Catheter Misplacement Revealing Partial Anomalous Pulmonary Venous Return (PAPVR) in an Acute Kidney Injury Patient
Ramy Zughul, Ayham Asassfeh, Rajit Pahwa

TL;DR
A patient with acute kidney injury had a dialysis catheter mistakenly placed into an unusual blood vessel, revealing a rare heart condition.
Contribution
This case highlights the incidental detection of PAPVR during routine catheter placement in ICU settings.
Findings
Catheter misplacement revealed an anomalous left pulmonary vein in an ICU patient.
Imaging confirmed the rare condition of partial anomalous pulmonary venous return.
CVC misplacement into PAPVR is a rare but important complication in critical care.
Abstract
An 84-year-old patient, treated in the ICU for acute kidney injury complicating coronary artery bypass surgery, experienced an unusual event during dialysis catheter placement. First, venous blood was drawn while the catheter was inserted into the left internal jugular vein. Ultrasound confirmed the proper guidewire placement, and the dilator and catheter were inserted without difficulty. However, the blood returned from the catheter was unexpectedly bright, raising concerns for arterial placement. Transduced pressures were pulsatile, but levels were inconsistent with arterial positioning. A subsequent chest x-ray revealed the catheter extending into the left mediastinum, and CT imaging confirmed the catheter was inadvertently placed in an anomalous left pulmonary vein. Misplacement of central venous catheters (CVCs) into partial anomalous pulmonary venous return (PAPVR) has been…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
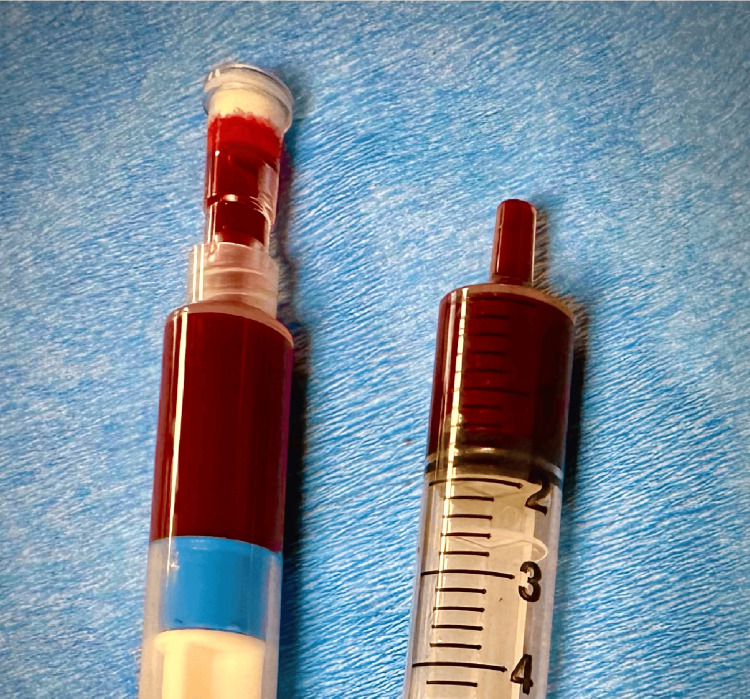 Figure 1
Figure 1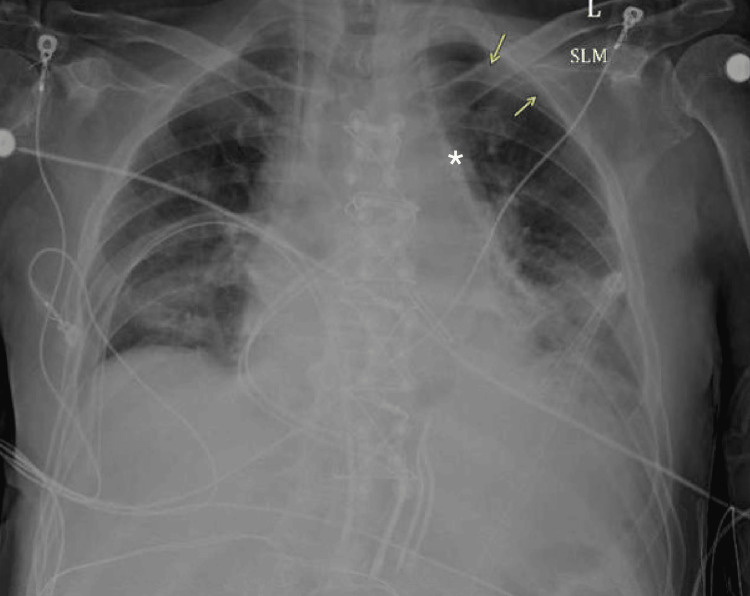 Figure 2
Figure 2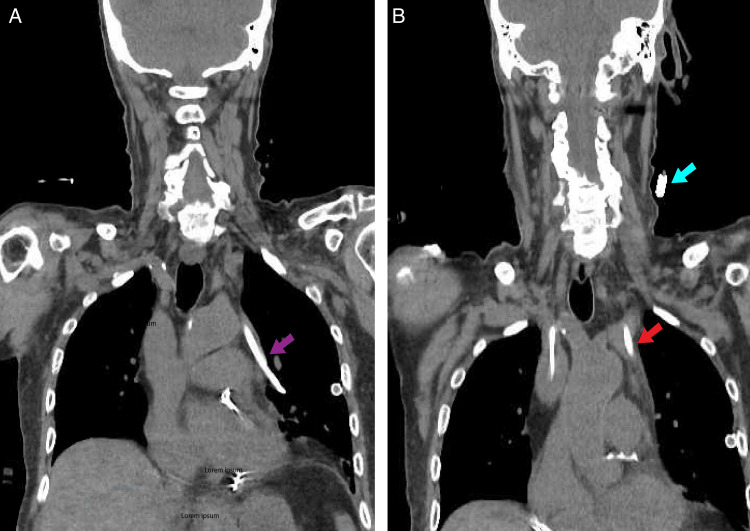 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCongenital Heart Disease Studies · Vascular anomalies and interventions · Ultrasound in Clinical Applications
Introduction
