From Petechiae to Intracerebral Hemorrhage: A Rare Progression of Pediatric Idiopathic Thrombocytopenia
Nirupam Nadella, Satwik Kuppili, Rhythm L Shukla, Korvi N Kumar, Adil M Siddiqui, Madhukar Madineni

TL;DR
A child with a rare blood disorder developed severe complications, including brain bleeding, highlighting the need for quick diagnosis and treatment.
Contribution
This case report highlights a rare progression from idiopathic thrombocytopenia to intracerebral hemorrhage in a pediatric patient.
Findings
The patient showed severe thrombocytopenia with giant platelets and abnormal megakaryocytes in bone marrow.
Despite treatment, the child developed intracerebral hemorrhage requiring emergency surgery.
The case underscores the importance of early detection and interdisciplinary care in such critical conditions.
Abstract
A four-year-old boy presented with a four-week history of hematuria, melena, and ecchymoses on his forehead, arm, and back, as well as upper respiratory symptoms. The physical examination revealed diffuse purpura on the lips, pallor, and several hyperpigmented spots. Laboratory results showed microcytic hypochromic anemia, neutropenia, lymphocytosis, and severe thrombocytopenia. A peripheral smear revealed giant platelets and a bone marrow biopsy revealed enhanced megakaryocytes with aberrant maturation. Despite the initiation of prednisolone medication, the patient experienced generalized tonic-clonic seizures and diminished consciousness (Glasgow Coma Scale: 4/15). Neuroimaging revealed a left-sided intracerebral hemorrhage with a midline shift, requiring an immediate decompressive craniotomy. Early detection and rapid interdisciplinary management are critical for improving outcomes…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1 Figure 2
Figure 2 Figure 3
Figure 3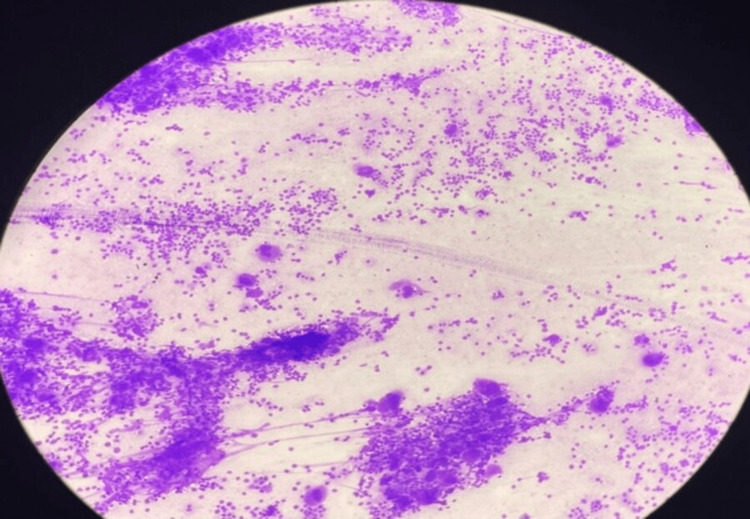 Figure 4
Figure 4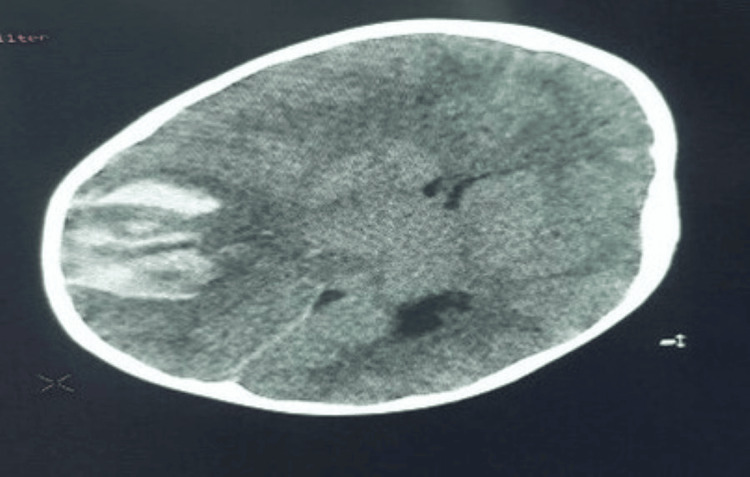 Figure 5
Figure 5Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPlatelet Disorders and Treatments · Blood groups and transfusion · Heparin-Induced Thrombocytopenia and Thrombosis
Introduction
Thrombocytopenia is a platelet count of <150 × 10^9^ /L. Low platelets may result from reduced bone marrow production, increased destruction in the circulation (due to coagulopathic consumption, auto-antibodies, vasculopathy, or inflammation), hemodilution, or splenic sequestration [1]. Idiopathic thrombocytopenic purpura (ITP) is one of the most common causes of symptomatic thrombocytopenia in children [2,3], with an annual incidence of 1 to 6.4 cases per 100,000 children [2,4]. Hematoma, petechiae, mucous membrane bleeding, and other hemorrhagic manifestations of thrombocytopenia are the most common clinical symptoms [5,6].
