Global and regional estimates of vaccine-associated herpes zoster and their related vaccines from 1969 to 2023
Jinyoung Jeong, Hyesu Jo, Yejun Son, Jaeyu Park, Jiyeon Oh, Sooji Lee, Yi Deun Jeong, Kyeongmin Lee, Hyeon Jin Kim, Hayeon Lee, Soeun Kim, Yesol Yim, Masoud Rahmati, Jiseung Kang, Raphael Udeh, Damiano Pizzol, Lee Smith, Jiyoung Hwang, Dong Keon Yon

TL;DR
This study estimates global vaccine-associated herpes zoster cases from 1969 to 2023, finding strong links with recent vaccines like mRNA and influenza vaccines.
Contribution
The study provides the first global and regional analysis of vaccine-associated herpes zoster using a large pharmacovigilance database.
Findings
Herpes zoster was most strongly associated with COVID-19 mRNA vaccines, followed by influenza and ad5-vectored vaccines.
The risk of vaccine-associated herpes zoster increased with age and was higher in males than females.
The study highlights the importance of monitoring immune status and managing vaccine-related herpes zoster.
Abstract
Vaccine-induced immunosuppression can reactivate the varicella-zoster virus, potentially leading to the development of herpes zoster. However, the literature on this topic is inconsistent, resulting in limited clarity. Therefore, we aimed to enhance our understanding of vaccine-associated herpes zoster and establish guidelines for future research, utilizing a global database to improve global public health. We investigated vaccine-associated adverse events in herpes zoster using reports (~ 13 million reports) from the WHO international pharmacovigilance database. Data were analyzed for the global number of reports, reported odds ratios (ROR), and information components (IC) to determine the potential association between 18 vaccines and vaccine-associated herpes zoster reports in nearly 170 countries and territories from 1969 to 2023. Of 7,805,380 vaccine-associated adverse events, there…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
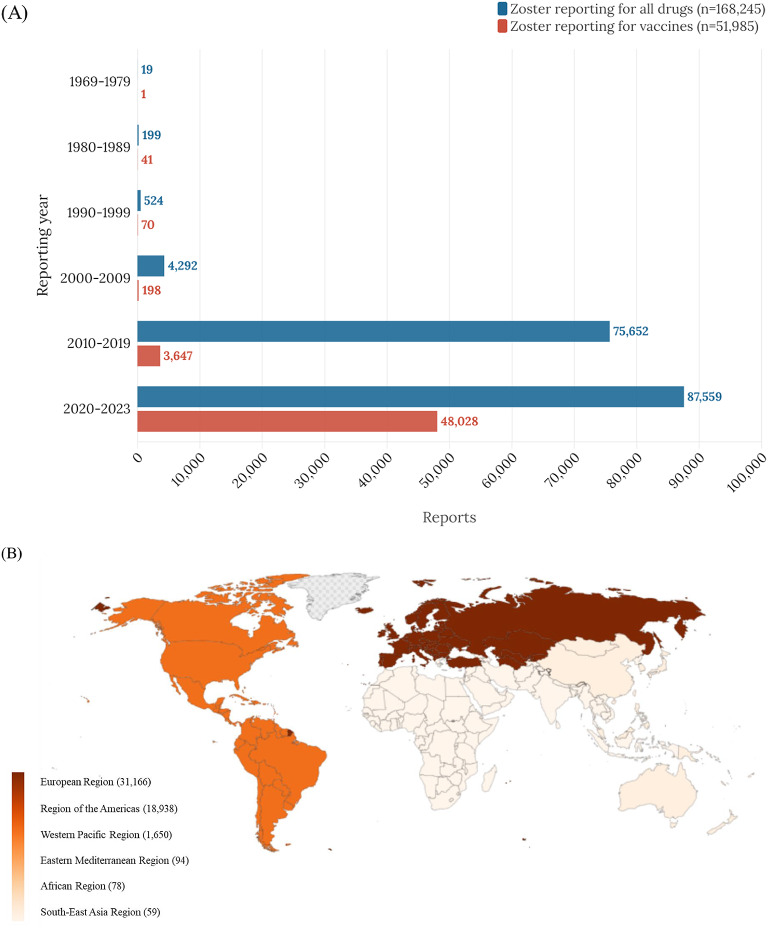 Figure 1
Figure 1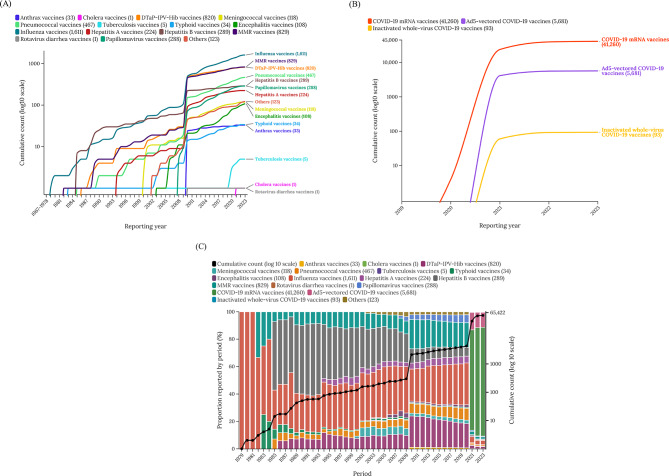 Figure 2
Figure 2- —https://doi.org/10.13039/501100003725National Research Foundation of Korea
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHerpesvirus Infections and Treatments · Virology and Viral Diseases · Drug-Induced Adverse Reactions
Introduction
The global health environment has seen notable advancements in vaccine development, especially in response to the COVID-19 pandemic^1,2^. These vaccines have been pivotal in global public health strategies, effectively reducing disease burden and mortality rates^3^. Nevertheless, similar to several medical interventions, vaccines may evoke adverse events^4^. One of the side effects following vaccination is a temporary decrease in immune response due to the immune system’s reaction to the vaccine^5^. This immunosuppression can also lead to the reactivation of the varicella zoster virus (VZV), potentially resulting in the onset of the zoster^6^.
