Sequential Development of Waldenström’s Macroglobulinemia After High-Grade Lymphomatoid Granulomatosis
Makoto Ito, Yusei Mizumoto, Yasushi Murakami, Satsuki Nakano, Norio Takagi

TL;DR
A rare case shows how a high-grade lymphoma can progress to Waldenström’s macroglobulinemia, highlighting diagnostic and treatment challenges.
Contribution
This case report documents a rare sequential development of Waldenström’s macroglobulinemia after high-grade LYG.
Findings
High-grade LYG can cause Pancoast syndrome and respond to R-CHOP therapy.
LYG may progress to LPL/WM after initial remission, complicating treatment.
Relapsed LYG remains difficult to treat despite bendamustine-rituximab.
Abstract
Lymphomatoid granulomatosis (LYG) is a rare Epstein-Barr virus-driven B-cell lymphoproliferative disease that often progresses to high-grade lymphoma. We describe a case of high-grade LYG causing Pancoast syndrome, diagnosed via transbronchial biopsy after a failed incisional biopsy. Complete remission was achieved with R-CHOP (rituximab, doxorubicin, cyclophosphamide, vincristine, and prednisolone), but 2.5 years later, the patient developed lymphoplasmacytic lymphoma/Waldenström’s macroglobulinemia (LPL/WM). Despite bendamustine-rituximab improving LPL/WM, LYG recurred, underscoring its treatment challenges. This case highlights LYG’s diagnostic complexity, its potential link with other hematologic malignancies, and therapeutic limitations. Further research is needed to elucidate LYG’s pathogenesis and develop effective treatments for relapsed cases.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
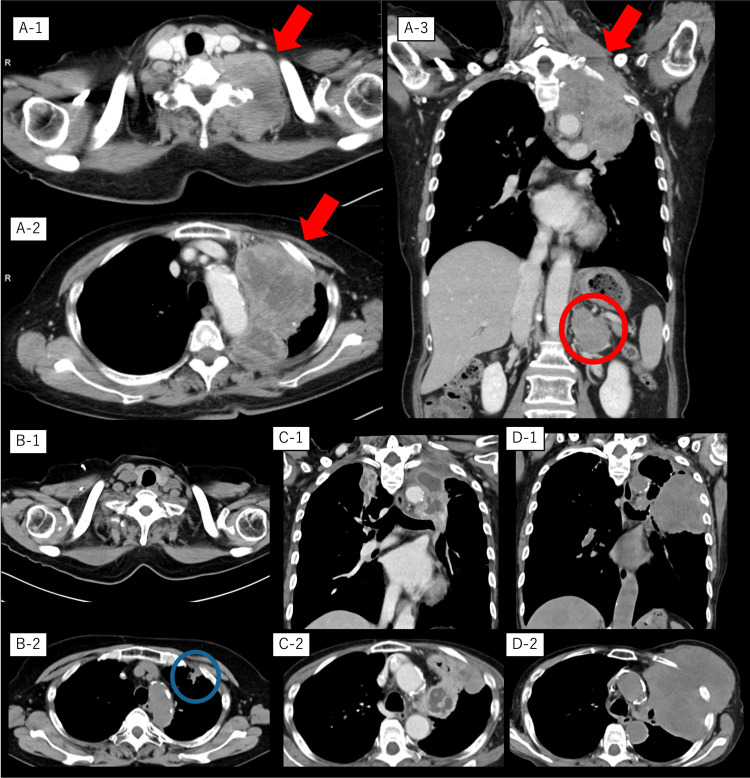 Figure 1
Figure 1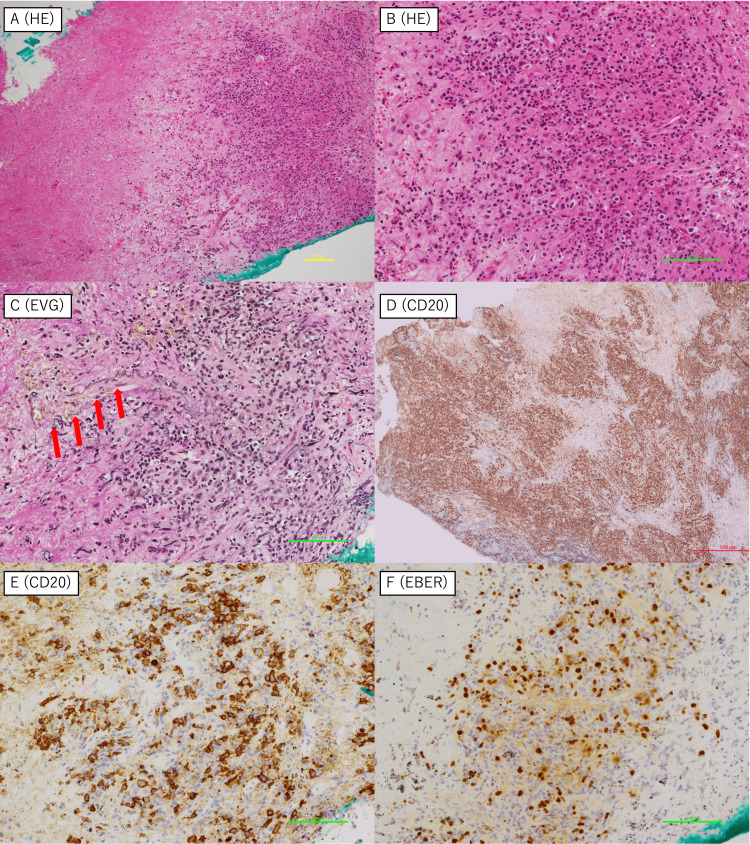 Figure 2
Figure 2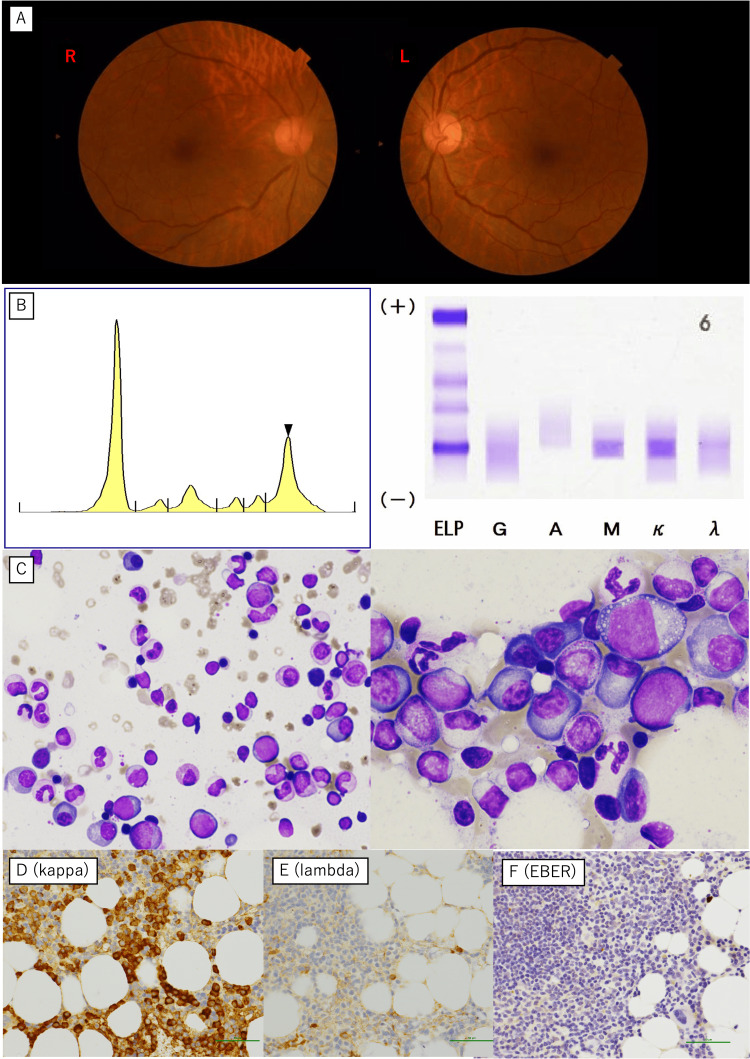 Figure 3
Figure 3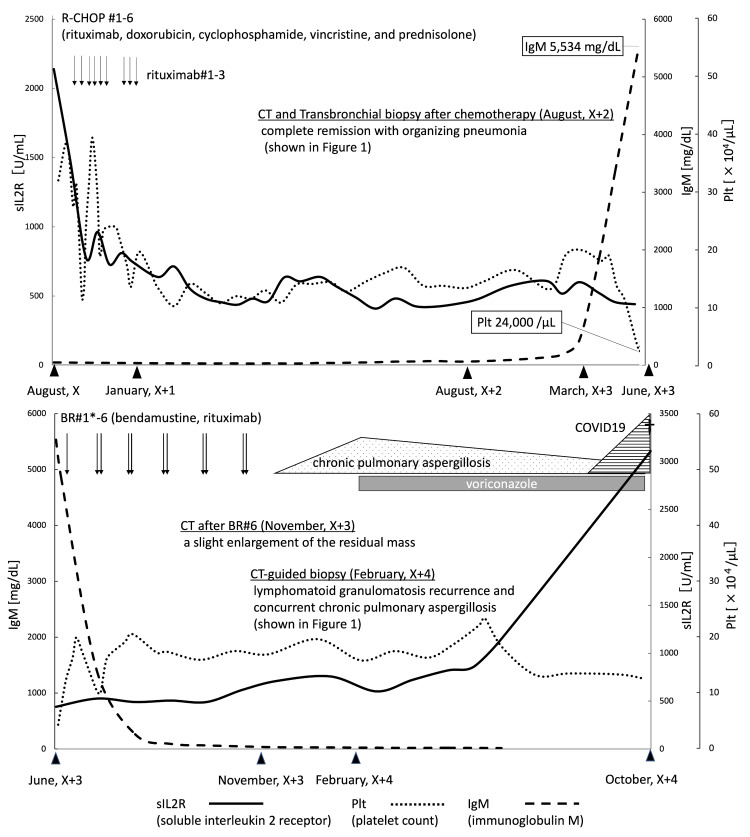 Figure 4
Figure 4| Complete blood test | Observed value | Reference range |
