Aspergillus Spondylodiscitis in an Immunocompetent Patient With Recurrent Aspergillus Endocarditis; A Clinical Case Report
Mohsen Meidani, Maryam Moradi, Mehrzad Rahmanian, Mehrdad Salehi, Morteza Foroumandi, Farnoosh Larti, Neda Alijani, Hanieh Movahhed, Ensiyeh Rahimi, Fereshteh Ghiasvand

TL;DR
A case report describes a rare instance of Aspergillus endocarditis in an immunocompetent man, successfully treated with liposomal amphotericin B.
Contribution
This case highlights the occurrence of Aspergillus endocarditis in an immunocompetent individual and its successful treatment.
Findings
Aspergillus endocarditis occurred in an immunocompetent patient with multiple brain septic emboli and spondylodiscitis.
The patient responded successfully to treatment with liposomal amphotericin B.
Early recognition and appropriate treatment are critical for reducing mortality in Aspergillus endocarditis cases.
Abstract
Fungal endocarditis is a very uncommon and deadly illness that causes inflammation in the heart's lining, including the valves. Aspergillus endocarditis is the second most common cause of prosthetic endocarditis, especially the aortic valve, after Candida spp. Aspergillus endocarditis can occur on native and prosthetic valves, even in immunocompetent hosts. In this article, we describe a case of recurrent aortic-valve Aspergillus endocarditis occurring in a Caucasian man without previously known immunocompromised status with multiple brain septic emboli and spondylodiscitis. The patient was successfully responsive to liposomal amphotericin B. Early recognition in patients with underlying immunosuppressive conditions and immunocompetent hosts is critical to decreasing the mortality rate. Aspergillosis must be considered in every patient with a prior valve replacement history and…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
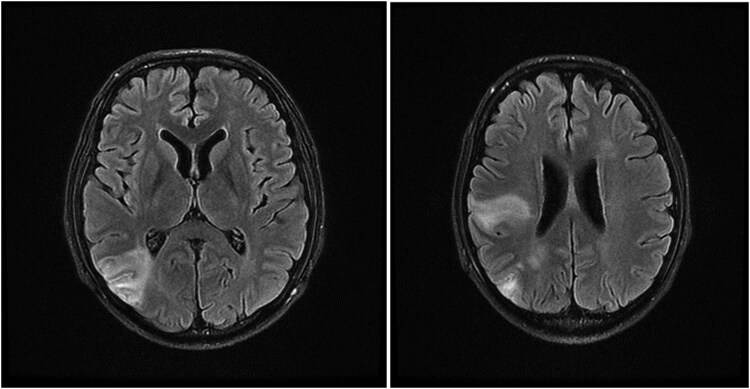 Figure 1
Figure 1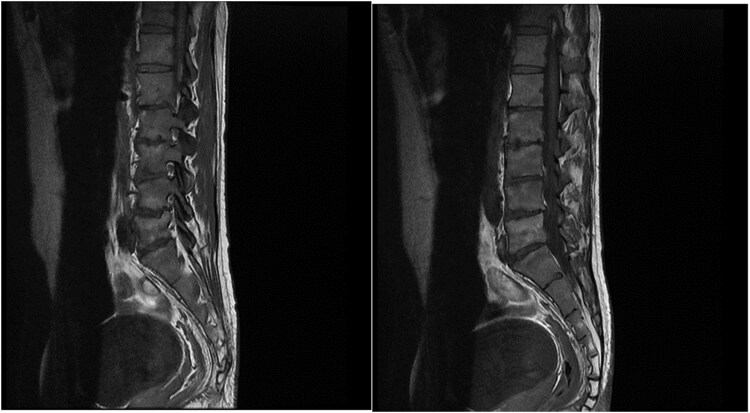 Figure 2
Figure 2| Date | Symptoms | Echocardiographic Findings | Outcome |
|---|---|---|---|
| August 2022 | No symptom (routine follow-up with echocardiogram) | Bicuspid aortic valve | Aortic valve replacement |
| November 2022 | Loss of appetite, weight loss, petechial lesions on arm and eyes | Aortic vegetation | Gram-negative cultured endocarditis (suspected fungal infection because of large vegetation but did not receive antifungal treatment) |
| May 2023 | Dyspnea, petechial lesions | Aortic vegetation | Culture of vegetation positive for |
| September 2023 | No symptoms (routine follow-up with echocardiogram) | Bioprosthetic aortic valve leakage, aortic large pseudoaneurysm, aortic vegetation | Positive polymerase chain reaction of vegetation for |
| Laboratory Test | Result | |
|---|---|---|
| Blood, urine, and endotracheal cultures | Negative | |
| Brucella (Wright, Coombs Wright, 2ME) | Negative | |