While these vaccine-associated herpes zoster does not have a high mortality^7^, it can pose a serious threat to the quality of life with painful rashes and nerve pain, as well as serious complications such as encephalitis^8^. Accordingly, many previous studies suggested that various vaccines can cause the onset of zoster, with numerous studies presenting that COVID-19 vaccines may trigger zoster^9^. However, there has been a lack of long-term research on the effects of vaccines on zoster, and studies exploring how vaccine side effects vary by sex and age have also not been conducted.
Therefore, we aimed to investigate the potential association of various vaccines with herpes zosters using the global pharmacovigilance database. Based on the findings of this study, we tried to enhance understanding of vaccine-associated herpes zoster, provide guidelines for future research, and propose appropriate policies to address vaccine-associated herpes zoster.
Methods
Data sources
Our study aimed to investigate the potential adverse effects associated with vaccines, focusing specifically on herpes zoster, by utilizing the World Health Organization (WHO) international pharmacovigilance database. WHO international pharmacovigilance database is the comprehensive global repository that aggregates reports of potential adverse drug reactions^10^. Since its inception in 1969, it has participated in the WHO International Drug Monitoring Program, containing over ~ 13 million reports associated with suspected adverse drug reactions reported by countries actively participating in the program^4,10,11^.
Systematic data collection is ongoing, and our dataset encompasses data collected until June 2023^11,12^. This extensive database comprises information on over 25,000 different pharmaceuticals, providing a comprehensive foundation for the safety evaluation of medications and vaccines^13^. The confidential use of this data was authorized by the Institutional Review Board of Kyung Hee University. Ethical approval and consent were not required as this study was based on publicly available data.
Selection of cases
Data associated with vaccines were collected between 1969 and June 2023. The vaccines were categorized into eighteen different groups: (1) anthrax, (2) cholera, (3) diphtheria, tetanus toxoids, pertussis, polio, and Hemophilus influenzatype b [DTaP-IPV-Hib], (4) meningococcal, (5) pneumococcal, (6) tuberculosis, (7) typhoid, (8) encephalitis (excluding live attenuated vaccines), (9) influenza, (10) hepatitis A, (11) hepatitis B, (12) measles, mumps, and rubella (MMR), (13) rotavirus diarrhea, (14) papillomavirus, (15) COVID-19 mRNA, (16) Ad5-vectored COVID-19, (17) inactivated whole-virus COVID-19, and (18) others (brucellosis, dengue vaccines, Ebola, leptospirosis, plague, rabies, smallpox, tuberculosis, typhus, and yellow fever vaccines)^4^. In this study, we systematically collected and analyzed adverse event reports from non-duplicated sources worldwide, utilizing the Medical Dictionary for Regulatory Activities version 26.0^11,14^. Our focus was primarily on the terms listed in **Table **S1, with a particular emphasis on herpes zoster as reported adverse reactions from global vaccination events. In compliance with the WHO guidelines for causality assessment, our analysis included only those vaccines identified as ‘suspected’ of having a disproportionate association with herpes zoster.
Data collection
To meticulously investigate cases of suspected zoster linked to vaccination, our study thoroughly compiled individual case safety reports acquired from various sources in the post-marketing setting, including patients, healthcare professionals, and pharmaceutical companies, which served as the principal data source for our analysis. The dataset included the following: patient demographics (i.e., age [0 to 11, 12 to 17, 18 to 44, 45 to 64, ≥ 65 years, and unknown] and sex), administrative information (i.e., reporting regions, reporting years, and reporter qualifications [health and non-health professionals, and unknown]). Information on vaccinations (i.e., type and single suspected vaccine), adverse effects, fatal outcomes (recovered/recovering, fatal, and unknown), and time to onset were also included^15^. Every voluntarily submitted report mentioned at least one vaccine suspected of being linked to herpes zoster adverse event.