| White blood cell | 9,800/μL | 3,300-8,600/μL |
| Band neutrophil | 11.3% | 2.0%-13.0% |
| Segmented neutrophil | 57.0% | 38.0%-58.9% |
| Lymphocyte | 23.7% | 26.2%-46.6% |
| Monocyte | 7.7% | 2.3%-7.7% |
| Basophil | 0.3% | 0.0%-0.6% |
| Eosinophil | 0.0% | 0.0%-1.0% |
| Red blood cell | 446 × 104/μL | 410-510 × 104/μL |
| Reticulocyte | 12‰ | 2‰-17‰ |
| Hemoglobin | 11.9 g/dL | 13.7-16.8 g/dL |
| Platelet | 27.2 × 104/μL | 15.8-34.8 × 104/μL |
| Albumin | 3.7 g/dL | 4.1-5.1 g/dL |
| Total bilirubin | 0.4 mg/dL | 0.2-1.0 mg/dL |
| Aspartate aminotransferase | 28 U/L | 13-30 U/L |
| Alanine aminotransferase | 12 U/L | 8-20 U/L |
| Lactate dehydrogenase | 290 U/L | 124-222 U/L |
| Blood urea nitrogen | 8.8 mg/dL | 8.0-20.0 mg/dL |
| Creatinine | 0.65 mg/dL | 0.65-1.07 mg/dL |
| Sodium | 131 mEq/L | 138-145 mEq/L |
| Potassium | 4.3 mEq/L | 3.6-4.8 mEq/L |
| Chloride | 95 mEq/L | 101-108 mEq/L |
| Calcium | 9.5 mg/dL | 8.8-10.1 mg/dL |
| Ferritin | 632.1 ng/mL | 40-188 ng/mL |
| C-reactive protein | 6.20 mg/dL | 0.00-0.14 mg/dL |
| Carcinoembryonic antigen | 0.79 ng/mL | 0.0-5.0 ng/mL |
| Cytokeratin 19 fragment | 0.0 ng/mL | 0.0-3.5 ng/mL |
| Pro-gastrin-releasing peptide | 29.8 pg/mL | <80 pg/mL |
| Soluble interleukin-2 receptor | 2,140 U/mL | 145-519 U/mL |
| Immunoglobulin G | 924 mg/dL | 870-1,700 mg/dL |
| Immunoglobulin A | 162 mg/dL | 110-410 mg/dL |
| Immunoglobulin M | 49 mg/dL | 33-190 mg/dL |
| Epstein-Barr virus-viral capsid antigen-immunoglobulin M | <10 | <10 |
| Epstein-Barr virus-viral capsid antigen-immunoglobulin G | 1:40 | <10 |
| Epstein-Barr virus nuclear antigen | 1:10 | <10 |
| Human immunodeficiency virus antibody | Negative | Negative |
| Case | Authors | Journal | Year | Associated hematologic malignancy | Timing of onset | Summary |
| LYG with hematologic malignancy cases | ||||||
| 1 | Ragage et al. | Ann Pathol | 2006 | Acute myeloid leukemia (AML) | Prior to LYG | Case of pulmonary LYG developed in an immunocompromised state after AML treatment [ |