Central venous catheter (CVC) misplacement into an anomalous pulmonary vein is a rare but important clinical occurrence. CVC malpositioning is generally well-documented, with complications arising in approximately 6.7% of catheter placements, predominantly in left-sided approaches such as the internal jugular or subclavian veins [1]. A CVC is a flexible tube inserted into a large vein to deliver medications, fluids, or dialysis treatment, but improper placement can lead to serious complications.
Partial anomalous pulmonary venous return (PAPVR), a congenital heart defect with an incidence of 0.1%-0.4%, complicates CVC placement as the anomalous pulmonary vein may inadvertently be cannulated [2-5]. PAPVR occurs when one or more pulmonary veins that normally carry oxygenated blood from the lungs to the heart’s left atrium, instead drain into the wrong chamber (such as the right atrium) or a systemic vein. This abnormal blood flow, known as shunt flow, can increase strain on the heart and, if significant, contribute to pulmonary hypertension and heart failure over time [4,5]. While PAPVR is often asymptomatic and typically detected incidentally during imaging, its presence may lead to procedural complications during CVC placement, posing additional challenges in critically ill patients [6].
Case presentation
This 85-year-old male with a history of coronary artery disease and multiple comorbidities was admitted following a non-ST elevation myocardial infarction (NSTEMI) and underwent coronary artery bypass grafting (CABG) with a left internal mammary artery (LIMA) to the left anterior descending artery (LAD), a modified Maze procedure, and left atrial appendage ligation. His postoperative course was complicated by coagulopathy, respiratory failure requiring high-flow oxygen and bilevel positive airway pressure (BIPAP), worsening acute kidney injury (AKI) on chronic kidney disease (CKD), and atrial fibrillation with rapid ventricular response necessitating cardioversions and amiodarone therapy. Nephrology followed his AKI closely, with continuous renal replacement therapy (CRRT) considered but not initiated. Cardiovascular support was provided with dopamine and later epinephrine for blood pressure management, alongside aggressive diuresis to optimize renal function.