Statistical analysis
An analysis of disproportionality was carried out for each vaccine listed in the WHO international database to investigate any possible associations with zoster incident reports^4^. The analysis employed two well-established pharmacovigilance metrics: the information component (IC) and the reporting odds ratio (ROR)^4^. The IC is a Bayesian measure employed by the WHO for disproportionality analyses in pharmacovigilance. It is designed to detect potential safety signals by comparing the observed number of adverse drug reaction (ADR) reports with the number expected, based on overall reporting rates in the database. The Bayesian model incorporates prior information and accounts for uncertainty, enhancing the robustness of signal detection^16^. In this study, the IC was calculated by comparing the rate of vaccine associated herpes zoster to the cumulative rate of this event for all other medications reported in our database. The method incorporates the expected number of reports and the observed instances for each vaccine-adverse event pair. IC_0.25_ represents the lower boundary of the 95% confidence interval, and IC_0.25_> 0.00 is generally considered statistically significant signals^17^.
The ROR is a frequentist-based measure commonly employed in pharmacovigilance for disproportionality analyses. Similar to the IC, it aims to identify potential safety signals by comparing the observed frequency of a specific ADR with the frequency expected based on overall reports. In this method, the odds of reporting a particular ADR for a given drug are compared to the odds of reporting the same ADR for all other drugs. We calculated the ROR by examining the rate of vaccine associated herpes zoster relative to all other reported events for that vaccine and then comparing these data with comparable data for other medications in our database. ROR values greater than 1.00—along with 95% confidence intervals that exclude 1.00—are generally interpreted as potential signals warranting further investigation^18^. The advantage of ROR is its straightforward calculation and interpretation, which facilitates large-scale comparative analyses of drug-event associations^19^. Statistical significance was taken into consideration when the two-sided p-value was less than 0.05^20^. All analyses were conducted using SAS software (version 9.4; SAS Institute, Cary, NC, USA).
Results
Overall analysis
Based on the WHO international pharmacovigilance database, a study from 1969 to 2023 included 7,805,380 total vaccine-associated adverse events, containing 51,985 vaccine-associated herpes zoster reports. The reports of vaccine-associated herpes zoster has been steadily increasing since 1969, experienced a sharp rise after 2011, and exploded in number after 2020 (Table 1). The world can be divided into six geographical regions (Fig. 1), with the European region accounting for 59.95% and the region of the Americas for 36.43% of all cases of vaccine-associated herpes zoster, followed by the Western Pacific region (3.17%), African region (0.15%), Eastern Mediterranean region (0.18%), and Southeast Asia region (0.11%). The COVID-19 mRNA vaccines exhibited the most significant association with vaccine-associated herpes zoster (79.37%), followed by ad5-vectored COVID-19 vaccines (10.93%) and influenza vaccines (3.1%). The prognosis for vaccine-associated herpes zoster disease was good for almost all individuals, with only 0.06% fatalities (Table 1).
Table 1. Baseline characteristics of reports on vaccine-associated herpes zoster adverse events. (n = 51,985).VariablesNumber (%)Region reportingAfrican region78 (0.15)Region of the Americas18,938 (36.43)Southeast Asia region59 (0.11)European region31,166 (59.95)Eastern Mediterranean region94 (0.18)Western Pacific region1,650 (3.17)Reporting year1969–19791 (0.00)1980–198941 (0.08)1990–199970 (0.13)2000–2009198 (0.38)2010–20193,647 (7.02)2020–202348,028 (92.39)Reporter qualificationHealth professional9,944 (19.13)Non-health professional22,989 (44.22)Unknown19,052 (36.65)SexMale18,275 (35.15)Female33,142 (63.75)Unknown568 (1.09)Age, years0 to 111,777 (3.42)12 to 17779 (1.50)18 to 4411,021 (21.20)45 to 6416,912 (32.53)≥ 6514,640 (28.16)Unknown6,856 (13.19)TTO, daysMedian days (IQR)1 (1–1)Drug classAnthrax vaccines33 (0.06)Cholera vaccines1 (0.00)DTaP-IPV-Hib vaccines820 (1.58)Meningococcal vaccines118 (0.23)Pneumococcal vaccines467 (0.90)Tuberculosis vaccines5 (0.01)Typhoid vaccines34 (0.07)Encephalitis vaccines108 (0.21)Influenza vaccines1,611 (3.1)Hepatitis A vaccines224 (0.43)Hepatitis B vaccines289 (0.56)MMR vaccines829 (1.59)Rotavirus diarrhea vaccines1 (0.00)Papillomavirus vaccines288 (0.55)COVID-19 mRNA vaccines41,260 (79.37)Ad5-vectored COVID-19 vaccines5,681 (10.93)Inactivated whole-virus COVID-19 vaccines93 (0.18)Others^^123 (0.24)Fatal outcomesRecovered/recovering33,766 (64.95)Fatal33 (0.06)Unknown18,186 (34.98)Single drug suspected51,985 (100.00)DTaP-IPV-Hib, diphtheria, tetanus toxoids, pertussis, polio, and Hemophilus influenza type b; IQR, interquartile range; MMR, measles, mumps, and rubella; TTO, time to onset; WHO, World Health Organization.^^Others: brucellosis, dengue vaccines, Ebola, leptospirosis, plague, rabies, smallpox, tuberculosis, typhus, and yellow fever vaccines.