| Galactomannan | 4.69 (reference range: < 0.5 index) | |
| Immunologic panel | IgG | 1340 (normal range) |
| IgG1 | 523 (normal range) | |
| IgG2 | 292 (normal range) | |
| IgG3 | 89 (normal range) | |
| IgG4 | 72.5 mg/L (52–125 mg/L) | |
| IgM | 176 (37–286 mg/dL) | |
| IgA | 387 (60–400 mg/dL) | |
| C3 | 150 (75–175 mg/dL) | |
| C4 | 37 (16–48 mg/dL) | |
| CH50 | 120 (42–95 U/mL) | |
| NBT-DHR | Normal (3.5–52.1) | |
| Year | Gender | Age, y | Previous Cardiac Surgery | Embolization | Outcome |
|---|---|---|---|---|---|
| 1990 [ | Male | 74 | None | Hand | Alive |
| 2004 [ | Male | 34 | Subaortic membrane excision | Femoral artery | Dead |
| 2009 [ | Male | 49 | CABG | Aorta | Dead |
| 2016 [ | Male | 65 | None | None | Dead |
| 2019 [ | Female | 63 | CABG | Femoral artery | Alive |
| 2020 [ | Male | 49 | None | None | Alive |
| 2021 [ | Male | 49 | CABG | Spleen, CNS | Dead |
| 2023 [ | Male | 74 | None | CNS | Dead |
| 2023 (current study) | Male | 35 | Aortic valve replacement (4 times) | CNS | Alive |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAntifungal resistance and susceptibility · Infective Endocarditis Diagnosis and Management · Actinomycetales infections and treatment
Fungal endocarditis is a very uncommon and deadly illness that causes inflammation in the heart's lining, including the heart valves. Aspergillus endocarditis (AE) is the second most common cause of prosthetic endocarditis, especially the aortic valve, after Candida spp [1, 2].
The number of AE cases has gone up and is expected to increase even more because there are more invasive procedures, cardiac devices, prosthetic valves, and immune system suppressors being used. AE does not have many of the signs clinicians use to diagnose infective endocarditis, where the blood culture is usually negative and there may not be a fever. These complications lead to late diagnosis and proper treatment and a higher mortality rate [3].
In this article, we describe a case of recurrent aortic-valve Aspergillus endocarditis occurring in a Caucasian man without previously known immunocompromised status with multiple brain septic emboli and spondylodiscitis.
CASE PRESENTATION
In September 2023, an intubated 35-year-old Caucasian man with a history of previous multiple valve replacements was transferred from the cardiac surgery ward to the intensive care unit of Imam Khomeini Hospital, Tehran, Iran, presenting with a blood pressure drop and possible septic shock. A huge aortic valve vegetation was discovered in early evaluation upon cardiac ultrasonographic findings. Fungal polymerase chain reaction was positive for aspergillosis. At first, amikacin 1 g daily intravenously (IV), meropenem 2 g 3 times a day IV, Linezolid 600 2 times per day IV, voriconazole 200 mg twice per day, and amphotericin B liposomal (5 mg/kg) 400 mg IV daily, were ordered.