Case presentation
A four-year-old male child presented with a four-week history of red-colored micturition and tarry stools. There was a history of recent cough and cold and black patches over the forehead, arm, and back, as shown in Figure 1, but there was no history of blood transfusion, jaundice, or similar complaints in the past. He had not been taking any medications that could precipitate ITP. On examination, he was afebrile with a blood pressure of 100/60mmHg. There was diffuse purpura on the lips, as shown in Figure 2, and ecchymosis but no rash. Pallor was present, and there were no retinal hemorrhages, gum bleeding, splenomegaly, or lymphadenopathy. Four hyperpigmented patches were over the forehead (4cm×3cm), left pinna (2cm×2cm), inner aspect of the right arm (4cm×5cm), and right lower flank just above the thigh (8cm×8cm), as shown in Figure 3.
Multiple Hyperpigmented Patches
Purpura on the Lips
Hyperpigmented Patches on the Thigh
Laboratory investigations revealed microcytic hypochromic anemia with neutropenia, lymphocytosis, and thrombocytopenia and a hemoglobin of 8.2 g/dl (reference value: >11 g/dL), white-blood count of 9100/ cumm (reference range: 5,000 to 15,000 per cumm), platelet count of 0.42 lakhs/cumm, and a reticulocyte count of 3.5% (reference range: 0.5% to 2.0%). Peripheral smear shows giant platelets. The prothrombin time, partial thromboplastin time, thrombin time, fibrinogen, fibrin monomers, and fibrin split products were normal. Serum ferritin and serum electrolytes were normal. An electroencephalogram, gallium scan of the abdomen, and chest X-ray were normal. The bone marrow aspirate and biopsy showed increased megakaryocytes with abnormal maturation, as shown in Figure 4. Platelet antibody levels were not performed because of the profound thrombocytopenia. The workup for the etiology of his thrombocytopenia, including auto-immune and microbiological serology, was entirely negative, and a diagnosis of acute ITP was made. Syrup. Phenylephrine-5mg + Chlorpheniramine-2mg 4ml/TID, Tab. Lansoprazole-1/2 tab/OD, Tab. Folic Acid-150µg/day and Syrup. Zincovit-5ml/OD were initiated. ITP validation led to the start of Tab. Prednisolone-10mg-BD.
Bone Marrow Aspirate and Biopsy Revealing Increased Megakaryocytes with Dysplastic Maturation
The child became drowsy and had generalized tonic-clonic seizures, with a Glasgow Coma Scale of 4/15. The pupils were dilated and not reactive to light. Treatment of status epilepticus started, and the child had decorticate rigidity. A non-contrast head CT was done, showing left-side intracerebral hemorrhage with a midline shift (Figure 5). The patient was referred to neurosurgery, where the neurosurgeon planned for a decompressive craniotomy.
Non-contrast Head CT Showing Left-Sided Intracerebral Hemorrhage with a Midline Shift
Discussion
The differential diagnosis for the case could include drug-induced immune thrombocytopenia, hemolytic uremic syndrome, Von Willebrand's disease, acute leukemia, and ITP. Clinical features like ecchymoses and hyperpigmented patches, the absence of splenomegaly, laboratory investigations revealing microcytic hypochromic anemia, and a decrease in platelet count with giant megakaryocytes led to the diagnosis of acute ITP with microcytic hypochromic anemia.