Fig. 1. Temporal trends (A) and global distribution (B) of vaccine-associated herpes zoster adverse events by continent.
Analysis of the disproportional vaccine-associated herpes zoster
In terms of vaccines showing an association with vaccine-associated herpes zoster, COVID-19 mRNA vaccines displayed the most highest value of ROR and IC (ROR: 11.85 [95% CI, 11.70–12.01]; IC: 2.74 [IC_0.25_, 2.72]), followed by encephalitis vaccines with a considerable association as well (ROR: 4.07 [95% CI, 3.37–4.92]; IC: 2.00 [IC_0.25_, 1.68]), influenza vaccines (ROR: 3.44 [95% CI, 3.28–3.62]; IC: 1.77 [IC_0.25_, 1.69]), and ad5-vectored COVID-19 vaccines (ROR: 3.05 [95% CI, 2.97–3.14]; IC: 1.54 [IC_0.25_, 1.50]) also impacted.
The ROR and IC for vaccine-associated herpes zoster were 7.94 (95% CI, 7.80–8.08) and 2.47 (IC₀.₂₅, 2.45) in males, and 6.71 (95% CI, 6.62–6.80) and 2.30 (IC₀.₂₅, 2.28) in females. The rate of ROR and IC increased with advancing age, with individuals aged over 65 exhibiting the highest ROR and IC values (Table 2).
Table 2. Analysis of subgroups in vaccine-associated herpes zoster adverse events disproportionality.TotalVaccine-associated herpes zosterIC (IC_0.25_) based on age, yearsObservedROR (95% CI)IC (IC_0.25_)0–1112–1718–4445–64≥ 65 Total 7,805,38051,985 7.11 (7.03–7.18)
2.36 (2.34)
0.86 (0.78)
1.75 (1.63)
2.27 (2.24)
2.73 (2.71)
3.13 (3.10) Sex differenceMale2,875,11918,275 7.94 (7.80–8.08)
2.47 (2.45)
0.96 (0.85)
1.99 (1.82)
2.37 (2.31)
2.97 (2.92)
3.29 (3.25) Female4,844,87233,142 6.71 (6.62–6.80)
2.30 (2.28)
0.77 (0.65)
1.58 (1.42)
2.21 (2.17)
2.61 (2.58)
3.00 (2.97) Vaccine typesAnthrax vaccines10,00733 2.58 (1.83–3.63)
1.33 (0.75) N/AN/A1.83 (1.20)1.13 (−0.64)1.52 (−2.26)Cholera vaccines2,46410.32 (0.04–2.25)−1.29 (−5.07)N/AN/A0.01 (−3.77)N/AN/ADTaP-IPV-Hib vaccines811,8998200.79 (0.73–0.84)−0.34 (−0.46) 0.17 (0.03)
0.63 (0.05)
0.62 (0.22)
1.20 (0.87)
1.39 (0.91) Meningococcal vaccines150,6921180.61 (0.51–0.73)−0.71 (−1.01)−0.88 (−1.45)0.38 (−0.20) 0.91 (0.23) 1.19 (−0.02) 2.10 (0.69) Pneumococcal vaccines274,107467 1.33 (1.22–1.46)
0.41 (0.26)
0.51 (0.25) 0.92 (−1.15)−0.44 (−1.65) 1.09 (0.72)
0.85 (0.60) Tuberculosis vaccines34,42650.11 (0.05–0.27)−3.02 (−4.58)−2.92 (−5.51)−0.58 (−4.36)0.91 (−1.68)N/AN/ATyphoid vaccines17,00934 1.56 (1.11–2.19)
0.63 (0.06) 0.07 (−3.71)N/A0.72 (−0.22) 1.32 (0.29)
2.02 (0.60) Encephalitis vaccines20,797108 4.07 (3.37–4.92)
2.00 (1.68) 0.64 (−0.78) 2.23 (0.81)
