Oral Granular Cell Tumour on the Mandibular Gingiva in an Adult: A Rare Case Report
Yosuke Iijima, Keisuke Sawada, Mami Yamazaki, Miki Yamada, Shunsuke Hino, Norio Horie, Takahiro Kaneko

TL;DR
This case report describes a rare instance of a granular cell tumor found on the gum instead of the tongue in an adult.
Contribution
The novelty is the rare presentation of a granular cell tumor on the mandibular gingiva rather than the typical tongue location.
Findings
A 75-year-old man had a granular cell tumor diagnosed on his mandibular gingiva.
Granular cell tumors are typically found on the tongue, not the gums.
This case highlights the need to consider this tumor type in unusual oral locations.
Abstract
Introduction: Granular cell tumours are rare benign tumours. In the oral cavity, these tumours are predominantly found on the tongue. This report describes a rare case of a granular cell tumour arising on the gingiva. Case Presentation: A 75-year-old man was referred to the department with a mandibular gingival mass. Intraoral examination revealed a relatively firm mass in the lingual gingiva around the left mandibular premolar. Biopsy results led to a diagnosis of granular cell tumour. Conclusion: Oral granular cell tumours can, in rare cases, occur in areas other than the tongue, such as the gingiva.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
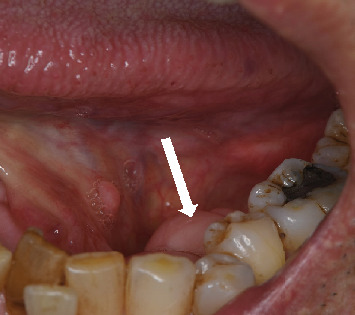 Figure 1
Figure 1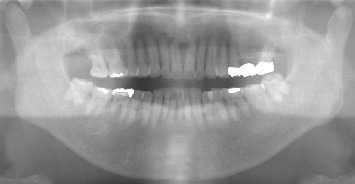 Figure 2
Figure 2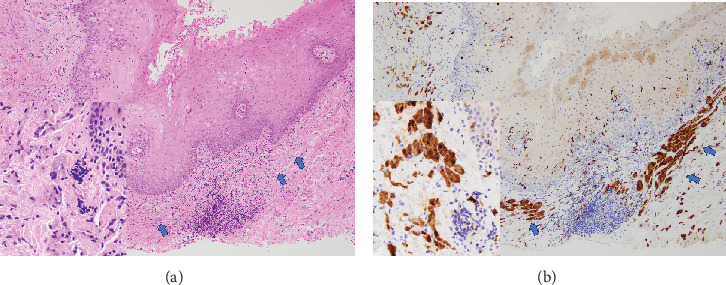 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsTumors and Oncological Cases
1. Introduction
Granular cell tumours are a rare benign soft tissue tumour derived from Schwann cells, and the overall incidence of granular cell tumours in surgical specimens has been reported as 0.03% [1, 2]. Histologically, tumour cells contain abundant fine eosinophilic granules in the cytoplasm and are immunobiologically positive for S-100 protein. Recent studies using whole-exome sequencing and targeted sequencing analysis have identified inactivating mutations of ATP6AP1 and ATP6AP2 as likely oncogenic drivers of granular cell tumours [3, 4]. Granular cell tumours are mainly found in the skin (30%–40%), gastrointestinal tract (5%–11%), breast (15%), and respiratory tract (10%), with a predilection for the oral cavity [2, 5]. In the oral cavity, the vast majority of cases arise on the tongue, with a small number of reports describing the involvement of other parts of the oral cavity [6]. We describe a case of granular cell tumour arising in the gingiva, which is relatively rarely reported [7, 8].
2. Case Report
A 75-year-old man was referred to the department through his family dentist after a mass noticed on the left mandibular gingiva of the mouth 1 month earlier had not disappeared. The patient had hypertension, was taking amlodipine, and had been smoking 13 cigarettes daily since the age of 20. His alcohol consumption had recently been 350 mL/day of beer.
Intraoral findings showed a relatively firm mass on the lingual gingiva around the mandibular left premolar, with normal mucosal colouration and a diameter of 10 mm, away from the floor of the mouth (Figure 1). No other abnormalities were evident in the oral region, including in the regional lymph nodes. Radiological examination showed no abnormalities of bone around the left lower first premolar (Figure 2).
The mass was excised under local anaesthesia with a clinical diagnosis of gingival fibroma. Histopathologically, the excised specimen was nonencapsulated and showed a thin, widespread distribution of polygonal cells with central small dark nuclei and cytoplasmic eosinophilic granules. No evidence of cytological atypia, mitotic activity, or necrosis suggestive of malignant transformation was observed (Figure 3a). Immunohistochemically, tumour cells were positive for S-100 protein (Figure 3b). The histopathological diagnosis was granular cell tumour. Twelve months after removal, no recurrence or malignant transformation was observed.
3. Discussion
According to a systematic review by Lafuente-Ibáñez de Mendoza et al., oral granular cell tumours are more common in women (74% female and 26% male), with a mean age at onset of 35.24 years. The predominant site in the oral cavity is the tongue (76%), followed by the lips (11%), the buccal area (5%), the palate (4%), the floor of the mouth (3%), and the gingiva (1%) [6]. Cases involving the gingiva appear rare, with only three reports, including the present [7, 8]. Clinically, granular cell tumours on the tongue were found as asymptomatic, slightly firm, well-delineated submucosal nodules of about 10 mm in diameter. The tumour in the present case was likewise recognised as a nodular lesion on the gingiva, but as very few cases have involved the gingiva, accumulation of more cases is required for valid characterisation. Most cases of granular cell tumour involved solitary lesions, but some showed multiple intra- and extraoral manifestations [9–11]. In addition, multiple granular cell tumours have been shown to be associated with syndromes such as Noonan syndrome, Neurofibromatosis Type 1, and LEOPARD syndrome [2, 12].
