (P=0.39). The comparison of VAS scores within the groups at 1 hour and 6 hours after surgery revealed a significant difference (P<0.001) in the placebo group along the time (P<0.001), which showed decreasing close to 1 unit of the VAS score after 5 hours. However, the VAS score in other groups remained constant over time (table 2).
As indicated in table 3, the comparison of the amount of pethidine in the three groups showed that none of the patients in the paracetamol group required a pethidine injection, and only one patient in the ketorolac group required an injection. However, in the placebo group, nearly 60% of the patients (n=19) had pethidine injection (P<0.001).
Discussion
Preventive IV doses of either paracetamol or ketorolac resulted in a significant reduction in one-hour postoperative pain compared to a placebo group. However, no significant pain reduction was observed 6 hours following surgery. Except for one, nearly all patients who received analgesics prior to surgery did not require opioid injections, while more than half of the placebo group requested pethidine.
Patients undergoing septorhinoplasty frequently encounter significant postoperative pain, particularly within the first 3 days. ^ 2 ^ Aydil and others reported that individuals who underwent septorhinoplasty had higher pain scores than those who underwent septoplasty alone. ^ 16 ^ Current pain management practices commonly assume that reducing the consumption of opioids is required to alleviate severe pain due to its potential systemic side effects. Even with the use of various pain relief methods, opioids might still be required. ^ 2 , 15 ^ The present approach to postoperative pain reduction is to combine anti-inflammatory or analgesic medications with opioids. Numerous studies evaluated preventive medications in septorhinoplasty patients. In a study resembling ours, the efficacy of ibuprofen and paracetamol was assessed and revealed higher pain reduction in patients receiving ibuprofen than the paracetamol and placebo group. ^ 17 ^ Similarly, Alshehri conducted a randomized clinical trial and compared ibuprofen and paracetamol. Their findings, which were consistent with ours, indicated that the ibuprofen group experienced higher pain alleviation. ^ 18 ^ Another study investigated the impact of preventive lidocaine infusion and demonstrated its efficacy in both pain control and reducing narcotic demand. ^ 19 ^ Demirhan and colleagues conducted a study and indicated the benefits of combining pregabalin and dexamethasone in pain management. However, it is important to note that this combination was associated with the side effect of blurred vision. ^ 20 ^ In two separate studies, low-dose pregabalin alone was found to be effective, yielding positive effects with minimal side effects. ^ 21 , 22 ^ Koputan and colleagues demonstrated the efficacy of preventive tramadol infiltration at the surgical site 10 min before the operation, not only for pain control but also as a better alternative to levobupivacaine infiltration. ^ 23 ^ Another study, with a smaller sample size, investigated the preventive analgesic efficacy of low-dose ketamine infusion, concluding that patients receiving ketamine experienced lower postoperative pain and relied less on rescue opioids. Intraoperative magnesium sulfate infusion also yielded positive outcomes for septorhinoplasty patients, including reduced postoperative pain and enhanced recovery. ^ 24 ^ A systematic review published in 2019 supported the use of local anesthetics, NSAIDs, gabapentin, and alpha-agonists as effective pain-control modalities for septorhinoplasty patients. ^ 25 ^
Paracetamol, which is extensively used as an analgesic and antipyretic for mild to moderate pain, has a historical association with NSAIDs due to its inhibition of COX-2 pathways. However, its exact mechanism of action is unknown. ^ 26 , 27 ^ In 2015, a comprehensive systematic review suggested that preventive paracetamol significantly reduced opioid consumption, which underscored its clinical value. ^ 28 ^ Ketorolac, utilized for moderate to severe pain, manifests in various pharmaceutical forms, including oral, nasal spray, IV, and intramuscular. Its efficacy extends to reducing opioid consumption, minimizing gastrointestinal motility issues, and alleviating postoperative nausea. ^ 29 ^ Although ketorolac, the same as other NSAIDs, block the cyclooxygenases (COXs), it is more effective than other NSAIDS. ^ 30 ^
