Outcome Prediction by Combining Initial Clinical Severity With Corticospinal Tract Lesion Load in Patients With Intracerebral Hemorrhage
Toshiki Yasukawa, Yuki Uchiyama, Tetsuo Koyama, Kazuhisa Domen

TL;DR
This study shows that combining initial clinical severity and brain lesion load improves predictions of motor recovery in patients with brain hemorrhage.
Contribution
The novel contribution is integrating initial hemiparesis severity and corticospinal tract lesion load to predict motor outcomes in intracerebral hemorrhage patients.
Findings
Both initial hemiparesis severity and corticospinal tract lesion load significantly predict motor outcomes.
The regression model explained 60.4% of the variance in motor recovery outcomes.
Initial severity and lesion load contributed comparably to outcome predictions.
Abstract
Objective: This study aimed to assess the predictive accuracy of motor outcomes in patients with intracerebral hemorrhage by integrating the initial severity of hemiparesis and the corticospinal tract lesion load (CST-LL). Materials and methods: A retrospective analysis was conducted on patients diagnosed with putaminal and/or thalamic hemorrhage who underwent computed tomography (CT) shortly after stroke onset. The CT images were aligned with a standardized brain template to calculate CST-LL. The initial severity of hemiparesis was evaluated using the summed Brunnstrom Recovery Stage (BRS total; range: 3-18). Motor outcomes at the time of discharge from a rehabilitation facility were assessed using the motor component total score of the Stroke Impairment Assessment Set (SIAS-motor total; range: 0-25). A multivariate regression analysis was performed with BRS total and CST-LL as…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
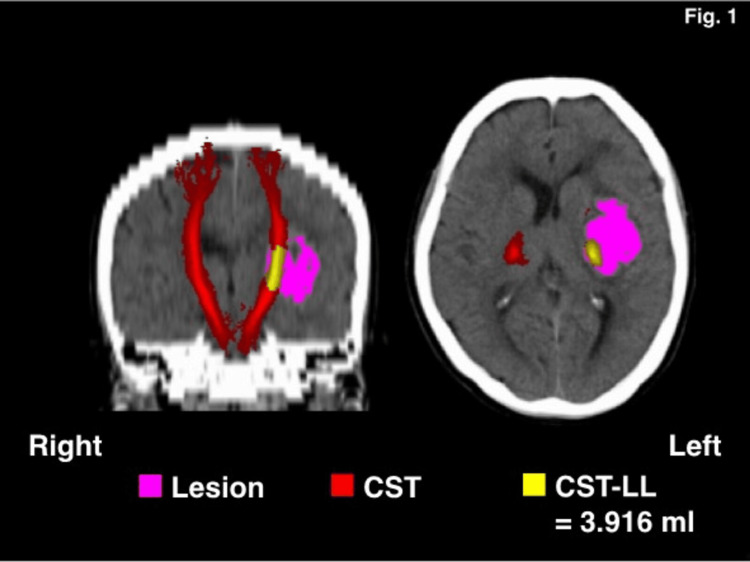 Figure 1
Figure 1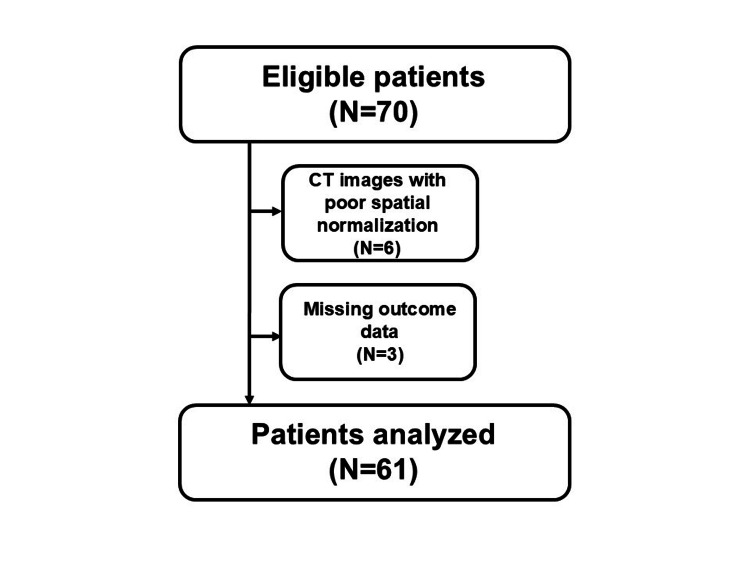 Figure 2
Figure 2| Demographic backgrounds | |
| Age (years) | Median 66 (IQR 57, 74.5; Range 44-89) |
| Gender (male/female) | 35/26 |
| Lesioned hemisphere (left/right) | 26/35 |
| CST-LL (mL) | 1.974 (IQR 1.113, 3.311; Range 0.002-7.595) |
| Clinical severity at admission | |
| BRS shoulder/elbow/forearm | Median 2 (IQR 1, 4; Range 1-6) |
| BRS hand/finger | Median 2 (IQR 1, 4; Range 1-6) |
| BRS lower extremity | Median 3 (IQR 2, 4.5; Range 1-6) |
| BRS total | Median 8 (IQR 4, 13; Range 3-18) |
| Outcome assessment | |
| SIAS-motor arm | Median 4 (IQR 2-5; Range 0-5) |
| SIAS-motor finger | Median 4 (IQR 1, 5; Range 0-5) |
| SIAS-motor hip | Median 4 (IQR 3, 5; Range 0-5) |
| SIAS-motor knee | Median 4 (IQR 3, 5; Range 0-5) |
| SIAS-motor ankle | Median 4 (IQR 1.5, 5; Range 0-5) |
| SIAS-motor total | Median 20 (IQR 9.5, 24.5; Range 0-25) |
| FIM-motor | Median 81 (IQR 67.5, 89; Range 15-91) |
| LOS | Median 108 (IQR 73, 152.5; Range, 31 - 257) |
| Variables | BRS total | SIAS-motor total |
| CST-LL | R=-0.697 (P<0.001) | R=-0.668 (P<0.001) |
| BRS total | - | R=0.745 (P<0.001) |
| Explanatory variable | SIAS-motor total | t | P | ||
| Estimate | S.E. | ||||