Histopathologically, a granular cell tumour presents as an infiltrative, nonencapsulated, submucosal lesion comprising sheets, nests, or trabeculae of large, polygonal cells with abundant, eosinophilic, finely granular cytoplasm [6, 13]. These tumour cells are immunohistochemically positive for S-100 protein (supporting the neural origin of granular cell tumour), as well as for neuron-specific enolase, CD68, calretinin, CD57, inhibin, TFE3, SOX, CD59, PGP9.5, and vimentin [7, 14, 15]. Granular cell tumours of the oral cavity that do not stain for S-100 protein but are positive for CD68 and vimentin have also been reported recently. Some researchers have suggested that the granules are derived from intracytoplasmic lysosomal granules [16]. In one-third of cases of oral granular cell tumours, pseudoepitheliomatous hyperplasia of the covering epithelium is observed. This pseudoepitheliomatous hyperplasia is readily misidentified as squamous cell carcinoma, so care should be taken with the depth of the biopsy [6, 17]. No pseudoepitheliomatous hyperplasia of the covering epithelium was observed in the present case.
The differential diagnosis of granular cell tumour arising in the gingiva requires differentiation from various odontogenic and nonodontogenic mass-forming proliferative diseases. Radiographic examination facilitates diagnosis, but whether this pathology shows specific bone findings remains unclear, as granular cell tumours arising in the gingiva are extremely rare. For example, radiopaque images may help with differentiation from osteogenic lesions such as peripheral ossifying fibroma, while radiolucent images may help with differentiation from malignant tumours, including metastatic ones. In any case, a histopathological search is essential. Aside from diseases within the jawbones, diseases with granular cells in adult soft tissues include primitive non-neural granular cell tumours, adult rhabdomyomas, and malignant melanomas. Primitive non-neural granular cell tumours are negative for S-100 protein [18]. Adult rhabdomyomas are positive for desmin and myogenin [19]. Malignant melanomas with occasional granular cell changes show diffuse positivity for S-100 protein and positivity for melanocytic markers [13].
Granular cell tumours have been reported to have a malignant aspect in less than 2% of all cases, and histological criteria for diagnosis have also been provided. Six histological criteria are assessed in the Fanburg–Smith criteria: necrosis, spindling, vesicular nuclei with large nucleoli, increased mitotic activity (> 2 mitoses/10 high magnification fields at ×200 magnification), high nuclear-to-cytoplasmic (N:C) ratio, and pleomorphism. Neoplasms meeting three or more of these criteria are histologically classified as malignant, while those meeting one or two criteria are classified as atypical, and those showing only focal pleomorphism and not meeting any other criteria are classified as benign [17]. The neoplasm in the present case was judged to be benign. No reports have described malignant cases in the oral cavity, but one case of an aggressive tumour with ulceration of the buccal mucosa has been reported, although it was not histologically classified as malignant [6, 20].
In terms of treatment, complete surgical resection is recommended due to the proliferative nature of the lesion.
In conclusion, oral granular cell tumours can, in rare cases, occur in areas other than the tongue, such as the gingiva.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Lack E. E. Worsham G. F. Callihan M. D. Granular cell Tumor: A Clinicopathologic Study of 110 Patients Journal of Surgical Oncology 198013430131610.1002/jso.29301304052-s 2.0-00188931606246310 · doi ↗ · pubmed ↗
- 2Neelon D. Lannan F. Childs J. Granular Cell Tumor Stat Pearls 2023 Stat Pearls Publishing 33085297 · pubmed ↗
- 3Pareja F. Brandes A. H. Basili T. Loss-of-Function Mutations in ATP 6AP 1 and ATP 6AP 2 in Granular Cell Tumors Nature Communications 201891 p. 353310.1038/s 41467-018-05886-y 2-s 2.0-8505261835430166553 PMC 6117336 · doi ↗ · pubmed ↗
- 4Sekimizu M. Yoshida A. Mitani S. Frequent Mutations of Genes Encoding Vacuolar H(+) -AT Pase Components in Granular Cell Tumors Genes, Chromosomes & Cancer 201958637338010.1002/gcc.227272-s 2.0-8506033751030597645 · doi ↗ · pubmed ↗
- 5Barakat M. Kar A. A. Pourshahid S. Gastrointestinal and Biliary Granular Cell Tumor: Diagnosis and Management Annals of Gastroenterology 201831443944710.20524/aog.2018.02752-s 2.0-8504961948929991888 PMC 6033765 · doi ↗ · pubmed ↗
- 6de Lafuente Ibáñez Mendoza I. López Ortega K. Trierveiler M. Oral Granular Cell Tumour: A Multicentric Study of 56 Cases and a Systematic Review Oral Diseases 202026357358910.1111/odi.1327331898368 · doi ↗ · pubmed ↗
- 7Buley I. D. Gatter K. C. Kelly P. M. Heryet A. Millard P. R. Granular Cell Tumours Revisited. An Immunohistological and Ultrastructural Study Histopathology 198812326327410.1111/j.1365-2559.1988.tb 01941.x 2-s 2.0-00238845492452781 · doi ↗ · pubmed ↗
- 8Eguia A. Uribarri A. Gay Escoda C. Crovetto M. A. Martínez-Conde R. Aguirre J. M. Granular Cell Tumor: Report of 8 Intraoral Cases Medicina Oral, Patología Oral Y Cirugía Bucal 2006115 E 425E 42816878061 · pubmed ↗