A Web-Based Tool to Perform a Values Clarification for Stroke Prevention in Patients With Atrial Fibrillation: Design and Preliminary Testing Study
Michael P Dorsch, Allen J Flynn, Kaitlyn M Greer, Sabah Ganai, Geoffrey D Barnes, Brian Zikmund-Fisher

TL;DR
A web-based tool was developed to help patients with atrial fibrillation understand the risks and benefits of anticoagulation for stroke prevention.
Contribution
The study introduces a values clarification exercise combined with visual aids to improve decision-making in stroke prevention for atrial fibrillation.
Findings
Visual aids modestly increased decision confidence compared to standard text-based information.
Participants in visual groups were less likely to choose anticoagulation and perceived smaller stroke risk reduction.
Gauge and icon array visualizations showed no significant difference in decision confidence but differed in perceived risk reduction.
Abstract
Atrial fibrillation (AF) is associated with an increased risk of stroke. Oral anticoagulation (OAC) is used for stroke prevention in AF, but it also increases bleeding risk. Clinical guidelines do not definitively recommend for or against OAC for patients with borderline stroke risk. Decision-making may benefit from values clarification exercises to communicate risk trade-offs. This study aimed to evaluate if a visual with a values clarification alters the understanding of the trade-offs of anticoagulation in AF. Participants aged 45‐64 years were recruited across the United States via an online survey. While answering the survey, they were asked to imagine they were newly diagnosed with AF with a CHA2DS2-VASc (congestive heart failure; hypertension; age ≥75 years [doubled]; type 2 diabetes; previous stroke, transient ischemic attack, or thromboembolism [doubled]; vascular disease;…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
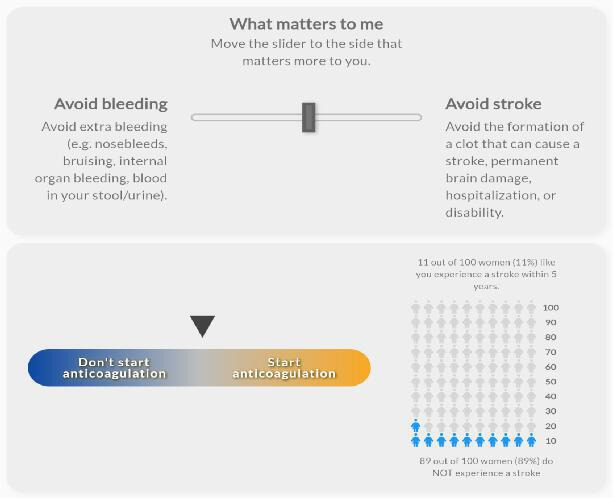 Figure 1
Figure 1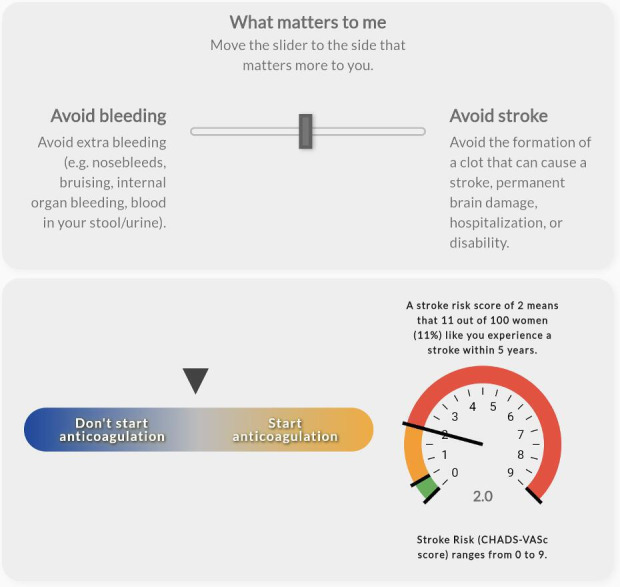 Figure 2
Figure 2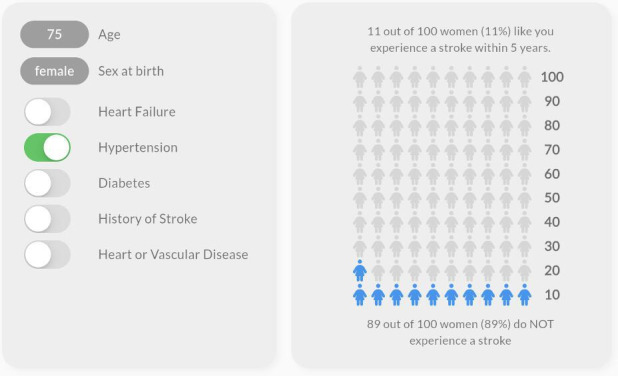 Figure 3
Figure 3 Figure 4
Figure 4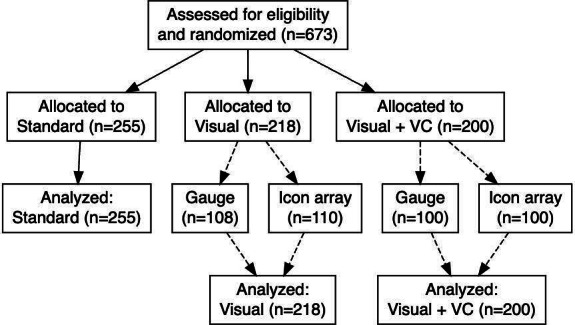 Figure 5
Figure 5| Variable | Standard (n=255) | Visual (n=218) | Visual+VC (n=200) | |
|---|---|---|---|---|
| Age (years), mean (SD) | 54.4 (5.8) | 54.5 (5.8) | 54.3 (6.1) | .93 |
| Sex (female), n (%) | 128 (50.2) | 102 (46.8) | 97 (48.5) | .76 |
| Race, n (%) | .55 | |||
| Black | 34 (13.3) | 27 (12.4) | 26 (13) | |
| Other | 29 (11.4) | 21 (9.6) | 24 (12) | |
| White | 192 (75.3) | 170 (78) | 150 (75) | |