2.52 (1.94)
2.51 (1.91)
2.52 (1.68) Influenza vaccines368,7281,611 3.44 (3.28–3.62)
1.77 (1.69)
0.78 (0.41) 0.76 (−0.01) 1.38 (1.15)
2.00 (1.85)
2.24 (2.11) Hepatitis A vaccines63,160224 2.78 (2.43–3.16)
1.46 (1.24)
2.67 (2.37)
1.51 (0.64)
1.12 (0.51)
1.68 (1.09)
2.35 (1.48) Hepatitis B vaccines110,354289 2.05 (1.82–2.30)
1.03 (0.83)
0.72 (0.23)
1.49 (0.76)
1.67 (1.33)
2.13 (1.75)
2.76 (1.97) MMR vaccines226,811829 2.87 (2.68–3.07)
1.51 (1.40)
2.49 (2.36)
1.52 (0.79)
0.75 (0.15)
1.70 (0.97)
2.79 (1.48) Rotavirus diarrhea vaccines82,45810.01 (0.00–0.07)−6.15 (−9.93)−5.03 (−8.82)N/AN/AN/AN/APapillomavirus vaccines134,319288 1.68 (1.49–1.88)
0.74 (0.55)
1.02 (0.32)
1.58 (1.31)
1.64 (1.25)
3.18 (2.28) 1.22 (−2.57)COVID-19 mRNA vaccines4,009,12941,260 11.85 (11.70–12.01)
2.74 (2.72)
1.27 (0.88)
2.31 (2.16)
2.72 (2.68)
3.08 (3.05)
3.47 (3.44) Ad5-vectored COVID-19 vaccines1,266,4465,681 3.05 (2.97–3.14)
1.54 (1.50) 1.01 (−0.76)−0.19 (−2.78) 0.96 (0.86)
2.02 (1.96)
2.56 (2.48) Inactivated whole-virus COVID-19 vaccines162,549930.37 (0.30–0.45)−1.42 (−1.77)0.25 (−3.53)N/A−1.47 (−2.09)−1.56 (−2.27)0.00 (−0.57)Others^*^60,025123 1.60 (1.34–1.91)
0.67 (0.37) N/A−0.14 (−2.74) 0.69 (0.19)
1.41 (0.88)
1.89 (0.99) CI, confidence interval; DTaP-IPV-Hib, diphtheria, tetanus toxoids, pertussis, polio, and Hemophilus influenza type b; IC, information component; MMR, measles, mumps, and rubella; N/A, not available; ROR, reported odds ratio.Bold style indicates that the value of IC_0.25_ > 0.00 or the lower end of the ROR 95% CI > 1.00, are statistically significant.Numbers in bold indicate a statistical significance.^*^Others included brucellosis, dengue vaccines, Ebola, leptospirosis, plague, rabies, smallpox, tuberculosis, typhus, and yellow fever vaccines.
Cumulative report analysis
The reporting of vaccine-associated herpes zoster increased significantly from 2011, and a sharp increase can be observed from 2020. From 2011 to 2020, influenza vaccines exhibited a significant association with vaccine-associated herpes zoster. However, since 2020, noticeable influences have also been observed from COVID-19 mRNA vaccines and ad5-vectored COVID-19 vaccines (Fig. 2; Table 3).
Fig. 2. Cumulative number of reports of zoster adverse events per year in association with different vaccines (A-C). Abbreviation: DTaP-IPV-Hib, diphtheria, tetanus toxoids, pertussis, polio, and Hemophilus influenza type b; MMR, measles, mumps, and rubella.