Idiopathic thrombocytopenia could be of two types, the acute and the chronic type, the acute type being more common in children from 2 to 6 years of age [7]. Most cases of Idiopathic thrombocytopenia are preceded by infections with a latent period of around two weeks before the onset of ecchymoses. Most infections are upper respiratory tract infections, particularly viral infections [8]. In a study by Lusher and Zuelzer on 152 children with thrombocytopenic purpura, 83.6% of individuals showed the presence of antecedent infections before purpura [8]. The most common presenting symptoms would be bleeding gums, bruises, petechiae, and nose bleeds. Cerebral hemorrhage is rare, but it is the most serious complication of thrombocytopenic purpura. Anemia is commonly associated with blood loss through nosebleeds and bleeding gums [8].
The laboratory findings show microcytic hypochromic anemia and thrombocytopenia, which is followed by rare cases of severe iron deficiency anemia. However, the expected serum ferritin levels in the biochemical findings make it back to being idiopathic. Anemia and thrombocytopenia might indicate severe bone marrow dysfunction [9]. Cerebral hemorrhage, as in this case, is very rare and indicates the severity of the disease. In a study conducted on 278 patients with thrombocytopenic purpura, only 19 (6.83%) progressed to cerebral hemorrhage. Out of the 19, 17 hemorrhages occurred in the first month of the disease and are associated with various spontaneous bleedings all over the body [8].
Thrombocytopenic purpura is generally treated with corticosteroids, intravenous immunoglobulins as the first line of therapy, and immunosuppressants as the second line. In progressed stages, surgical intervention may be required, and a splenectomy has to be done [10]. However, the usage of corticosteroids in cases of ITP has been controversial. It is suggested that steroid usage in the early stages might cause the rise of platelets in some patients and control hemorrhage in other patients whose platelet count remains low [8]. Schulman et al. suggested the infusion of fresh plasma to patients with idiopathic thrombocytopenia at a dose of 30ml per kg body weight [11], and this is currently being followed by many practitioners [8].
Conclusions
This case highlights the severity and unpredictable progression of acute ITP, particularly when complicated by intracerebral hemorrhage. While ITP is often a self-limiting condition in children, this case underscores the need for close monitoring and timely intervention, especially in patients presenting with severe thrombocytopenia and signs of systemic involvement. The rare occurrence of cerebral hemorrhage in ITP serves as a reminder that early detection, aggressive management, and multidisciplinary coordination are crucial to improving patient outcomes. Future research and clinical vigilance are necessary to refine treatment protocols and identify patients at risk for such severe complications.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Thrombocytopenia: the good, the bad and the ugly Clin Med (Lond) Ashworth I Thielemans L Chevassut T 2142172220223558482810.7861/clinmed.2022-0146 PMC 9135082 · doi ↗ · pubmed ↗
- 2ITP in children: pathophysiology and current treatment approaches J Pediatr Hematol Oncol D'Orazio JA Neely J Farhoudi N 1133520132307304510.1097/MPH.0b 013e 318271 f 457 · doi ↗ · pubmed ↗
- 3Idiopathic thrombocytopenic purpura in children: a 10 years experience at tertiary care hospital J Pak Med Assoc Alam MM 13581362642014 https://pubmed.ncbi.nlm.nih.gov/25842577/25842577 · pubmed ↗
- 4The incidence of immune thrombocytopenic purpura in children and adults: a critical review of published reports Am J Hematol Terrell DR Beebe LA Vesely SK Neas BR Segal JB George JN 1741808520102013130310.1002/ajh.21616 · doi ↗ · pubmed ↗
- 5Childhood idiopathic thrombocytopenic purpura: oral manifestations and dental care Int J Oral Dent Health Vasconcelos RB Vasconcelos GB do Nascimento MG Colares V 42018
- 6Assessment of UK practice for management of acute childhood idiopathic thrombocytopenic purpura against published guidelines Lancet Bolton-Maggs PH Moon I 6206233501997928804410.1016/s 0140-6736(97)04143-3 · doi ↗ · pubmed ↗
- 7Acute idiopathic thrombocytopenic purpura Oral Surg Oral Med Oral Pathol James WD Guiry CC Grote WR 149151571984660807810.1016/0030-4220(84)90202-0 · doi ↗ · pubmed ↗
- 8Idiopathic thrombocytopenic purpura in childhood J Pediatr Lusher JM Zuelzer WW 971979681966594901710.1016/s 0022-3476(66)80218-4 · doi ↗ · pubmed ↗