Nephrology was actively following the patient’s worsening renal function, and a decision was made to place a central line for potential CRRT, a continuous dialysis method used in critically ill patients to maintain hemodynamic stability. A non-tunneled dialysis catheter was attempted in the left internal jugular vein. The initial blood return from the needle was of venous color, and after confirmation of jugular guidewire placement with ultrasound, the dilator and dialysis catheter were inserted without difficulty. However, upon checking the catheter ports, the blood return appeared much brighter in color, raising concern for potential malpositioning (Figure 1). The catheter was transduced, showing pressures of 29/20, which were not suggestive of arterial placement. However, a plain chest x-ray revealed the catheter extending towards the left side of the mediastinum, raising suspicion of an anomalous vessel placement (Figure 2).
Difference in blood color between needle and catheter insertionsDark-colored venous blood seen on the right compared to bright blood color on the left.
Plain chest x-ray showing malposition of left internal jugular central venous catheter placementCentral venous catheter seen extending to left mediastinum (star). Small pneumothorax also present unchanged from before line placement (yellow arrows).
Subsequent non-contrast CT imaging of the neck and chest (Figures 3A, 3B) confirmed that the dialysis catheter had been inadvertently placed in an anomalous left upper lobe pulmonary vein which appears to be draining in the left brachiocephalic vein. There was a tiny left apical pneumothorax seen on previous imaging with bilateral chest tubes that were in place previously.
CT neck and chest without contrast showing central line visible in anomalous left upper lobe pulmonary vein CVC placed in partially anomalous pulmonary venous return (PAPVR)(A) CT imaging confirming the catheter was inadvertently placed in an anomalous left pulmonary vein (purple arrow). (B) The blue arrow showing proximal catheter entry point into a left internal jugular. The red arrow tracking the insertion of the pulmonary vein to the left innominate vein.CVC: Central venous catheter
Vascular surgery was consulted and recommended leaving the catheter in place and flushing it regularly to avoid further complications. Despite this rare complication, the patient remained hemodynamically stable, and there was no indication for immediate catheter removal. Over the following days, his respiratory and renal statuses improved, with weaning from inotropic support and high-flow oxygen. The patient was eventually discharged in stable condition to a skilled nursing facility for further rehabilitation, with follow-up planned for his multiple medical issues, including his pulmonary venous anomaly.
Discussion
PAPVR, first described by Winslow in 1739, results from persistent embryonic venous anastomosis [7]. During normal embryological development, pulmonary veins originate as a common pulmonary venous plexus that drains into the splanchnic venous system before establishing a definitive connection with the left atrium. Around the fourth to sixth weeks of gestation, the common pulmonary vein forms as an outgrowth of the left atrium and eventually absorbs the pulmonary venous plexus, allowing for direct drainage into the left atrium. Failure of this process, due to incomplete incorporation of the pulmonary veins or persistent embryologic venous connections, can lead to PAPVR. This anomaly occurs when one or more, but not all, pulmonary veins retain abnormal connections to systemic veins instead of fully integrating into the left atrium [8].
The most common PAPVR defect occurs on the right side, typically draining into the superior vena cava (SVC) [2-5]. Less commonly, it involves the left pulmonary vein, often with the left upper pulmonary vein draining into the innominate vein, as seen in our case. The majority of cases are asymptomatic, and patients can escape diagnosis.