Table 3. Vaccine class-based description of adverse reactions (heatmap).Anthrax vaccinesCholera vaccinesDTaP-IPV-Hib vaccinesMeningococcal vaccinesPneumococcal vaccinesTuberculosis vaccinesTyphoid vaccinesEncephalitis vaccinesInfluenza vaccinesHepatitis A vaccinesHepatitis B vaccinesMMR vaccinesRotavirus diarrhea vaccinesPapillomavirus vaccinesCOVID-19 mRNA vaccinesAd5-vectored COVID-19 vaccinesInactivated whole-virus COVID-19 vaccinesOthers^^ N observed 3318201184675341081,611224289829128841,2605,68193123Age, years0–110 (0.0)0 (0.0)531 (64.8)34 (28.8)153 (32.8)2 (40.0)1 (2.9)6 (5.6)78 (4.8)119 (53.1)46 (15.9)703 (84.8)1 (100.0)23 (8.0)75 (0.2)4 (0.1)1 (1.1)0 (0.0)12–170 (0.0)0 (0.0)33 (4.0)33 (28.0)3 (0.6)1 (20.0)0 (0.0)6 (5.6)19 (1.2)15 (6.7)21 (7.3)21 (2.5)0 (0.0)151 (52.4)472 (1.1)2 (0.0)0 (0.0)2 (1.6)18–4428 (84.8)1 (100.0)67 (8.2)24 (20.3)8 (1.7)2 (40.0)13 (38.2)33 (30.6)208 (12.9)30 (13.4)95 (32.9)31 (3.7)0 (0.0)72 (25.0)9,356 (22.7)980 (17.3)29 (31.2)44 (35.8)45–644 (12.1)0 (0.0)98 (12.0)8 (6.8)77 (16.5)0 (0.0)11 (32.4)31 (28.7)526 (32.7)33 (14.7)77 (26.6)21 (2.5)0 (0.0)14 (4.9)13,425 (32.5)2,526 (44.5)22 (23.7)39 (31.7)≥ 651 (3.0)0 (0.0)49 (6.0)6 (5.1)182 (39.0)0 (0.0)6 (17.6)16 (14.8)673 (41.8)15 (6.7)18 (6.2)7 (0.8)0 (0.0)1 (0.3)11,904 (28.9)1,713 (30.2)35 (37.6)14 (11.4)SexMale28 (84.8)1 (100.0)393 (47.9)45 (38.1)222 (47.5)2 (40.0)14 (41.2)55 (50.9)601 (37.3)114 (50.9)119 (41.2)409 (49.3)0 (0.0)28 (9.7)14,199 (34.4)1,931 (34.0)48 (51.6)66 (53.7)Female5 (15.2)0 (0.0)422 (51.5)72 (61.0)244 (52.2)3 (60.0)19 (55.9)44 (40.7)992 (61.6)109 (48.7)162 (56.1)410 (49.5)1 (100.0)254 (88.2)26,694 (64.7)3,612 (63.6)44 (47.3)55 (44.7)Time to onset,** days**1 (1–1)1 (1–1)1 (1–1)1 (1–1)1 (1–1)1 (1–1)1 (1–1)1 (1–1)1 (1–1)1 (1–1)1 (1–1)1(1–1)1(1–1)1(1–1)1(1–1)1(1–1)1 (1–1)1(1–1) Fatals 0 (0.0)0 (0.0)2 (0.2)1 (0.8)1 (0.2)0 (0.0)0 (0.0)0 (0.0)2 (0.1)1 (0.4)2 (0.7)0 (0.0)0 (0.0)0 (0.0)23 (0.1)1 (0.0)0 (0.0)0 (0.0)Concomitant adverse events, %Coronary6.10.00.40.81.30.02.90.01.40.02.80.20.01.41.11.01.10.8Arrhythmia9.10.02.21.73.620.02.94.63.43.14.82.10.08.03.62.61.16.5Heart failure6.10.00.70.81.10.00.00.90.60.41.70.60.01.40.90.31.10.8Other cardiac diseases0.00.00.00.00.90.00.00.00.40.40.30.10.00.70.60.51.10.8Hyperthermia3.00.06.81.77.920.02.91.93.26.77.67.70.03.83.22.71.18.1Eosinophilia0.00.00.00.00.00.00.00.00.00.00.00.00.00.00.10.00.00.0Thrombocytopenia and leucopenia0.00.00.60.00.620.00.00.00.20.40.70.50.00.30.10.20.00.8Pulmonary0.00.02.01.71.70.00.00.01.73.12.11.60.01.70.70.60.00.0Infections93.9100.070.681.485.980.088.267.681.594.693.490.5100.062.858.634.269.965.9Abdominala3.00.02.03.40.60.00.00.02.63.15.21.30.05.21.71.02.20.8Hepato-biliary0.00.00.60.81.10.00.00.00.22.71.70.50.01.00.20.12.21.6Renal3.00.00.40.01.10.00.00.01.00.90.70.40.01.70.30.10.00.0Endocrine6.10.00.20.81.30.00.00.00.71.31.70.20.01.40.50.40.01.6Muscular18.20.02.73.44.50.02.92.84.14.95.21.10.06.63.22.83.24.9Neurologic36.40.010.512.713.920.05.95.614.814.718.07.70.019.814.114.37.517.1Psychiatric15.20.01.70.83.20.00.00.03.03.61.71.80.08.31.61.00.02.4Osteoarticular and rheumatologic15.20.01.20.03.90.00.00.92.50.95.21.00.04.92.21.52.22.4Dermatologic27.3100.029.022.033.460.035.39.327.631.732.230.50.019.416.711.93.222.8Anaphylaxis0.00.00.41.70.20.00.00.90.70.41.00.10.00.00.30.10.00.0Ophthalmology9.10.01.60.03.40.00.00.91.92.21.70.80.02.11.10.50.04.1The heatmap was expressed according to the percentage value.DTaP-IPV-Hib, diphtheria, tetanus toxoids, pertussis, polio, and Hemophilus influenza type b; IQR, interquartile range; MMR, measles, mumps, and rubella; TTO, time to onset.^^Others included brucellosis, dengue vaccines, Ebola, leptospirosis, plague, rabies, smallpox, tuberculosis, typhus, and yellow fever vaccines.