| Hispanic or Latino, n (%) | 55 (21.5) | 44 (20.2) | 24 (12) | .02 |
| Self-rated health status, n (%) | .68 | |||
| Poor | 4 (1.6) | 8 (3.7) | 7 (3.5) | |
| Fair | 40 (15.7) | 43 (19.7) | 34 (17) | |
| Good | 126 (49.4) | 104 (47.7) | 90 (45) | |
| Very good | 66 (25.6) | 51 (23.4) | 57 (28.5) | |
| Excellent | 19 (7.5) | 12 (5.5) | 12 (6) | |
| Seen an HCP | 196 (76.9) | 162 (74.3) | 156 (78) | .66 |
| Prescription insurance, n (%) | 210 (82.4) | 177 (81.2) | 164 (82) | .95 |
| Knows someone with AFib | 61 (23.9) | 64 (29.4) | 61 (30.5) | .23 |
| Knows someone taking an OAC | 115 (45.1) | 103 (47.3) | 103 (51.5) | .39 |
| Confidence filling out forms, n (%) | .24 | |||
| Never | 6 (2.4) | 3 (1.4) | 1 (0.5) | |
| Occasionally | 0 (0) | 5 (2.3) | 2 (1) | |
| Sometimes | 18 (7.1) | 11 (5.1) | 10 (5) | |
| Often | 42 (16.5) | 39 (17.9) | 40 (20) | |
| Always | 189 (74.1) | 160 (73.4) | 147 (73.5) | |
| Help reading, n (%) | 102 (40) | 74 (33.9) | 87 (43.5) | .13 |
| Problems reading, n (%) | 101 (39.6) | 77 (35.2) | 77 (38.5) | .62 |
| Variable | Standard, n (%) | Visual, n (%) | Visual+VC, n (%) | OR |
|---|---|---|---|---|
| Yes to all 4 SURE questions | 156 (61.2) | 145 (66.5) | 134 (67) |
Visual versus No Visual: 1.26 (0.86‐1.84); Visual+VC versus No Visual: 1.29 (0.87‐1.90); |
| Do you feel SURE about the best choice for you? Yes | 191 (74.9) | 180 (82.6) | 163 (81.5) |
Visual versus No Visual: 1.59 (1.01‐2.49); Visual+VC versus No Visual: 1.48 (0.94‐2.33); |
| Do you know the benefits and risks of each option? Yes | 224 (87.8) | 193 (88.5) | 179 (89.5) |
Visual versus No Visual: 1.07 (0.61‐1.87); Visual+VC versus No Visual 1.18 (0.66‐2.12); |
| Are you clear about which benefits and risks matter most to you? Yes | 225 (88.2) | 185 (84.9) | 173 (86.5) |
Visual versus No Visual: 0.75 (0.44‐1.27); Visual+VC versus No Visual: 0.85 (0.49‐1.49); |
| Do you have enough support and advice to make a choice? Yes | 189 (74.1) | 167 (76.6) | 151 (75.5) |
Visual versus No Visual: 1.14 (0.75‐1.74); Visual + VC versus No Visual: 1.08 (0.70‐1.65); |
| Variable | Standard, mean (SD) | Visual, mean (SD) | Visual+VC, mean (SD) | |
|---|---|---|---|---|
| Based on how you feel about this decision right now, would you say you will choose to: | 58.3 (30.0) | 51.4 (32.0) | 51.9 (28.0) | .03 |
| How much of a reduction would anticoagulation make to your risk of stroke in AFib | 63.8 (22.0) | 54.2 (28.0) | 58.6 (25.0) | <.001 |