| 2 | Kim | Korean J Spine | 2012 | Acute lymphoblastic leukemia (ALL) | Prior to LYG | Spinal LYG after treatment for childhood ALL [ |
| 3 | Michot et al. | Leuk Lymphoma | 2013 | T-large granular lymphocyte leukemia (T-LGL) | Prior to LYG | T-LGL preceded the diagnosis of LYG by 3 years, suggesting that LG is secondary to T-LGL [ |
| 4 | De Luca et al. | Leuk Lymphoma | 2018 | T-LGL | Prior to LYG | Pulmonary LYG occurred after T-LGL leukemia development [ |
| 5 | Rezvani et al. | Case Rep Pulmonol | 2019 | Chronic lymphocytic leukemia (CLL) | Prior to LYG | Report of rapidly progressive pulmonary LYG in a patient with CLL [ |
| 6 | Lee et al. | Intern Med | 2019 | Multiple myeloma (MM) | Simultaneous | Simultaneous onset of CNS/pulmonary LYG and MM under immunosuppressive conditions [ |
| 7 | Szczepanek et al. | Front Neurol | 2020 | CNS Hodgkin lymphoma (HL) | Simultaneous | Simultaneous onset of CNS HL and pulmonary LYG during immunosuppressive therapy for ulcerative colitis [ |
| 8 | Bi et al. | Front Oncol | 2022 | Chronic myeloid leukemia (CML) | Prior to LYG | CML patient developed LYG and pulmonary infection during treatment [ |
| LPL/WM after B-cell malignancy cases | ||||||
| 9 | Uğur et al. | Tepecik Eğit Hast Derg | 2014 | Non-Hodgkin lymphoma (NHL) | WM after NHL treatment | WM occurred 3 years after NHL treatment; reported as secondary malignancy [ |
| 10 | Samsuddoha et al. | Cureus | 2024 | Chronic lymphocytic leukemia (CLL) | WM after CLL | Very rare case of CLL transforming into WM during ibrutinib therapy [ |
| LYG-WM/LPL association case | ||||||
| 11 | Melegh et al. | Pathol Res Pract | 2009 | Lymphoplasmacytic lymphoma (LPL) | LYG after LPL treatment | Cervical LYG occurred under immunosuppression after treatment for LPL [ |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsChronic Lymphocytic Leukemia Research · Lymphoma Diagnosis and Treatment · Viral-associated cancers and disorders
