Goserelin 3-month depot shows non-inferiority to the monthly formulation in U.S. patients with premenopausal breast cancer: a real-world evidence study
Kelly E. McCann, Noran Osman, Joan Cannon, Lonnie Brent, Yuexi Wang, Jon Tepsick, Prithviraj Vikramsinh Mandora, Vincent Miller, Nancy Martin, Virginia G. Kaklamani

TL;DR
A real-world study shows that a 3-month goserelin dose is as effective as the monthly dose for premenopausal breast cancer patients.
Contribution
This study provides real-world evidence supporting the non-inferiority of 3-month goserelin over the monthly formulation.
Findings
12-month event-free survival was 79.2% for 3-month goserelin and 76.6% for monthly goserelin.
Non-inferiority was observed in both early-stage and metastatic breast cancer patients.
The treatment difference was within the non-inferiority margin of −15%.
Abstract
Clinical trials demonstrated every 3-month goserelin 10.8 mg to be non-inferior to monthly goserelin 3.6 mg in premenopausal patients with ER-positive breast cancer. However, real-world studies comparing 3-month goserelin 10.8 mg with monthly goserelin 3.6 mg are scarce. Electronic medical records from the ConcertAI Patient360™ database were analyzed in U.S. patients exposed to goserelin 3.6 mg or 10.8 mg post-breast cancer diagnosis. Inverse probability of treatment weighting (IPTW) was used to ensure the comparability between the two cohorts (goserelin 3.6 mg and goserelin 10.8 mg). The non-inferiority of goserelin 10.8 mg compared with goserelin 3.6 mg was assessed by 12-month real-world event-free survival (rwEFS) rates (− 15% margin) for the overall group of patients and separately for patients with early-stage/locally advanced and metastatic breast cancer. A total of 575…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
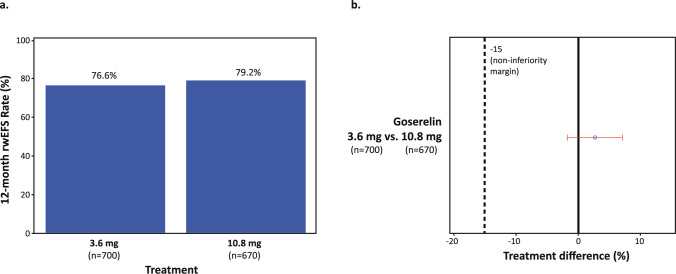 Figure 1
Figure 1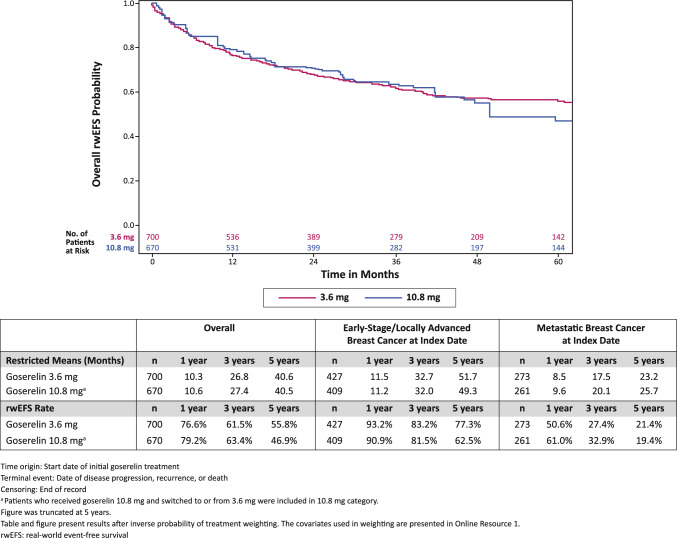 Figure 2