Regarding the patient’s medical history of the bicuspid aortic valve, he had had aortic valve replacement 4 times, with the last replacement on current admission based on echocardiographic findings. The echocardiograph revealed a shaggy semimobile mass of approximately (18 mm × 13 mm × 14 mm) attached to the aortic valve (suggestive of vegetation and an echo-free space of about 18 mm × 30 mm) in the posterior part of the aorta with extension to intervalvular fibrosa and to and fro flow suggestive of a pseudoaneurysm. Also, there was severe paravalvular leakage from the dehiscence part of the aortic valve leaflet and a large echo-free space of approximately 50 mm × 41 mm at the level of ascending aorta suggestive of abscess formation with compression effect on the superior vena cava (Supplementary Data). In the patient's medical history, a diagnosis of Aspergillus endocarditis was definite with the culture of Aspergillus flavus in vegetation; in a previous episode of endocarditis, treatment with voriconazole 200 mg twice daily was started for the patient about 6 months before this episode. His past surgical procedures are summarized in Table 1.
To complete the patient evaluation, blood, urine, endotracheal cultures, Brucella, serum galactomannan test, immunologic panel for primary immune deficiency, and abdominopelvic ultrasound were ordered. On abdominopelvic ultrasound, bilateral pleural effusion was seen; spleen and liver were intact without abscess formation. Rheumatologic tests including antinuclear antibody (ANA), and rheumatoid factor (RF) and HIV antibodies were negative. Other laboratory test results are summarized in Table 2.
The patient was extubated after proper antibiotic therapy and blood pressure rose. Forty-eight hours after extubation, the patient developed a fever again and became tachycardic. The physical examination was normal. A sepsis workup was done and because of the possibility of a low voriconazole level and failure of treatment, therapeutic drug monitoring (TDM) was requested and caspofungin 50 mg IV daily was added to the patient's treatment regimen. The dose of voriconazole raised to 400 mg twice per day. Results of blood and urine culture were negative, CXR and abdominal sonography were normal, and follow-up Echocardiographic did not reveal any vegetation or abscess formation. The TDM of voriconazole was reported 0.1 mcg/mL (normal range: 1–5.5 mcg/mL). Amikacin, meropenem, and linezolid were discontinued. Three days later, lower back pain and left paraesthesia were reported. Whole lumbosacral, spine, and brain magnetic resonance imaging (MRI) scans were done, respectively.
The brain MRI scan revealed subacute hemorrhagic infarction in the right inferior frontal lobe, right temporal lobe, and right centrum semiovale. These findings favor brain septic emboli after the patient's previous septic shock (Figure 1).
Patient's brain magnetic resonance imaging scan.
The lumbosacral MRI showed spondylodiscitis evidence, including low T1 and high T2 signal intensity in the vertebral bodies and the intervertebral disk between them; gadolinium enhancement on T1-weighted imaging in the affected tissues also were seen (Figure 2).
The patient's lumbosacral magnetic resonance imaging scan.
The TDM was in normal range after 2 weeks and signs and symptoms of back pain had significant improving. He did not need surgery. Amphotericin B liposomal and caspofungin were discontinued at the time of discharge after 2 weeks.
The patient was discharged from the hospital after 8 weeks of amphotericin therapy with an acceptable general condition, the following medication orders (voriconazole 400 mg twice per day with careful TDM), and a recommendation for regular follow-up by his cardiologist.
DISCUSSION
Aspergillus endocarditis is not common and usually occurs after previous heart surgery such as valve replacement. Approximately half of the patients with infectious endocarditis experience a complication called systemic embolization, where the infection spreads to other parts of the body, especially the brain. Multiple blood cultures and routine echocardiograms in patients with a history of cardiac surgery are the best ways to make a proper diagnosis [4].
In several studies, systemic embolization following AE has been reported. Aortic embolism, splenic infarction, and aortic stroke were reported in patients with AE [5, 6]. Our study detected multiple brain septic emboli on the patient's MRI scan after the fourth aortic valve replacement resulting from AE.