| How important is anticoagulation for stroke prevention in AFib? 0=Not important, 100=Extremely important | 75.6 (18.0) | 75.7 (19.0) | 73.9 (16.0) | .55 |
| How worried would you be about bleeding if you took anticoagulation for stroke prevention in AFib? 0=Not worried, 100=Extremely worried | 64.3 (24.0) | 65.2 (25.0) | 63 (23.0) | .63 |
| How worried would you be about having a stroke if you did NOT take anticoagulation? 0=Not worried, 100=Extremely worried | 66.3 (26.0) | 63 (28.0) | 62.1 (26.0) | .21 |
| Variable | Gauge (n=208), mean (SD) | Icon array (n=210), mean (SD) | |
|---|---|---|---|
| Based on how you feel about this decision right now, would you say you will choose to: 0=Do not take OAC, 100=Take OAC | 48.8 (31.0) | 55.4 (30.0) | .03 |
| How much of a reduction would anticoagulation make to your risk of stroke in AFib | 52.1 (27.0) | 60.4 (25.0) | .001 |
| How important is anticoagulation for stroke prevention in AFib? 0=Not important, 100=Extremely important | 74.6 (17.0) | 75.1 (18.0) | .76 |
| How worried would you be about bleeding if you took anticoagulation for stroke prevention in AFib? 0=Not worried, 100=Extremely worried | 64.5 (24.0) | 63.7 (24.0) | .73 |
| How worried would you be about having a stroke if you did NOT take anticoagulation? 0=Not worried, 100=Extremely worried | 60.5 (27.0) | 64.7 (27.0) | .11 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAtrial Fibrillation Management and Outcomes · Acute Ischemic Stroke Management · Health Systems, Economic Evaluations, Quality of Life
Introduction
Risk stratification and shared decision-making are essential in stroke prevention in atrial fibrillation (SPAF). In a wide variety of patients with AF, anticoagulation reduces the risk of ischemic stroke by 65% with a relative 2-fold increase in major extracranial bleeding compared to placebo [1-3]. Yet, medication responses vary across patients. Personalized risks and benefits are available to clinicians via the CHA_2_DS_2_-VASc (congestive heart failure; hypertension; age ≥75 years [doubled]; type 2 diabetes; previous stroke, transient ischemic attack, or thromboembolism [doubled]; vascular disease; age 65 to 75 years; and sex category) and HAS-BLED (hypertension, abnormal renal/liver function, stroke, bleeding history or predisposition, labile international normalized ratio, elderly [>65 years], drugs/alcohol concomitantly) risk scoring systems, representing the risk of stroke and bleeding in AF [4-6]. These tools can provide a tailored estimate of a patient’s benefit and risk of anticoagulation in AF.