| CST-LL | -1.79 | 0.54 | -3.29 | 0.002 | |
| BRS total | 0.82 | 0.17 | 4.79 | <0.001 | |
| Intercept | 13.67 | 2.51 | 5.43 | <0.001 | |
| Adjusted R2 | 0.604 | <0.001 | |||
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsIntracerebral and Subarachnoid Hemorrhage Research · Acute Ischemic Stroke Management · Advanced Neuroimaging Techniques and Applications
Introduction
Predicting patient outcomes is crucial for planning effective rehabilitation strategies for individuals who have experienced a stroke [1]. Among the various factors influencing recovery, the severity of clinical symptoms in the early stages is particularly important, as it provides critical insights into stroke impact and guides therapeutic and rehabilitative interventions [2]. Therefore, assessing clinical manifestations during the acute phase is essential for predicting outcomes and determining appropriate management strategies in stroke rehabilitation.
Beyond initial clinical severity, the integrity of the corticospinal tract (CST) has been identified as a key factor in predicting functional outcomes, particularly motor recovery in the extremities [3,4]. Studies utilizing magnetic resonance imaging (MRI) have demonstrated that the overlap between the stroke lesion and the CST, known as CST lesion load (CST-LL), correlates with motor function outcomes [5,6]. In addition, computed tomography (CT), which is commonly used in stroke management, especially for hemorrhagic stroke, has been investigated as a potential tool for estimating CST-LL. Some reports suggest that CST-LL derived from CT imaging may aid in outcome prediction, particularly in cases involving putaminal or thalamic hemorrhage [7,8].
Various predictive models incorporating techniques such as machine learning and functional MRI have been developed to estimate stroke outcomes [9-11]. However, these methods often require significant computational resources and prolonged processing times, limiting their feasibility for routine clinical use. In contrast, integrating initial clinical severity assessment with CST-LL derived from standard CT scans offers a practical approach that can be readily implemented in daily clinical practice [8,12]. This study aims to evaluate the clinical utility of combining early clinical severity and CST-LL in predicting outcomes for patients with intracerebral hemorrhage.
Materials and methods
Patient selection
This retrospective study builds on our previous research investigating the clinical applicability of conventional CT imaging in stroke rehabilitation [8,12]. It included patients diagnosed with intracerebral hemorrhage who were admitted to Nishinomiya Kyoritsu Neurosurgical Hospital between April 2019 and March 2024. Upon admission, patients typically received conservative treatment, such as antihypertensive therapy, with surgical evacuation of hematomas performed when indicated [13]. Rehabilitation interventions, including physical, occupational, and speech therapy, were provided for up to 180 minutes daily, following the Japanese stroke management guidelines [13].