Introduction
Lymphomatoid granulomatosis (LYG) is a rare Epstein-Barr virus (EBV)-driven B-cell lymphoproliferative disease first described by Liebow et al. [1]. LYG is characterized by angiocentric and angiodestructive infiltration of EBV-positive B-cells and is often accompanied by necrosis [2]. The clinical course varies widely, ranging from spontaneous remission to progression into aggressive lymphoma. High-grade LYG has a poor prognosis, with median progression-free survival and overall survival of approximately one and two years, respectively, even with rituximab-based regimens such as R-CHOP (rituximab, doxorubicin, cyclophosphamide, vincristine, and prednisolone) [2,3]. Waldenström’s macroglobulinemia (WM), a subtype of lymphoplasmacytic lymphoma (LPL), is a rare B-cell malignancy characterized by monoclonal IgM production and bone marrow infiltration. The age-adjusted incidence rate of WM/LPL in the United States is approximately 0.63 per 100,000 person-years, with the highest rates observed among White populations (0.74 per 100,000). In Japan, the reported incidence is approximately 0.28 per 100,000 person-years [4]. Even more rarely, LYG is an EBV-associated B-cell lymphoproliferative disorder for which precise epidemiological data are lacking due to its extreme rarity. Although LYG is recognized as a disorder often associated with immunodeficiency states [2], its coexistence or sequential development with LPL/WM has not been reported. The coexistence or sequential development of LPL/WM following other EBV-related lymphoproliferative disorders is extremely rare and, to our knowledge, has not been reported before. In this report, we describe a unique case of LYG that later developed LPL/WM and highlight the diagnostic challenges, disease progression, and therapeutic strategies.