Many current AF-shared decision-making tools use visual tools such as icon arrays to display the percent risk of stroke (CHA_2_DS_2_-VASc) and risk of bleed (HAS-BLED). While such tools help convey probabilities to patients [7], such probability-focused communications do not visually distinguish between different outcomes. This is a problem because it may lead patients and clinicians to give similar weight to these outcomes even though the medical complications of a stroke are far greater than the medical complications of a bleed. AF guidelines indicate that for the majority of patients where anticoagulation is recommended (CHA_2_DS_2_-VASc ≥2), the HAS-BLED is best used to remove or treat risk factors for bleeding (eg, stop concomitant aspirin or nonsteroidal anti-inflammatory drugs and treat hypertension) rather than to determine if anticoagulation should or should not be given.
One approach to encouraging more thoughtful consideration of the different possible outcomes of AF is using values clarification exercises [3]. Values clarification exercises are structured activities that encourage people to consider how much subjective weight they place on different possible outcomes [8-10]. For many years, developers of patient decision aids have encouraged the inclusion of values clarification exercises in such tools to increase the alignment of medical decisions with patient preferences. However, there is limited evidence on the comparative effectiveness of these different formats in the context of oral anticoagulation (OAC) decision-making in AF.
We report the results of a multistep design and evaluation process to explore the potential for integrating values clarification exercise–derived patient values into presentations of the risks and benefits of anticoagulant therapy. We based our work on the Ottawa Decision Support Framework (ODSF), an evidence-based midrange theory guiding patients’ health decisions [1112]. The framework is based on concepts from psychology, decision analysis, and decision conflict to evaluate the quality of outcomes in providing decision support. In this project, we engaged patients and providers in the user-centered design of a decision support tool for anticoagulation in AF (ODSF step 1), built the technology to deliver this tailored decision support tool (ODSF step 2), and tested if the decision support tool with a values clarification improves the knowledge of the trade-offs of anticoagulation in AF (ODSF step 3).
Methods
Study Design
We used a user-centered design to develop the decision support tool. For the user-centered design, we conducted an iterative series of user experience interviews with adults recruited from the general population, medical providers, and patient-provider dyads. We recruited participants from the general Ann Arbor, Michigan, population participants during February or March 2020 (first round), April 2020 (second round), and May 2020 (third round). In addition to these general patient interviews, we interviewed 6 providers and performed 2 patient-provider dyad interviews. These patient interviews were conducted virtually due to the COVID-19 pandemic.
After completing the design of the decision support tool, we performed a randomized controlled trial using a sample of adults recruited from across the United States using a panel managed by the online survey company Qualtrics. Participants were eligible if they were 45 to 64 years old, had not been diagnosed with AF, and had not taken anticoagulants.
The Qualtrics-administered survey asked participants to imagine themselves as a patient diagnosed with AF and hypertension, which made the imaginary patient a CHA_2_DS_2_-VASc score of 1 for men and 2 for women. This was chosen because using anticoagulation in those patients is not definitive in the guidelines, and patients may need decisional support [1]. All participants then received text-based education about AF, stroke risk in AF, and the need for anticoagulation. Following the education, we randomized patients to receive no visual (standard group), a visual representation of relevant probabilities of risk of stroke in AF (visual group), or to the new decision support tool that combined design-tailored visual displays with a values clarification (visual+VC group). The survey provider performed the randomization. Quotas were used to ensure adequate sex (50% female), race (maximum of 62.3% White), and ethnicity (minimum of 12.4% not Hispanic or Latino) across all groups. Randomization was done until those quotas were met, which led to more than 200 participants in each group.