Misplacement of CVCs into PAPVR-associated pulmonary veins has been sporadically reported, with most cases discovered via imaging post-procedure [9,10]. As imaging modalities such as CT and MRI become more commonplace in clinical practice, it is expected that both the diagnosis of PAPVR and incidental CVC misplacements will increase [10]. Despite being a rare event, this finding underscores the importance of careful evaluation when venous access complications arise, particularly in patients with undiagnosed congenital anomalies. Management typically involves the removal and repositioning of the catheter, though the decision to treat the PAPVR itself remains nuanced. The management approach is based on factors such as RV function, pulmonary hypertension risk, and shunt volume, and those who are at low risk can be managed conservatively [11,12].
Functional impairment, right ventricular (RV) enlargement, and a high shunt fraction (Qp/Qs >1.5) are the primary indications for surgical intervention (Class 1B) [5,13-15]. Patients requiring surgery were often reported to have multiple anomalous pulmonary veins and RV enlargement, aligning with previous observations that cardiac decompensation is unlikely when less than half of pulmonary venous return is anomalous, and the presence of multiple anomalous veins or increased left atrial pressure can lead to preferential right atrial shunting [15]. While pulmonary hypertension is common, especially in older patients, Pulmonary artery systolic pressure should be less than 50% of systemic pressure and pulmonary vascular resistance less than 30% of one-third of systemic resistance to be considered for surgery (Class 1B) [14]. This aligns with recommendations for closing other left-to-right shunts, such as atrial septal defects, to prevent severe RV dysfunction post-repair. Fortunately, when present, preoperative RV dysfunction is typically mild, and surgical outcomes are generally excellent [16].
Conclusions
This case underscores the importance of recognizing rare complications like CVC misplacement into an anomalous pulmonary vein and the need for exploring the approach to the incidental discovery of such anomalies. Identifying patients who may require further investigations or intervention.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Central venous catheter intravascular malpositioning: causes, prevention, diagnosis, and correction West J Emerg Med Roldan CJ Paniagua L 6586641620152658708710.5811/westjem.2015.7.26248 PMC 4644031 · doi ↗ · pubmed ↗
- 2Computed tomography of partial anomalous pulmonary venous connection in adults J Comput Assist Tomogr Haramati LB Moche IE Rivera VT 7437492720031450136510.1097/00004728-200309000-00011 · doi ↗ · pubmed ↗
- 3MDCT of partial anomalous pulmonary venous return (PAPVR) in adults J Thorac Imaging Ho ML Bhalla S Bierhals A Gutierrez F 89952420091946583010.1097/RTI.0b 013e 318194 c 942 · doi ↗ · pubmed ↗
- 4Clinical significance of partial anomalous pulmonary venous connections (isolated and atrial septal defect associated) determined by cardiovascular magnetic resonance Circ Cardiovasc Imaging Hatipoglu S Almogheer B Mahon C 014202110.1161/CIRCIMAGING.120.01237134384233 · doi ↗ · pubmed ↗
- 5Partial anomalous pulmonary venous return: a case series with management approach Respir Med Case Rep El-Kersh K Homsy E Daniels CJ Smith JS 1008332720193100804610.1016/j.rmcr.2019.100833 PMC 6456451 · doi ↗ · pubmed ↗
- 6Trends in use of medical imaging in US health care systems and in Ontario, Canada, 2000-2016 JAMA Smith-Bindman R Kwan ML Marlow EC 84385632220193147913610.1001/jama.2019.11456 PMC 6724186 · doi ↗ · pubmed ↗
- 7Partial anomalous pulmonary venous connection: diagnosis by transesophageal echocardiography J Am Coll Cardiol Ammash NM Seward JB Warnes CA Connolly HM O'Leary PW Danielson GK 13511358291997913723510.1016/s 0735-1097(97)82758-1 · doi ↗ · pubmed ↗
- 8Imaging of pulmonary venous developmental anomalies AJR Am J Roentgenol Dillman JR Yarram SG Hernandez RJ 1272128519220091938055210.2214/AJR.08.1526 · doi ↗ · pubmed ↗