Case presentation
A 73-year-old woman presented with left chest and arm pain that had persisted for three months and was accompanied by a gradually enlarging palpable tumor in the left neck region. She had no significant medical history, smoking history, or family history of systemic disease or cancer. Physical examination revealed left eyelid ptosis, neck swelling, and tenderness. Laboratory results showed elevated C-reactive protein and soluble interleukin-2 receptor levels but normal immunoglobulin M levels (Table 1). Hyponatremia was likely secondary to the syndrome of inappropriate antidiuretic hormone secretion associated with the tumor or inflammatory cytokine release.
Contrast-enhanced computed tomography (CT) revealed a 9-cm mass extending from the left pulmonary apex to the neck, along with left adrenal metastasis as shown in Figure 1A-1 to Figure 1A-3.
Computed tomography images of the patient during the clinical courseContrast-enhanced computed tomography images at hospitalization (A-1, A-2, and A-3), after six cycles of R-CHOP (rituximab, doxorubicin, cyclophosphamide, vincristine, and prednisolone) therapy (B-1 and B-2), at relapse of lymphomatoid granulomatosis (C-1 and C-2), and just before the patient passed away (D-1 and D-2). Red arrows indicate the primary lesion from the left lung apex to the neck; the red circle indicates a metastatic lesion in the left adrenal gland. A transbronchial lung biopsy performed on the residual lesions showed organizing pneumonia (blue circle).
Although a transbronchial biopsy (TBB) was rapidly performed, it yielded seemingly insufficient diagnostic material due to prominent necrosis observed on hematoxylin-eosin staining. An incisional biopsy of the supraclavicular lesion was also performed to obtain a certain amount of tumor specimens. While the additional biopsy confirmed only large B-cell lymphoma, TBB ultimately established a diagnosis of grade 3 LYG through histopathological findings, including angiodestruction, angioinvasion, coagulative necrosis, and EBV-encoded RNA (EBER) positivity (Figure 2).
Histopathological findings of the lung specimens at the diagnosis of lymphomatoid granulomatosisHistopathological examination revealed prominent coagulative necrosis (A) and angiocentric and angiodestructive lymphoid infiltration (B, C). Red arrows indicate the destructed vessels on Elastica van Gieson (EVG) staining (C). CD20-positive atypical large B-cells infiltrated in clusters (D, E), and these lymphocytes were positive for Epstein-Barr virus-encoded RNA (EBER) (F).HE: hematoxylin-eosin
Given the diagnosis of high-grade LYG with Pancoast syndrome (Horner’s syndrome and brachial plexus involvement), R-CHOP therapy was initiated immediately. After one cycle, the patient experienced rapid pain relief, obviating the need for analgesics. Following six R-CHOP cycles and three cycles of additional rituximab monotherapy, complete remission (CR) was achieved. Follow-up CT performed one year after the initial chemotherapy revealed a suspected residual lesion in the left lung apex. Subsequent TBB of this area led to a diagnosis of organizing pneumonia, suggesting that the lesion represented post-chemotherapy scarring rather than residual malignancy as shown in Figures 1B-1, 1B-2.
However, 2.5 years later, the patient developed retinopathy due to hyperviscosity, a rapidly elevated IgM level (5,534 mg/dL, reference range: 33-190 mg/dL), and thrombocytopenia (platelet count: 24,000/μL, reference range: 15.8-34.8 × 104/μL). Bone marrow biopsy confirmed LPL/WM, which was characterized by monoclonal IgM-kappa production and EBER negativity (Figure 3). The markedly elevated IgM level was indicative of a hyperviscosity syndrome, explaining the development of retinopathy. Thrombocytopenia likely resulted from bone marrow infiltration by lymphoplasmacytic cells. The detection of monoclonal IgM-kappa protein confirmed the diagnosis of WM. EBER negativity in the bone marrow further supported the notion that the newly diagnosed lymphoma was unrelated to prior EBV-driven LYG.