Figure 2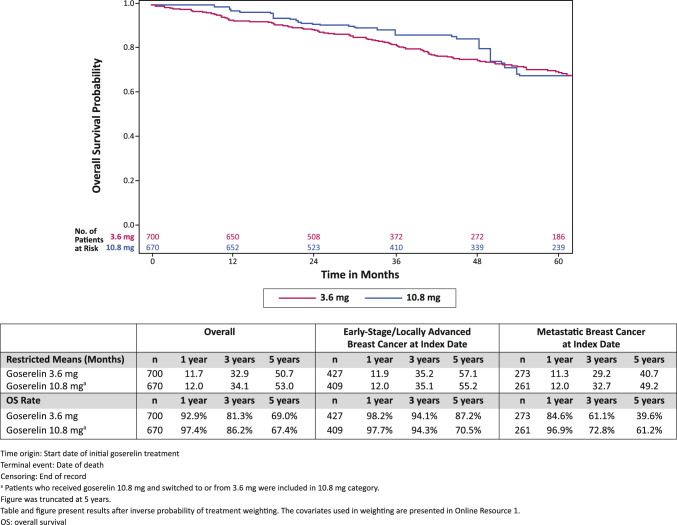 Figure 3
Figure 3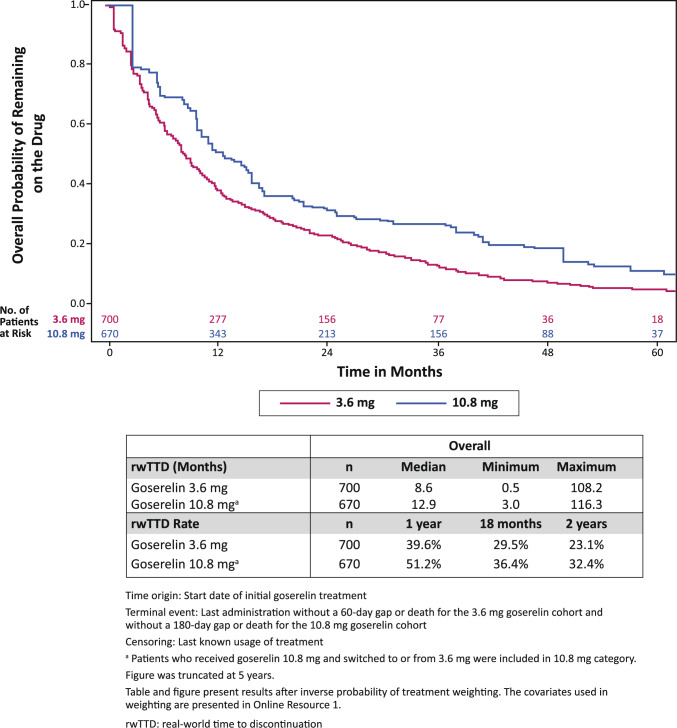 Figure 4
Figure 4- —TerSera Therapeutics LLC
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsBreast Cancer Treatment Studies · HER2/EGFR in Cancer Research · Cancer Risks and Factors
Introduction
Over three-quarters of breast cancer cases are estrogen receptor-positive (ER +) [1]. In premenopausal patients with ER + breast cancer, tumor growth can be decreased by reducing estrogen production via ovary removal, ovarian ablation, or the administration of a gonadotropin-releasing hormone agonist (GnRHa) [2]. Goserelin, a GnRHa, is recommended in the current NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines®) for ovarian function suppression with adjuvant endocrine therapy and start of chemotherapy (neoadjuvant or adjuvant) in premenopausal patients with hormone receptor-positive breast cancer who are at high risk of recurrence [3].
Patients with breast cancer who received goserelin had a decreased risk of all-cause mortality and breast cancer related-mortality as well as a lower risk of disease recurrence and disease progression [4, 5]. The efficacy and safety of goserelin, with or without concomitant endocrine therapy, in premenopausal and perimenopausal women with ER + advanced breast cancer are well documented [6–9].
The goserelin 3.6 mg implant is administered every 4 weeks and has been approved by the United States (U.S.) Food and Drug Administration (FDA) for decades for premenopausal and perimenopausal patients with breast cancer [10]. The goserelin 10.8 mg implant is administered once every 12 weeks and may provide a more convenient treatment option for patients due to its less frequent administration schedule. However, goserelin 10.8 mg is currently not approved by the U.S. FDA for patients with breast cancer [11]. The formulation was approved by Health Canada in May 2024 for patients with ER + breast cancer [12].