The values clarification group was presented with an exercise to evaluate which health event matters more to them: avoiding bleeding or stroke. This values clarification exercise altered the recommendation to “start anticoagulation” or “don’t start anticoagulation” based on a slider movement between the 2 health events. As the user moved the slider toward avoiding a stroke, the pointer moved toward the recommendation to “start anticoagulation.” As the user moved the slider toward avoiding bleeding, the pointer moved toward the recommendation to “don’t start anticoagulation.” In addition, those randomized to the visual or visual+VC group were subrandomized to receive either a gauge display showing the CHA_2_DS_2_-VASc score or an icon array representing the individual’s probability of experiencing a stroke using a person icon [7]. The individuals’ probability of experiencing a stroke did not change during the values clarification exercise. Figures14 display examples of the 4 visualizations. Participants were also asked several questions to capture baseline characteristics. The complete survey, including consent, patient scenario, educational content, and questions, is available in Multimedia Appendix 1.
Example visualization of values clarification with icon array for a 75-year-old female with hypertension.
Example visualization of values clarification with gauge for a 75-year-old female with hypertension.
Example visualization with icon array for a 75-year-old female with hypertension.
Example visualization with gauge for a 75-year-old female with hypertension.
Outcomes
Participants completed the SURE (Sure of Myself; Understand Information; Risk-Benefit Ratio; Encouragement) screening test, which assesses the conflict a person has when making a decision [13]. The SURE test was used to understand if the participants in this study felt comfortable with their own decision to take or not take an OAC after reviewing the standard education or visuals. This was the primary outcome of this randomized trial [14]. The four yes-or-no questions are: (1) Do you feel SURE about the best choice for you? (2) Do you know the benefits and risks of each option? (3) Are you clear about which benefits and risks matter most to you? (4) Do you have enough support and advice to make a choice? Patient comfort was assessed as the percentage of participants answering yes to all the questions. Additionally, we measured anticoagulation intentions by the question: “Based on how you feel about this decision right now, would you say you will choose to,” with anchors, “Definitely TAKE an anticoagulant,” (100) on the right of the scale and, “Definitely NOT take an anticoagulant,” (0) on the left.
Secondary outcomes were questions about the participants’ understanding of anticoagulation for SPAF. The questions were: (1) How much of a reduction would anticoagulation make to your risk of stroke in AF? (0 to 100 scale: 0=Very small to 100=Very large); (2) How important is anticoagulation for SPAF? (0 to 100 scale: 0=Not at all important to 100=Very important); (3) How worried would you be about bleeding if you took anticoagulation for SPAF? (0 to 100 scale: Not at all worried to Very worried); and (4) How worried would you be about having a stroke if you did NOT take anticoagulation? (0 to 100 scale: Not at all worried to Very worried).
Statistical Analysis
The study was powered to detect 10 percentage differences, for example, 50% of patients in the standard group versus 60% of patients in the visual group and 70% of patients in the visual+VC group answering “Yes” to all questions on the SURE test, the primary outcome. This was considered a clinically meaningful difference between experimental groups. A total sample size of 480 survey participants (160 in each group) provided greater than 90% power to detect such a difference using a chi-square test. We set our recruitment goal for this study at 200 participants in each arm to account for variation in the estimates. The SURE test was reported as a percent of participants answering “Yes” as the numerator and the total number of participants as the denominator. The secondary outcome questions were analyzed using an analysis of variance and reported as a mean and SD of the scale in each group.
Ethical Considerations
This study was determined to be exempt by the University of Michigan Institutional Review Board (HUM00183776). Participants consented to participate in the survey study. Completed questionnaires were collected anonymously, and the data were deidentified. The service provider, Qualtrics, was paid for each participant that completed the survey. Compensation was provided by the service provider to the participants in the study.
Results
Baseline Characteristics
We recruited a total of 673 participants who completed the survey and were randomized to receive standard written communication (standard group), a visual representation of relevant probabilities (visual group), or the new decision support tool that combines design-tailored visual displays with values clarification (visual+VC group). Participant enrollment and allocation are summarized in the flow diagram (Figure 5). The average age was 54 (SD 6) years, and about half of the participants in the survey were female. Table 1 shows more detailed baseline demographics of the participants.
Flow diagram for patient enrollment, randomization, and analysis.