Findings observed at the diagnosis of lymphoplasmacytic lymphoma/Waldenström’s macroglobulinemiaMarked venous engorgement (sausaging) was observed (A). Serum protein electrophoresis and immunoelectrophoresis revealed M-peak (arrowhead) and IgM-kappa type M-protein (B). May-Giemsa staining showed an increased number of small lymphocytes and plasma cells in the bone marrow (C). Immunohistochemical staining revealed positive for kappa light chains (D) but negative for lambda light chains (E) and Epstein-Barr virus-encoded RNA (EBER) (F).
At the time of WM diagnosis, when LYG was still in remission, six cycles of bendamustine-rituximab (BR) were administered for LPL/WM, resulting in the clinical improvement of retinopathy, IgM levels, and platelet counts. However, follow-up CT after six cycles of BR revealed progressive thoracic mass enlargement and internal fluid retention. CT-guided biopsy confirmed LYG recurrence with concurrent Aspergillus fumigatus infection as shown in Figures 1C-1, 1C-2. The patient declined further chemotherapy, opting for the best supportive care. Despite antifungal treatment with voriconazole, the patient succumbed to COVID-19-related complications. The entire treatment trajectory is shown in Figure 4.
*The overall clinical course of the patientThe patient visited our hospital in August of year X, developed Waldenström’s macroglobulinemia in March of year X+3, and passed away in October of year X+4.We administered bendamustine monotherapy during the first course of BR therapy.BR: bendamustine-rituximab; CT: computed tomography
Discussion
To our knowledge, this is the first reported case of WM developing after high-grade LYG, highlighting a potentially underrecognized association between these rare B-cell malignancies. This case underscores three critical aspects of LYG and its management: diagnostic challenges, secondary hematologic malignancies, and therapeutic strategies.
Diagnostic challenges
The diagnosis of LYG is inherently challenging because the disease is exceedingly rare and exhibits very subtle histological features [5]. The initial differential diagnoses in this case included lung cancer, granulomatosis with polyangiitis, other EBV-associated lymphoproliferative disorders, and infectious causes. However, histopathological findings such as angiocentric and angiodestructive infiltration, necrosis, and EBER positivity in B-cells by in situ hybridization were highly characteristic of LYG and allowed us to distinguish it from these other conditions. TBB has emerged as a less invasive alternative to surgical lung biopsy in lung cancer diagnosis, although its diagnostic yield and sensitivity are slightly lower than those of surgical biopsy [6]. TBB may occasionally fail to provide an accurate diagnosis due to tissue contusion caused by mechanical clamping, necessitating subsequent surgical biopsy. Nevertheless, the TBB specimen in this case was analyzed successfully and presented the features of LYG grade 3, including angiocentric infiltration, coagulative necrosis, and EBER positivity. This observation is interesting, as lesions at the leading edge of the tumor may not consistently exhibit the hallmark histopathological findings of LYG. Although the exact mechanism underlying this phenomenon remains unclear, these findings emphasize the importance of the multidimensional evaluation of LYG. The detection of EBER positivity via TBB highlighted its diagnostic value even when the incisional biopsy is inconclusive. Furthermore, transbronchial lung cryobiopsies can provide larger, higher-quality tissue samples [7], which may enhance the LYG diagnosis.
Cooccurrence of hematologic malignancies
This is the first reported case of WM developing after high-grade LYG, highlighting a potentially underrecognized association between these rare B-cell malignancies. Previous reports have described the development of LYG in patients with immunodeficiency disorders, such as Wiskott-Aldrich syndrome and acquired immunodeficiency syndrome [8,9]. Several LYG cases also developed secondary to multiple myeloma, T-cell large granular lymphocytic leukemia, and chronic lymphocytic leukemia [10-13]. These findings demonstrate that the pathogenesis arises from defective immune surveillance. To better highlight the rarity and clinical significance of our case, previously reported cases of LYG associated with other hematologic malignancies have been summarized in Table 2.