In addition to a less frequent administration schedule, clinical trials have shown that goserelin 10.8 mg had similar outcomes as goserelin 3.6 mg in premenopausal women with ER + breast cancer. A Phase 2 clinical trial found that goserelin 10.8 mg was non-inferior for serum estrogen suppression compared with goserelin 3.6 mg [13]. A Phase 3 trial conducted in Asia showed that goserelin 10.8 mg was non-inferior compared with goserelin 3.6 mg for progression-free survival at 24 weeks (61.5% versus 60.2%; treatment difference 1.3%) in patients with advanced breast cancer [14]. Although these studies have compared the outcomes of goserelin 3.6 mg and goserelin 10.8 mg in clinical trials, no U.S. studies, to our knowledge, have examined these outcomes of 3-month goserelin 10.8 mg and the monthly goserelin 3.6 mg in the real-world setting.
The aim of this study was to provide insights into the utility of goserelin 10.8 mg in patients with breast cancer. The primary objective of this study was to evaluate if the real-world event-free survival (rwEFS) in patients receiving goserelin 10.8 mg was non-inferior to goserelin 3.6 mg in the real-world setting. The study also sought to examine patient characteristics and real-world clinical outcomes among patients with breast cancer who received goserelin 3.6 mg and 10.8 mg.
Methods
Study population
This retrospective, non-interventional study used electronic medical record (EMR) data collected from geographically diverse oncology practice locations within the U.S. and included in the ConcertAI Patient360™ Breast Cancer dataset. The ConcertAI Patient360™ dataset comprises de-identified structured and unstructured data (text and image documents, such as physician notes and pathology reports). The unstructured data were manually curated by trained curators for the ConcertAI Patient360™ Breast Cancer dataset and evaluated for consistency, completeness, and outlier values.
Patients who were female assigned at birth, aged 18–55 years without evidence of being postmenopausal at initial breast cancer diagnosis and exposed to goserelin 3.6 mg or 10.8 mg post-breast cancer diagnosis were included in the study. All patients had at least 360 days of follow-up after the initiation of goserelin or died before 360 days of follow-up. Patients were included in the study regardless of ER, human epidermal growth factor receptor 2 (HER2), and progesterone receptor (PR) status observed in the data. Patients with other primary tumors and those enrolled in a clinical trial during goserelin use were excluded.
Two cohorts were created based on goserelin use: (1) 3.6 mg cohort: patients only receiving goserelin 3.6 mg, and (2) 10.8 mg cohort: patients with any use of goserelin 10.8 mg within 6 months of initial goserelin treatment (includes patients who switched from or to goserelin 3.6 mg). The index date was defined as the date of first goserelin exposure. The study period was defined as the interval between initial breast cancer diagnosis and last activity date, data cutoff, or death (whichever occurred first).
This research was reviewed and determined to be exempt from Institutional Review Board (IRB) oversight by Advarra IRB (Columbia, Maryland). Informed consent was not applicable for this study.
Study endpoints
The primary outcome was the 12-month rwEFS rate to assess the non-inferiority of 3-month goserelin 10.8 mg versus monthly goserelin 3.6 mg. Secondary endpoints included real-world overall survival (OS) and real-world time to treatment discontinuation (rwTTD). The study endpoints were reported in the overall populations for each cohort and by stage of breast cancer (early-stage/locally advanced or metastatic) at initiation of goserelin.
rwEFS was defined as the time from initiation of goserelin to the first documented date of disease recurrence/disease progression or death from any cause (whichever occurred first). Patients without documented disease recurrence/progression or death were censored on the date of the last activity date. OS was defined as the time from initiation of goserelin to the date of death from any cause. For patients not known to be deceased at the time of analysis, OS was censored at the last date the patient was known to be alive. rwTTD was defined as the time from initiation of goserelin to the last administration without a 60-day gap or death for the 3.6 mg goserelin cohort and without a 180-day gap or death for the 10.8 mg goserelin cohort. This timeframe allows for 2 cycles of each respective dosage to be missed before being considered as discontinued. Patients were censored at last known usage of treatment.