Discussion
Main findings
This is the first study to investigate the potential association between various vaccines and herpes zoster across a large population (total = 7,805,380) over a long period, from 1969 to 2023. The reporting of vaccine-associated herpes zoster has sharply increased since the introduction of influenza vaccines in 2011, with a further rapid rise observed in 2020 following the introduction of COVID-19 mRNA vaccines and ad5-vectored COVID-19 vaccines. The COVID-19 mRNA vaccine showed the greatest ROR and IC value with vaccine-associated herpes zoster, followed by the encephalitis vaccine, influenza vaccine, and ad5-vectored COVID-19 vaccine. Regarding sex and age, an increased rate of ROR and IC for vaccine-associated herpes zoster was observed among males and older populations. While zoster can lead to various complications and further research is needed for the appropriate management of vaccine-associated herpes zoster, its mortality rate is low. Therefore, there is no need to hesitate about vaccination.
Interpretations of the study findings
Our study found that COVID-19 mRNA vaccines and ad5-vectored COVID-19 vaccines are significantly associated with vaccine-associated herpes zoster. However, according to previous research, the degree of association varied between these two, which can be attributed to differences in cytokine activation and T-cell immune responses among vaccines. The mechanism by which these vaccines might trigger herpes zoster involves the role of T lymphocytes in controlling VZV during its latent phase. Vaccination-induced T-cell dysfunction could play a part in this occurrence. Presenting more detailed mechanisms, it has been observed that COVID-19 vaccination induces a robust T-cell response and enhances the proinflammatory action profile in potent antigen-presenting cells via the spike protein, potentially causing VZV reactivation. Additionally, a significant shift of naive CD8 + cells to create specific CD8 + cells might temporarily impair the control of VZV by VZV-specific CD8 + cells. Furthermore, changes in Toll-like receptor signaling due to vaccination or the effects of cytokines such as type I interferon might be involved^9^.
Another vaccine that showed an association with vaccine-associated herpes zoster in the present study is the encephalitis vaccine. There have been reports of systemic urticaria or rash following encephalitis vaccination^21^. Additionally, side effects such as fatigue suggest the possibility of zoster occurrence due to immunosuppression. Influenza vaccines are hypothesized to cause vaccine-associated herpes zoster due to the dysregulation of T cells and cellular immunity. This dysregulation is likely due to immune modulation induced by the vaccines’ target vectors or adjuvants, which could play a role in reactivating the virus. It is also speculated that the reactivation of VZV is caused by the interaction of various factors with a summation effect^22^.
Our research indicates that the value of ROR and IC for vaccine-associated zoster due to vaccines is higher in males. Although, previous studies have reported either a higher incidence of zoster in females or no significant difference based on sex, there has been no precise analysis explaining these results. Additionally, it has been suggested that this discrepancy could be due to females being more likely to visit their clinics when experiencing symptoms of zoster^23–25^. Therefore, further research is needed to understand why the risk varies between sexes.
Comparison of previous studies
Previous studies investigated the impact of COVID-19 mRNA, ad5-vectored COVID-19, and influenza vaccines on vaccine-associated herpes zoster, showing results similar to ours^6,9,22,26^. However, these studies were limited by their short duration and smaller sample sizes, which lowered their reliability. In contrast, our study was conducted over a more extended period with a larger population, encompassing all types of vaccines. Additionally, by targeting a global population, we further increased the credibility of our results.
Other prior research has indicated that females and older individuals are more susceptible to zoster. While prior studies have investigated the association between age, sex, and the onset of herpes zoster^27^, there has been no investigation into how vaccine influences change depending on age and sex. Therefore, this study is the first to explore how vaccines influence zoster across different age groups and sexes.
Clinical policy implications
While herpes zoster is not a disease with a high mortality rate^28^, it is a quality-of-life-threatening condition characterized by very painful rashes and neuralgia^29^. It can also carry the risk of leading to severe complications^30^. Moreover, there are ongoing reports regarding vaccine-associated herpes zoster. Despite this, there is a lack of research on vaccine-associated herpes zoster. Therefore, it is imperative to facilitate more related studies and use the accumulated results from various research to propose compensation and management manuals.
Vaccine-associated herpes zoster occurs when the latent VZV virus reactivates, primarily controlled by T lymphocytes. As the dysregulation of T cells is the leading cause of vaccine-associated herpes zoster, an individual’s immune status plays a crucial role^31^. Consequently, it is essential to properly assess an individual’s health status before administering a vaccine and provide guidance accordingly. This study also found that older individuals are especially susceptible to vaccine-associated herpes zoster. Therefore, checking a patient’s immune status before vaccination is necessary, and attention should be paid to older individuals and males.