To minimize variability due to pre-stroke health status and lesion location, the study focused on individuals experiencing their first-ever stroke with hemorrhagic lesions in the putamen and/or thalamus who had been functionally independent in daily activities, including unassisted ambulation, prior to the stroke. Patients were excluded if they had a history of neurological disorders such as Parkinson’s or Alzheimer’s disease, exhibited progressive neurological deficits, or had significant comorbidities [12]. To ensure a consistent rehabilitation protocol, only patients subsequently transferred to Nishinomiya Kyoritsu Rehabilitation Hospital, an affiliated long-term rehabilitation facility, were included [12]. The study protocol was approved by the Ethics Committee of Hyogo College of Medicine (approval no. 4666), and informed consent was obtained using an opt-out approach.
CT imaging and processing
CT acquisition and image processing followed previously published methods by our research team [8,12]. Briefly, patients underwent a head CT scan upon admission when stroke was suspected. Imaging was performed using a 320-row detector CT scanner (Aquilion ONE, Canon Medical Systems Corp., Tochigi, Japan) with a standard helical acquisition protocol. Parameters included a tube voltage of 120 kVp, a current of 300 mAs, an in-plane resolution of 0.43 × 0.43 mm (512 × 512 matrix), and a slice thickness of 5 mm.
CT image processing was conducted using FMRIB Software Library (FSL) version 6.0.6 (FMRIB, Oxford, UK) for brain image analysis [14]. Images were thresholded within the Hounsfield unit (HU) range of 0-100 and spatially normalized to a standard CT template [7,8,12]. Spatial normalization accuracy was confirmed by visual inspection. A rectangular volume of interest (VOI) was defined for each patient, encompassing the hematoma in the x, y, and z planes. A lesion mask was created by extracting and binarizing voxels within the VOI that exceeded 50% of the HU threshold [8,12].
The CSTs in both hemispheres were delineated using the JHU-ICBM-tracts-maxprob-thr0-1mm.nii.gz template from the FMRIB Software Library and mapped onto CT images aligned to the standard brain space [15]. CST-LL was determined by identifying overlapping voxels between the CST and the lesion mask. The total volume of overlapping CST-LL voxels (in milliliters) was calculated for each patient (see Figure 1) [8,12].
Representative computed tomography images of the brain after spatial registration to a standard brain. CST, corticospinal tract; LL, lesion load.
Clinical assessments
Motor impairment severity at admission was assessed using the Brunnstrom Recovery Stage (BRS) [16], which evaluates upper limb function (proximal: shoulder, elbow, forearm; distal: hand, fingers) and lower limb function on the affected side. Each component is rated on a six-point scale (1-6). The total BRS score (BRS total) was calculated by summing the individual component scores, providing an overall measure of hemiparesis severity [17].
To evaluate motor function in both the upper and lower limbs, the Stroke Impairment Assessment Set motor subscale (SIAS-motor) was used [18]. This assessment consists of five domains (arm, finger, hip, knee, and ankle function), each rated on a six-point scale (0-5). The total SIAS-motor score was calculated following the methodology established in prior studies [8].
Additionally, the motor component of the Functional Independence Measure (FIM-motor) was recorded for each patient [19]. This score, ranging from 13 to 91, reflects the patient’s degree of dependence or independence. SIAS-motor and FIM-motor assessments were conducted biweekly, with final scores documented at discharge from the rehabilitation facility. The total length of stay (LOS), encompassing both acute care and rehabilitation periods, was also recorded.
Statistical analysis
Pearson’s correlation analyses were performed to explore relationships among CST-LL, BRS total at admission, and SIAS-motor total at discharge. Additionally, a multivariate regression analysis was conducted to assess the predictive value of CST-LL and BRS total at admission for motor recovery outcomes. The regression model included CST-LL and BRS total as independent variables and SIAS-motor total as the dependent variable. Statistical analyses were performed using the JMP software package (SAS Institute Inc., Cary, North Carolina). A p-value of <0.05 was considered statistically significant.
Results
The procedure used to screen patients for the final analytical database is shown in Figure 2. During the study period, 70 patients met the inclusion criteria. After verifying spatial normalization accuracy through visual inspection, six patients were excluded due to the presence of a midline shift. Additionally, three patients were excluded due to incomplete SIAS-motor data. Consequently, 61 patients were included in the final analysis.
Flow chart of the screening process.CT, computed tomography.