Statistical analysis
Descriptive statistics were used to summarize patient characteristics and evaluate the differences between the 3.6 mg cohort and the 10.8 mg cohort. Inverse probability of treatment weighting (IPTW) was used to ensure comparability of baseline demographic and clinical characteristics between the two cohorts. IPTW uses the propensity score to balance baseline patient characteristics in the exposed (those who received 10.8 mg goserelin treatment) and unexposed groups (those who received 3.6 mg goserelin treatment) by weighting each individual by the inverse probability of receiving actual treatment. Weights were calculated for each individual as 1/propensity score for the exposed group and 1/(1 − propensity score) for the unexposed group. The standardized difference, which compares the difference in the means between groups, was also reported [15]. Variables included in the IPTW can be found in Online Resource 1. Variables were selected based on the data available in the EMR data.
Non-inferiority testing was conducted for rwEFS rate at 12 months. U.S. FDA guidelines recommend that both statistical and clinical judgment be considered when choosing a non-inferiority margin [16]. Based on the clinical trial results presented by Noguchi et al., the extrapolated 12-month rwEFS was estimated to be 36.2% for the goserelin 3.6 mg cohort and 37.8% for the goserelin 10.8 mg cohort. A power analysis showed a total sample size of 210 patients (105 patients in each cohort) was necessary for the study to demonstrate a non-inferiority margin of 15% with 80% power and an alpha of 0.05. As a result, the non-inferiority margin was set at − 15% between treatment groups based on published oncology clinical trials and the results of the power analysis [17]. The hypothesis for the primary outcome was that goserelin 10.8 mg would be non-inferior to goserelin 3.6 mg at the prespecified margin.
Weighted Kaplan–Meier analyses were conducted for rwEFS, OS, and rwTTD for each cohort. Restricted mean survival time and survival rates at 6 months, 1 year, 3 years, and 5 years were calculated for rwEFS and OS [18]. The proportion of patients who remained on the treatment at 6 months, 12 months, 18 months, and 24 months was also reported.
Results
Patient characteristics
A total of 698 patients were included in the study, with 575 patients in the goserelin 3.6 mg cohort and 123 patients in the goserelin 10.8 mg cohort. In the goserelin 10.8 mg cohort, 35 (28.5%) patients switched to or from goserelin 3.6 mg and received goserelin 10.8 mg within 6 months of initial goserelin treatment.
After weighting, the 3.6 mg cohort had a median age of 41 years, and 70.3% of patients were White (Table 1). A majority of patients (68.3%) had infiltrating ductal carcinoma histology, and 61.0% of patients had early-stage/locally advanced breast cancer at initial goserelin treatment. The 10.8 mg cohort had a median age of 42 years, and 69.9% of patients were White. Most patients (70.2%) in the 10.8 mg cohort had infiltrating ductal carcinoma histology, and 61.0% of patients had early-stage/locally advanced breast cancer at initial goserelin treatment. Online Resource 2 presents the Love plot of the standardized differences for the unweighted and weighted variables. The median follow-up time from the index date to the end of the record for the 3.6 mg cohort was 37.1 months and 36.3 months for the 10.8 mg cohort.Table 