Dietary Upper Gastrointestinal Obstruction Caused by Mushrooms
Yuto Shiozaki, Takuya Otsuki, Kosuke Ishizuka, Yuichi Kato, Kenya Ie, Chiaki Okuse

TL;DR
People with a history of peptic ulcers can experience upper GI blockage from food, and early endoscopic removal is key to quick recovery.
Contribution
Highlights the risk of dietary obstruction in peptic ulcer patients and advocates for early endoscopic intervention.
Findings
Dietary obstruction at the pylorus can occur in patients with a history of peptic ulcers.
Early endoscopic evaluation and removal of the obstruction can rapidly improve symptoms and prevent complications.
Abstract
In patients with a history of peptic ulcer, dietary upper gastrointestinal obstruction at the pylorus may occur. Early endoscopic evaluation should be considered when obstruction is suspected, as timely removal of the foreign body can rapidly improve symptoms and prevent complications.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 FIGURE 1
FIGURE 1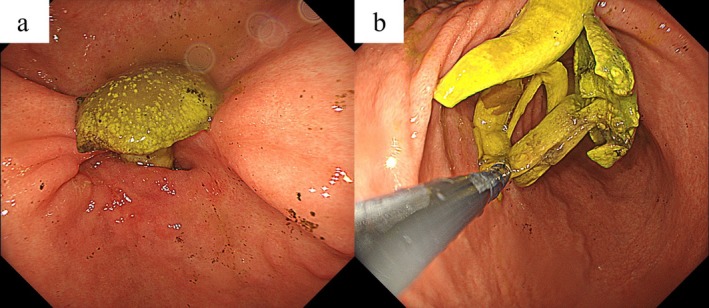 FIGURE 2
FIGURE 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsForeign Body Medical Cases · Esophageal and GI Pathology · Biliary and Gastrointestinal Fistulas
Case
1
A 63‐year‐old Japanese man with a history of duodenal ulcer presented with frequent vomiting after eating and drinking since the previous day. He was taking rabeprazole sodium 20 mg/day. On physical examination, his temperature was 37.3°C, pulse rate was 130 beats per minute, blood pressure was 143/93 mmHg, respiratory rate was 18 breaths per minute, and SpO_2_ was 98% on room air. Laboratory tests revealed an elevated blood urea nitrogen of 30.3 mg/dL and serum creatinine of 2.23 mg/dL, suggesting possible dehydration or acute kidney injury. Abdominal computed tomography revealed gastric dilatation and luminal stricture of the digestive tract extending from the pylorus to the duodenal bulb (Figure 1). The patient was admitted and managed with fasting and intravenous fluid replacement. On the second day of hospitalization, esophagogastroduodenoscopy (EGD) revealed a mushroom‐like foreign body impacted in the pyloric region, along with deformity of the pyloric ring and narrowing of the duodenal bulb, likely caused by a previous duodenal ulcer (Figure 2). Foreign body removal was successfully performed endoscopically. The patient's symptoms, particularly vomiting, improved rapidly, allowing for the gradual reintroduction of food starting from the third day of hospitalization. He was discharged on the 8th day without any recurrence of symptoms.
(a) Gastric dilatation, (b) Luminal stricture.
(a) Mushroom shade fitted into the pyloric region, (b) Removal of endoscopes.
Upper gastrointestinal obstruction can result from the ingestion of foreign bodies, malignant tumors, or peptic ulcers. The majority of upper gastrointestinal obstructions due to ingestion in adults are diet‐related, most commonly occurring in the esophagus and often at sites of physiologic stricture, with pyloric obstruction being a rare occurrence [1]. Foods that can cause dietary upper gastrointestinal obstruction include meat, fish bones, rice cakes, and gastroliths [2]. For sharp objects, magnets, batteries, or large and long objects lodged in the stomach, EGD within 24 h is recommended to prevent complications [3].
Author Contributions
Yuto Shiozaki: writing – original draft. Takuya Otsuki: writing – review and editing. Kosuke Ishizuka: writing – review and editing. Yuichi Kato: writing – review and editing. Kenya Ie: writing – review and editing. Chiaki Okuse: writing – review and editing.
Consent
Written informed consent was obtained from the patient for the publication of this case report and accompanying images.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1K. Tantillo , R. J. Dym , V. Chernyak , M. H. Scheinfeld , and B. H. Taragin , “No Way out: Causes of Duodenal and Gastric Outlet Obstruction,” Clinical Imaging 65 (2020): 37–46, 10.1016/j.clinimag.2020.04.017.32353717 · doi ↗ · pubmed ↗
- 2A. Oka , S. Ishihara , H. Mikami , et al., “Retained Rice Cake: A Unique Upper Gastrointestinal Foreign Body: Case Report and a Literature Review,” Internal Medicine 58, no. 17 (2019): 2485–2494, 10.2169/internalmedicine.2760-19.31178509 PMC 6761341 · doi ↗ · pubmed ↗
- 3M. Birk , P. Bauerfeind , P. H. Deprez , et al., “Removal of Foreign Bodies in the Upper Gastrointestinal Tract in Adults: European Society of Gastrointestinal Endoscopy (ESGE) Clinical Guideline,” Endoscopy 48 (2016): 489–496.26862844 10.1055/s-0042-100456 · doi ↗ · pubmed ↗