This comparison highlights the unique sequence and diagnostic complexity of the present case. In the present case, however, immunodeficiency in the patient was not evident. Although the risk of developing LPL/WM increases after developing LYG or administering immunochemotherapy remains unknown [4], two hypotheses were considered: (1) a shared tumorigenic origin and (2) LPL/WM emergence secondary to immunosuppression. Although the absence of elevated IgM levels and EBER positivity at LYG onset might be evidentiary against a shared etiology, favoring the latter hypothesis, we could not perform genetic analysis to support this hypothesis. This highlights a major limitation of this study, indicating the need for further molecular studies to elucidate the mechanisms underlying this lymphomagenesis.
Therapeutic challenges
While the patient achieved CR after R-CHOP, BR was ineffective against early-stage recurrent LYG despite demonstrating some efficacy against LPL/WM. Recent evidence indicates that dose-adjusted-EPOCH-R (etoposide, prednisone, vincristine, cyclophosphamide, doxorubicin, and rituximab) is a promising first-line therapy for high-grade LYG [21]. However, an effective regimen has not yet been established for refractory/relapsed cases. To date, only two cases of LYG treated with bendamustine have been documented. However, these cases were treated by brentuximab-vedotin combination therapy. No cases treated with BR therapy have been reported [22,23]. These studies indicate that unregulated immune control of EBV may contribute to disease relapse after chemotherapy, signifying the critical need for novel immunotherapies, including programmed cell death protein-1 blockade. The results of the ongoing prospective study will be of interest (Clinical Trials number: NCT03258567).
Conclusions
This case illustrates an exceptionally rare clinical trajectory in which LPL/WM developed sequentially after high-grade LYG. The diagnostic complexity presented in this case due to overlapping clinical features, evolving histopathological findings, and limitations in biopsy sampling emphasizes the importance of comprehensive and multidimensional diagnostic approaches. Furthermore, the treatment course highlights the therapeutic challenges in managing relapsed LYG, for which standardized regimens are lacking. Although the coexistence or sequential development of these rare B-cell malignancies is extremely uncommon, this case underscores the importance of long-term surveillance and consideration of secondary hematologic malignancies in patients with EBV-associated lymphoproliferative disorders. Future research is warranted to elucidate the underlying pathogenesis and to develop more effective therapeutic strategies.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Lymphomatoid granulomatosis Hum Pathol Liebow AA Carrington CR Friedman PJ 45755831972463896610.1016/s 0046-8177(72)80005-4 · doi ↗ · pubmed ↗
- 2Pathobiology and treatment of lymphomatoid granulomatosis, a rare EBV-driven disorder Blood Melani C Jaffe ES Wilson WH 1344135213520203210753910.1182/blood.2019000933 PMC 7162687 · doi ↗ · pubmed ↗
- 3Lymphomatoid granulomatosis: a single institution experience and review of the literature Clin Lymphoma Myeloma Leuk Chavez JC Sandoval-Sus J Horna P 0416 Suppl 201610.1016/j.clml.2016.02.02427521314 · doi ↗ · pubmed ↗
- 4The epidemiology of Waldenström macroglobulinemia Semin Hematol Mc Master ML 65726020233709903210.1053/j.seminhematol.2023.03.008PMC 10351685 · doi ↗ · pubmed ↗
- 5Lymphomatoid granulomatosis--a single institute experience: pathologic findings and clinical correlations Am J Surg Pathol Song JY Pittaluga S Dunleavy K 1411563920152532132710.1097/PAS.0000000000000328 PMC 4293220 · doi ↗ · pubmed ↗
- 6Histological comparison between preoperative and surgical specimens of non-small cell lung cancer for distinguishing between "squamous" and "non-squamous" cell carcinoma Diagn Pathol Yamagishi T Shimizu K Ochi N 103920142488516910.1186/1746-1596-9-103PMC 4099154 · doi ↗ · pubmed ↗
- 7Comparison of transbronchial and cryobiopsies in evaluation of diffuse parenchymal lung disease J Bronchology Interv Pulmonol Ramaswamy A Homer R Killam J Pisani MA Murphy TE Araujo K Puchalski J 14212320162670500710.1097/LBR.0000000000000246 PMC 4864578 · doi ↗ · pubmed ↗
- 8Pulmonary lymphomatoid granulomatosis in acquired immunodeficiency syndrome: lesions with Epstein-Barr virus infection Mod Pathol Haque AK Myers JL Hudnall SD Gelman BB Lloyd RV Payne D Borucki M 347356111998 https://pubmed.ncbi.nlm.nih.gov/9578085/9578085 · pubmed ↗