Invasive AE usually occurs in immunocompromised or drug-using patients. Posttransplant patients receiving high doses of corticosteroids or chemotherapy are most prone to developing AE. Most AEs are challenging to diagnose because of the negative blood culture and fever absence [1]. Immunocompetent patients are rarely diagnosed with AE. There have been several studies in which patients without any prior immunosuppressive condition or IV drug use had AE in their aortic valve even without any previous cardiac surgery. These cases, along with our patients, are summarized in Table 3.
In contrast to our study, Aspergillus spondylodiscitis was reported in immunocompromised patients following heart transplant, acute lymphoblastic leukemia, and hairy cell leukemia. Patients were treated with itraconazole, which was given as a single drug therapy or in combination with 5-flucytosine and amphotericin B. Surgical management was required in those who did not respond to medical treatment. Our report was the first immunocompetent patient with Aspergillus spondylodiscitis following AE [5, 6].
CONCLUSION
Aspergillus endocarditis can occur on native and prosthetic valves, even in immunocompetent hosts. Our patient did not have secondary immunodeficiency. He was tested for primary immunodeficiency (chronic granulomatous disease [CGD]/common variable immunodeficiency [CVID]) and the results were negative. The only risk factor was the patient's prosthetic valve. It is critical to consider aspergillosis in every patient with prior valve replacement history and culture-negative endocarditis. Surgical debridement and appropriate antifungal agents are required to solve the problem. Systemic embolization and Aspergillus discitis were also detected afterward in our case.
Supplementary Material
ofaf198_Supplementary_Data
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Chevalier K, Barde F, Benhamida S, et al Invasive aspergillosis and endocarditis. Rev Med Interne 2021; 42:678–85.34303547 10.1016/j.revmed.2021.07.001 · doi ↗ · pubmed ↗
- 2Caroselli C, Suardi LR, Besola L, Fiocco A, Colli A, Falcone M. Native-valve Aspergillus endocarditis: case report and literature review. Antibiotics 2023; 12.10.3390/antibiotics 12071190 PMC 1037602737508286 · doi ↗ · pubmed ↗
- 3Meshaal MS, Labib D, Said K, et al Aspergillus endocarditis: diagnostic criteria and predictors of outcome, a retrospective cohort study. P Lo S One 2018; 13:e 0201459.30092074 10.1371/journal.pone.0201459 PMC 6084895 · doi ↗ · pubmed ↗
- 4Aldosari MA, Alghamdi MH, Alhamdan AA, Alamri MM, Ahmed AM, Aziz MS. Native valve fungal endocarditis caused by Aspergillus fumigatus: management dilemma. Oxf Med Case Reports 2020; 2020:omz 147.32257253 10.1093/omcr/omz 147PMC 7104203 · doi ↗ · pubmed ↗
- 5Cortet B, Richard R, Deprez X, et al Aspergillus spondylodiscitis: successful conservative treatment in 9 cases. J Rheumatol 1994; 21:1287–91.7966071 · pubmed ↗
- 6Cortet B, Deprez X, Triki R, et al Aspergillus spondylodiscitis. Apropos of 5 cases. Rev Rhum Ed Fr 1993; 60:37–44.8242025 · pubmed ↗
- 7Bogner JR, Lüftl S, Middeke M, Spengel F. Successful drug therapy in Aspergillus endocarditis. Dtsch Med Wochenschr 1990; 115:1833–7.2245766 10.1055/s-2008-1065234 · doi ↗ · pubmed ↗
- 8Verghese S, Maria CF, Mullaseri AS, Asha M, Padmaja P, Padhye AA. Aspergillus endocarditis presenting as femoral artery embolism. Mycoses 2004; 47:252–6.15189195 10.1111/j.1439-0507.2004.00980.x · doi ↗ · pubmed ↗