Strengths and limitations
Using a global pharmacovigilance database, this study is the first to conduct a long-term investigation on the side effects of zoster associated with various vaccines across a broad population. Furthermore, this research also observed how these side effects vary according to age and sex, thereby enhancing the reliability of the findings compared to previous studies. However, despite these strengths, the present study still has several limitations.
First, due to the inherent characteristics of the study being a cross-sectional analysis, a limitation arises because it is not possible to definitively ascertain the causes of the outcomes derived from the data analysis within the results themselves^32^. However, the study attempted to explain the mechanisms as clearly as possible, building upon previous findings. Furthermore, if future studies are conducted to analyze the causes based on the results, the understanding of vaccine-associated herpes zoster could be significantly advanced.
Second, the structure of the reporting system that analyzes vaccine-associated herpes zoster has limitations. This study relied on passive reporting methods, which may lead to an underrepresentation of vaccine-associated herpes zoster cases and distort report rates. Therefore, it is probable that fewer incidents were reported than occurred, suggesting the possibility that associations were observed less than they exist.
Third, there may be bias in the results due to the possibility that individuals who received vaccines managed their health and well-being better than those who did not receive vaccinations. This is a consequence of not being able to exclude the various characteristics possessed by the vaccinated individuals, potentially leading to errors attributable to the specific environments of certain groups. However, we included a large number of participants, and all values utilized in interpreting the research findings were significant. Therefore, these factors are unlikely to have significantly reduced the reliability of the results.
Fourth, the lack of reports on live attenuated vaccines among encephalitis vaccines in this study limited a comprehensive analysis of their effects. Although the study was initially designed to include an analysis of live attenuated vaccines, there was insufficient data on live attenuated vaccines related to vaccine-associated herpes zoster, preventing their inclusion in the study. Consequently, the findings related to encephalitis vaccines in this study should primarily be interpreted based on inactivated vaccines, and further comprehensive research that includes live attenuated vaccines is warranted. Fifth, various reporting biases may have influenced the study results. In particular, this study observed a sharp increase in reporting rates after 2011, which may have been influenced by the development of reporting systems. Additionally, in countries with well-established reporting systems, vaccine-related adverse events are more likely to be reported compared to those with less developed systems. Therefore, interpreting an increase in reported cases solely as a rise in adverse event rates may not be appropriate, and cautious interpretation and thorough examination are required when considering the generalizability of the findings. Lastly, our analysis was based on self-reported data obtained from the WHO global pharmacovigilance database. Due to the inability to determine the population at risk required for incidence rate calculation, we were unable to analyze the incidence rate of vaccine-associated herpes zoster.
Conclusion
This study is the first to observe the global impact of various vaccines on herpes zoster over a long period, from 1969 to 2023. Vaccine-associated herpes zoster increased due to the influenza vaccines starting in 2011, with a sharp rise after the introduction of COVID-19 vaccines in 2020. Although various vaccines can lead to herpes zoster, the mortality rate is very low, so vaccination might not be hesitated. The highest ROR and IC values for vaccine-associated herpes zoster were observed with the COVID-19 mRNA vaccine, followed by the encephalitis vaccine, influenza vaccine, and ad5-vectored COVID-19 vaccine. Additionally, this study identified elevated ROR and IC rates for vaccine-associated herpes zoster among males and older individuals. Based on the research findings, it is essential to consider the immune status of individuals receiving vaccines and to implement appropriate compensation and management manuals for vaccine-associated herpes zoster.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Supplementary Material 1
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Al Fayez, N. et al. Recent advancement in m RNA vaccine development and applications. Pharmaceutics 1510.3390/pharmaceutics 15071972 (2023).10.3390/pharmaceutics 15071972 PMC 1038496337514158 · doi ↗ · pubmed ↗
- 2Patil, A., Goldust, M. & Wollina, U. Herpes Zoster: A review of clinical manifestations and management. Viruses 1410.3390/v 14020192 (2022).10.3390/v 14020192 PMC 887668335215786 · doi ↗ · pubmed ↗
- 3Park, J., Kim, D. & Song, T. J. A disproportionality analysis for association of systemic capillary leak syndrome with COVID-19 vaccination using the world health organization pharmacovigilance database. Vaccines (Basel). 10. 10.3390/vaccines 10060835 (2022).10.3390/vaccines 10060835 PMC 922746335746443 · doi ↗ · pubmed ↗
- 4Schmader, K. Herpes Zoster. Ann. Intern. Med.169 (Itc 19-itc 31). 10.7326/aitc 201808070 (2018).10.7326/AITC 20180807030083718 · doi ↗ · pubmed ↗