SURE Test Results
The overall SURE test, saying “yes” to all 4 components, was 61.2% (156/255) for the standard group, 66.5% (145/218) for the visual group, and 67% (134/200) for the visual+VC group (visual vs standard, odds ratio [OR] 1.26, 95% CI 0.86‐1.84; P=.23; visual+VC vs standard, OR 1.29, 95% CI 0.87‐1.90; P=.20). In exploratory analyses of each question, participants felt more sure about the best choice for them, question 1 of the SURE test, if they were presented with either visual compared to standard education (visual vs standard, OR 1.59, 95% CI 1.01‐2.49; P=.04; visual+VC vs standard, OR 1.48, 95% CI 0.94‐2.33; P=.09). Table 2 shows the overall SURE test and the individual components.
Participants were less likely to choose to take an OAC when shown either visual compared to standard education. The average rating was 58.3 (SD 30) in the standard group, 51.4 (SD 32) in the visual group, and 51.9 (SD 28) in the visual+VC group (P=.03). Participants also felt that the reduction in stroke risk from an OAC was less in either visual group than in the standard education group. The average rating was 63.8 (SD 22) in the standard group, 54.2 (SD 28) in the visual group, and 58.6 (SD 25) in the visual+VC group (P<.001). Table 3 demonstrates more detail on the questions about choosing OAC and stroke risk.
No significant differences were found between the visualization methods, gauge, and icon array for the outcome of the SURE test. Participants answered “yes” to all 4 SURE test questions, 65.9% (137/208) when shown a gauge and 67.6% (142/210) when shown an icon array group (P=.70). Participants were less likely to choose to take an OAC when shown a gauge compared to an icon array (mean 48.8, SD 31 vs mean 55.4, SD 30; P=.03). Participants also felt that the reduction in stroke risk from an OAC was less when shown a gauge than an icon array (mean 52.1, SD 27 vs mean 60.4, SD 25; P=.001). Table 4 provides further details regarding choosing OAC and stroke risk by visualization method.
Discussion
Principal Results
This trial investigated the difference in participant preferences for OAC for SPAF after reviewing 3 different approaches, which included standard education (standard group), a visual representation of relevant probabilities of risk of stroke in AF (visual group), or the new decision support tool that combined design-tailored visual displays with a values clarification (visual+VC group). The visuals were created using a user-centered design approach with iterative feedback from patients and providers. These visuals are unique because of the addition of values clarification and because most current tools use a dot-based icon array to show stroke risk in AF [1516]. Each participant was given a scenario with a CHA_2_DS_2_-VASc risk score, and the guidelines do not expressly state whether a patient should be prescribed an OAC. The 3 strategies did not affect the participants’ comfort in deciding to take an OAC between study groups, measured by the SURE test.
Participants were less likely to take an OAC and felt that the reduction in stroke risk from an OAC was less when shown either the visual or visual VC compared to standard education. This is unique for the CHA_2_DS_2_-VASc score of 1 for men and 2 for women, which we showed participants. Since the guidelines do not recommend for or against OAC in this population, visuals like the ones in this study could persuade patients not to take OAC.
Interestingly, the values clarification visual did not demonstrate a difference in the participants’ comfort in taking an OAC compared to the other visual group. This could have been due to several factors. Based on patient feedback, we used a horizontal bar for the values clarification. Previous versions of the tool we created and those in the literature used a vertical bar to represent the values clarification [8]. The horizontal bar could have led to more confusion than vertical bars. Additionally, the participants in this study were older than those in other studies using values clarification. Older participants may need more in-person help with the visuals. This could have led to more confusion with the intent of the visuals.
Although not the study’s primary outcome, the 2 visual types, gauge or icon array, influenced the participants’ decision to take an OAC and changed their perception of the stroke risk reduction from an OAC compared to the person-based icon array. Showing risk with the gauge made participants less likely to take an OAC, and they felt that the reduction in stroke risk from an OAC was smaller than the icon array. A body of research demonstrates the value of icon arrays in risk communication [17-20]. This difference in risk demonstration in this study could be explained by the lower detail presented in the gauge compared to the icon array, which represents a matrix of icons showing the at-risk population. The more detailed icon array could have made it easier for participants to understand the estimated risk and decide to take an OAC.