Table 1 presents the demographic and clinical characteristics of the study participants. The median age was 66 years (IQR 57-74.5). Of the participants, 35 were male and 26 were female. Lesions were located in the right hemisphere in 35 cases and in the left hemisphere in 26 cases. The median CST-LL was 1.974 mL (IQR 1.113-3.311 mL). Motor impairment was assessed at admission using the BRS. The median BRS scores were 2 (IQR 1-4) for the shoulder/elbow/forearm, 2 (IQR 1-4) for the hand/fingers, and 3 (IQR 2-4.5) for the lower extremities. The total BRS score had a median of 8 (IQR 4-13). Motor function outcomes were evaluated using the SIAS-motor. The median SIAS-motor scores were as follows: arm, 4 (IQR 2-5); finger, 4 (IQR 1-5); hip, 4 (IQR 3-5); knee, 4 (IQR 3-5); and ankle, 4 (IQR 1.5-5). The total SIAS-motor score had a median of 20 (IQR 9.5-24.5). The median score for the Functional Independence Measure motor subscale (FIM-motor) was 81 (IQR 67.5-89). The median LOS was 108 days (IQR 73-152.5).
Table 2 presents the results of the correlation analyses. Significant and strong correlations were observed among CST-LL, BRS total at admission to the acute care hospital, and SIAS-motor total at discharge from the long-term rehabilitation center, with absolute correlation coefficients close to 0.7.
Table 3 summarizes the findings of the multivariate regression analysis. Both CST-LL and BRS total scores at admission were identified as significant predictors of SIAS-motor total scores. The estimated t-values were 4.79 for BRS total and −3.29 for CST-LL, suggesting that these factors had a comparable influence on motor function outcomes. The regression model explained 60.4% of the variance in SIAS-motor total scores.
Table 3: Results of multivariate regression analysis.P < 0.05 was considered statistically significant.BRS, Brunnstrom Recovery Stage; CST-LL, corticospinal tract lesion load; SE, standard error; SIAS-motor, motor component of the Stroke Impairment Assessment Set.
Discussion
This study identified a novel approach for predicting motor outcomes in patients with intracerebral hemorrhage by integrating clinical severity assessments conducted shortly after stroke onset with CST-LL evaluation using routine CT scans. The findings suggest that combining these two factors could enhance prognostic accuracy and support personalized rehabilitation strategies for stroke recovery.
The correlation analysis results (Table 2) provide valuable insights into the relationship between CST-LL and hemiparesis severity both during the acute phase and in the long term. A strong correlation was observed between CST-LL and hemiparesis severity in the early phase, suggesting a meaningful association between these variables [5,7,8,12]. Moreover, when CST-LL and acute-phase clinical severity were analyzed together, they explained a significant proportion of the variance in long-term hemiparesis severity. Multivariate regression analysis further confirmed that both CST-LL and acute-phase severity independently contributed to stroke prognosis (Table 3).
Previous research has established the clinical relevance of CST-LL, beginning with Zhu et al., who examined T1-weighted images in patients with chronic stroke [20]. Feng et al. later extended this concept by analyzing diffusion-weighted imaging in the acute stroke phase [5]. While diffusion-weighted imaging is primarily utilized for diagnosing acute ischemic stroke, both studies focused on ischemic stroke populations [5,20]. To expand CST-LL’s applicability, multiple research groups have explored its utility in hemorrhagic stroke cases using CT imaging [7,8,12]. Their findings align with those from ischemic stroke cohorts, reinforcing the validity of CST-LL as a prognostic marker across stroke subtypes [5,20]. In our prior work, we confirmed the reproducibility of CST-LL measurements across different datasets, demonstrating methodological consistency [8,12]. While external validation remains necessary, the methodology underlying CST-LL assessment holds promise for clinical implementation.
Recent literature has also emphasized the prognostic significance of initial clinical severity in stroke recovery. For example, the Shoulder Abduction, Finger Extension (SAFE) score is a well-recognized tool for predicting upper limb function recovery [21]. This score has been strongly linked to upper extremity outcomes and is widely used in clinical practice [22]. Assessing acute-phase hemiparesis severity allows clinicians to tailor rehabilitation interventions and set realistic recovery goals based on individual patient needs. The severity of initial impairment serves as a key prognostic indicator, helping guide rehabilitation strategies and improve patient outcomes.
In this study, we selected specific scoring systems for evaluating acute-phase hemiparesis severity and long-term motor outcomes based on their clinical utility. The BRS was used during acute care due to its straightforward application [16]. However, because the BRS provides a generalized assessment of lower limb function, the Stroke Impairment Assessment Set (SIAS-motor) was employed for long-term evaluation, as it allows for a more detailed assessment of hip, knee, and ankle function [18]. Given the critical role of regaining ambulation for functional independence in chronic stroke patients, a more granular evaluation of lower extremity function is advantageous [23]. To assess the comparability of these two scoring systems, we preliminarily examined their correlation in a subset of patients who were evaluated using both scales during long-term rehabilitation. The Spearman’s correlation coefficient for the BRS and SIAS-motor total scores at discharge was 0.98 (N=15), demonstrating a strong association between these measures.