Several studies evaluated and compared the analgesic effect of paracetamol and ketorolac at preventative dosages. In 2020, Javaherforooshzadeh and others found no significant difference in pain reduction intensity between ketorolac and paracetamol within the 1^st^ and 6^th^ hours after coronary artery bypass surgery. The findings indicated that paracetamol were significantly more successful in reducing pain intensity at 24 and 48 hours post-surgery. ^ 31 ^ A double-blind study in the same year by Dastan and colleagues assessed the analgesic effects of ketorolac, paracetamol, and IV morphine in patients undergoing thoracoscopy. The results revealed that the ketorolac and paracetamol group had a significantly lower mean pain score than the morphine-only group. However, there was no significant difference concerning morphine consumption between the paracetamol and ketorolac groups. ^ 32 ^ Jahangiri Fard and others examined the analgesic efficacy of these two drugs in thoracic surgery patients and found no significant difference in pain scores at any time after the procedure. ^ 33 ^
In acknowledging the limitations of the present study, it is important to note the small sample size, which might affect the generalizability of the findings. Furthermore, giving participants a single preventive dose before surgery might not fully capture the varying nature of postoperative pain. Using a more varied dosing regimen could help us better understand how effective the medications are over time. Recognizing the inherent differences in the half-life of paracetamol and ketorolac is crucial, especially given the 6-hour duration for the second pain assessment, which might not fully capture all potential variations in the duration of their pain-relieving effects. Another limitation was the absence of a pain assessment after 6 hours postoperatively, which left a gap in understanding the medications’ long-term efficacy beyond the initial hours.
Conclusion
The present study on the preoperative administration of paracetamol and ketorolac in septorhinoplasty patients demonstrated that they had a significant impact on reducing one-hour postoperative pain. The majority of the patients who received these medications as a preventive measure did not require to use opioids, which was in line with reduced reliance on opioids. These findings encourage further research into optimized drug combinations and individualized approaches to enhance patient outcomes.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Heppt W Gubisch W Septal surgery in rhinoplasty Facial Plast Surg 2011271677810.1055/s-0030-127129721404159 · doi ↗ · pubmed ↗
- 2Szychta P Antoszewski B Assessment of early post-operative pain following septorhinoplasty J Laryngol Otol 20101241194910.1017/S 002221511000151920602848 · doi ↗ · pubmed ↗
- 3Savoia G Alampi D Amantea B Ambrosio F Arcioni R Berti Metal Postoperative pain treatment SIAARTI Recommendations 2010. Short version Minerva Anestesiol 2010766576720661210 · pubmed ↗
- 4Gadkaree SK Shaye DA Occhiogrosso J Lee LN Association Between Pain and Patient Satisfaction After Rhinoplasty JAMA Facial Plast Surg 2019214759[ PMC Free Article ]10.1001/jamafacial.2019.080831536105 PMC 6753502 · doi ↗ · pubmed ↗
- 5Kehlet H Wilkinson RC Fischer HB Camu F Prospect Working G PROSPECT: evidence-based, procedure-specific postoperative pain management Best Pract Res Clin Anaesthesiol 2007211495910.1016/j.bpa.2006.12.00117489225 · doi ↗ · pubmed ↗
- 6Neugebauer E Sauerland S Keck V Simanski C Witte J [Surgical pain management. A Germany-wide survey including the effect of clinical guidelines] Chirurg 200374235810.1007/s 00104-003-0615-912647080 · doi ↗ · pubmed ↗
- 7Rathmell JP Wu CL Sinatra RS Ballantyne JC Ginsberg B Gordon D Betal Acute post-surgical pain management: a critical appraisal of current practice, December 2-4, 2005 Reg Anesth Pain Med 20063114210.1016/j.rapm.2006.05.00216849098 · doi ↗ · pubmed ↗
- 8Gordon DB Dahl JL Miaskowski C Mc Carberg B Todd KH Paice J Aetal American pain society recommendations for improving the quality of acute and cancer pain management: American Pain Society Quality of Care Task Force Arch Intern Med 200516515748010.1001/archinte.165.14.157416043674 · doi ↗ · pubmed ↗