Limitations
There are several limitations to this study. First, the tool is meant for a shared decision-making session with a patient and provider, but the survey was done with members of the general public. Second, the survey was conducted with the general public to decrease any bias the provider would add to the shared decision-making situation in the study. If this tool was implemented as shared decision-making with a provider, it could lead to a better understanding of the tool. Future research should investigate the use of the tool with a provider present to guide and educate the patient. Third, newer AF guidelines have been published since the time of the study’s completion. Although our methods and educational materials referred to earlier guidelines, the updated guidelines recognize a borderline stroke-risk threshold (eg, CHA₂DS₂-VASc of 1 for men or 2 for women) where shared decision-making remains a priority.
Conclusions
Overall, the study suggests visual aids can modestly affect decision confidence and perceptions regarding the benefits of anticoagulation therapy but do not significantly change overall decision certainty in a scenario where the guidelines do not recommend for or against the treatment. Future work should determine the role of a gauge versus icon array in visual aids for decision-making in SPAF.
Supplementary material
10.2196/67956Multimedia Appendix 1Qualtrics Survey.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Joglar JA Chung MK Armbruster AL et al 2023 ACC/AHA/ACCP/HRS guideline for the diagnosis and management of atrial fibrillation: a report of the American College of Cardiology/American Heart Association Joint Committee on clinical practice guidelines Circulation 01220241491 e 1e 156doi 10.1161/CIR.0000000000001193 Medline 38033089 PMC 11095842 · doi ↗ · pubmed ↗
- 2Hart RG Pearce LA Aguilar MI Meta-analysis: antithrombotic therapy to prevent stroke in patients who have nonvalvular atrial fibrillation Ann Intern Med Jun 19200714612857867 doi 10.7326/0003-4819-146-12-200706190-00007 Medline 17577005 · doi ↗ · pubmed ↗
- 3Noseworthy PA Brito JP Kunneman M et al Shared decision-making in atrial fibrillation: navigating complex issues in partnership with the patient J Interv Card Electrophysiol Nov 2019562159163 doi 10.1007/s 10840-018-0465-5Medline 30327992 PMC 7056296 · doi ↗ · pubmed ↗
- 4Lip GYH Frison L Halperin JL Lane DA Identifying patients at high risk for stroke despite anticoagulation: a comparison of contemporary stroke risk stratification schemes in an anticoagulated atrial fibrillation cohort Stroke Dec 2010411227312738 doi 10.1161/STROKEAHA.110.590257 Medline 20966417 · doi ↗ · pubmed ↗
- 5van den Ham HA Klungel OH Singer DE Leufkens HGM van Staa TP Comparative performance of ATRIA, CHADS 2, and CHA 2DS 2-VA Sc risk scores predicting stroke in patients with atrial fibrillation: results from a National Primary Care Database J Am Coll Cardiol Oct 272015661718511859 doi 10.1016/j.jacc.2015.08.033Medline 26493655 · doi ↗ · pubmed ↗
- 6Pisters R Lane DA Nieuwlaat R de Vos CB Crijns H Lip GYH A novel user-friendly score (HAS-BLED) to assess 1-year risk of major bleeding in patients with atrial fibrillation: the Euro Heart Survey Chest Nov 2010138510931100 doi 10.1378/chest.10-0134 Medline 20299623 · doi ↗ · pubmed ↗
- 7Zikmund-Fisher BJ Witteman HO Dickson M et al Blocks, ovals, or people? Icon type affects risk perceptions and recall of pictographs Med Decis Making 052014344443453 doi 10.1177/0272989 X 13511706 Medline 24246564 PMC 3991751 · doi ↗ · pubmed ↗
- 8Witteman HO Chipenda Dansokho S Exe N Dupuis A Provencher T Zikmund-Fisher BJ Risk communication, values clarification, and vaccination decisions Risk Anal Oct 2015351018011819 doi 10.1111/risa.12418 Medline 25996456 · doi ↗ · pubmed ↗