Previous literature has indicated that injury to the CST is more closely associated with the severity of upper extremity impairment than with that of lower extremity impairment [1-4]. One possible explanation lies in neuroanatomical differences within the CST related to the control of upper and lower extremities. The CST traverses relatively small and compact regions, including the posterior limb of the internal capsule and the cerebral peduncle. The posterior limb of the internal capsule lies adjacent to the thalamus and putamen, which are common sites of origin for intracerebral hemorrhage. Traditionally, the motor somatotopy in this region has been thought to follow an anteromedial pattern for the upper extremities and a posterolateral pattern for the lower extremities. However, recent studies using diffusion tensor imaging and functional magnetic-resonance imaging have demonstrated a different organization, with the upper extremity represented anterolaterally and the lower extremity posteromedially, along with considerable inter-individual variability in this pattern [24,25]. Accordingly, motor somatotopy is now regarded as more complex than previously believed. In this line, in the present study, we did not differentiate the CST injury according to upper or lower extremity pathways.
This study has several limitations. First, this study included only patients with hemorrhages localized to the thalamus and/or putamen, which may restrict the generalizability of our findings. Future research should consider hemorrhages in other brain regions to assess broader applicability. Second, only functionally independent patients experiencing their first-ever stroke were included, limiting the extension of our results to individuals who required assistance before their stroke. Further studies are needed to validate these findings in a more diverse patient population. Third, our sample size was relatively small (N=61), which may impact the statistical power and generalizability of the results. While small sample sizes are common in neuroimaging research, larger studies would strengthen the reliability of these findings. Despite these constraints, our study provides valuable insights and highlights the need for further investigations to address these limitations and improve understanding across different patient populations and lesion locations.
Conclusions
This study underscores the importance of combining acute-phase clinical severity, assessed by the BRS, with CST-LL measured using routine CT imaging to predict motor recovery in patients with intracerebral hemorrhage. Our findings indicate that these two factors serve as independent yet complementary predictors, together explaining a substantial portion of motor outcome variability. By incorporating both clinical severity and CST-LL into early assessments, clinicians can refine prognosis predictions, tailor rehabilitation strategies, and ultimately enhance patient recovery in stroke rehabilitation.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Prediction tools for stroke rehabilitation Stroke Stinear CM Smith MC Byblow WD 331433225020193161076310.1161/STROKEAHA.119.025696 · doi ↗ · pubmed ↗
- 2Prediction of motor recovery after stroke: advances in biomarkers Lancet Neurol Stinear CM 8268361620172892088810.1016/S 1474-4422(17)30283-1 · doi ↗ · pubmed ↗
- 3Biomarkers of stroke recovery: consensus-based core recommendations from the Stroke Recovery and Rehabilitation Roundtable Neurorehabil Neural Repair Boyd LA Hayward KS Ward NS 8648763120172923307110.1177/1545968317732680 · doi ↗ · pubmed ↗
- 4Prediction of motor recovery after stroke: being pragmatic or innovative?Curr Opin Neurol Rosso C Lamy JC 4824873320203265788910.1097/WCO.0000000000000843 · doi ↗ · pubmed ↗
- 5Corticospinal tract lesion load: an imaging biomarker for stroke motor outcomes Ann Neurol Feng W Wang J Chhatbar PY 8608707820152628912310.1002/ana.24510 PMC 4715758 · doi ↗ · pubmed ↗
- 6Corticospinal tract lesion load originating from both ventral premotor and primary motor cortices are associated with post-stroke motor severity Neurorehabil Neural Repair Ito KL Kim B Liu J 1791823620223495194710.1177/15459683211068441 PMC 8901562 · doi ↗ · pubmed ↗
- 7Determining corticospinal tract injury from stroke using computed tomography Can J Neurol Sci Lam TK Cheung DK Climans SA 7757844720203249353310.1017/cjn.2020.112 · doi ↗ · pubmed ↗
- 8Outcome prediction of patients with intracerebral hemorrhage by measurement of lesion volume in the corticospinal tract on computed tomography Prog Rehabil Med Uchiyama Y Domen K Koyama T 20210050620213496390510.2490/prm.20210050 PMC 8652345 · doi ↗ · pubmed ↗