1. Patient Characteristics Pre- and Post-Weighting by Goserelin DosagePre-WeightingPost-WeightingVariableGoserelin 3.6 mgn = 575Goserelin 10.8 mg^a^n = 123Goserelin 3.6 mgn = 700Goserelin 10.8 mg^a^n = 670Standardized DifferenceAge at initial breast cancer diagnosis, median (min, max) (years)41 (24–55)41 (22–55)41 (24–55)42 (22–55)0.0521Race, n (%)0.02884 White418 (72.7)74 (60.2)492 (70.3)468 (69.9) Black or African American77 (13.4)26 (21.1)101 (14.5)103 (15.3) Other or unknown race80 (13.9)23 (18.7)106 (15.2)99 (14.8)Stage at initial breast cancer diagnosis, n (%)0.4676 Stage 0 + Stage I127 (22.1)26 (21.1)153 (21.8)158 (23.5) Stage II196 (34.1)48 (39.0)246 (35.2)229 (34.2) Stage III110 (19.1)19 (15.4)129 (18.5)114 (17.0) Stage IV86 (15.0)21 (17.1)106 (15.2)90 (13.4) Unknown56 (9.7)9 (7.3)66 (9.4)79 (11.8)Comorbidities at initial breast cancer diagnosis, n (%) Chronic obstructive pulmonary disease, unspecified29 (5.0)3 (2.4)32 (4.6)37 (5.5) Type 2 diabetes mellitus without complications24 (4.2)1 (< 1)31 (4.4)7 (1.0) Autoimmune disease10 (1.7)2 (1.6)11 (1.6)16 (2.4)Surgical procedures prior to initial goserelin therapy, n (%)0.04397 Mastectomy309 (53.7)69 (56.1)381 (54.4)351 (52.3) Excision81 (14.1)15 (12.2)95 (13.6)98 (14.6) Both mastectomy and excision66 (11.5)18 (14.6)84 (12.0)80 (12.0) No surgery119 (20.7)21 (17.1)140 (19.9)141 (21.1)Timing of initial goserelin therapy, n (%)0.00109 Early-stage/locally advanced breast cancer, prior to metastatic diagnosis (if any)349 (60.7)77 (62.6)427 (61.0)409 (61.0) At or after metastatic diagnosis226 (39.3)46 (37.4)273 (39.0)261 (39.0)Histology at initial breast cancer diagnosis, n (%)0.18494 Infiltrating duct393 (68.3)81 (65.9)478 (68.3)470 (70.2) Infiltrating lobular46 (8.0)4 (3.3)50 (7.1)27 (4.1) Infiltrating duct and lobular28 (4.9)8 (6.5)36 (5.2)45 (6.8) Carcinoma in situ + Other/Unknown108 (18.8)30 (24.4)136 (19.4)127 (18.9)HER2 status, n (%)0.10448 Positive87 (15.1)20 (16.3)106 (15.1)81 (12.0) Low211 (36.7)44 (35.8)257 (36.7)229 (34.3) Negative253 (44.0)51 (41.5)302 (43.2)324 (48.3) Equivocal/Conflict/Unable to confirm/Unknown24 (4.2)8 (6.5)35 (5.0)36 (5.4)PR status, n (%)0.12908 Positive486 (84.5)102 (82.9)586 (83.8)534 (79.7) Negative76 (13.2)16 (13.0)92 (13.2)111 (16.5) Conflict/Unknown13 (2.3)5 (4.1)21 (3.0)25 (3.8)^a^Patients who received goserelin 10.8 mg and switched to or from 3.6 mg were included in the 10.8 mg categoryData source: ConcertAI Patient360™ Breast Cancer datasetStudy population: Patients who were female assigned at birth, aged 18–55 years without evidence of being postmenopausal at initial breast cancer diagnosis and exposed to goserelin 3.6 mg or 10.8 mg post-breast cancer diagnosis were included in the study. All patients had at least 360 days of follow-up after the initiation of goserelin or died before 360 days of follow-up. Two cohorts were created based on goserelin use: 1) 3.6 mg cohort: patients only receiving goserelin 3.6 mg, and 2) 10.8 mg cohort: patients with any use of goserelin 10.8 mg within 6 months of initial goserelin treatment (includes patients who switched from or to goserelin 3.6 mg)Index date: The date of first goserelin exposureThe covariates used in weighting are presented in Online Resource 1HER2: human epidermal growth factor receptor 2; Max: maximum, Min: minimum; PR: progesterone receptor
Non-inferiority test
The 12-month rwEFS rates were 76.6% for the 3.6 mg cohort and 79.2% for the 10.8 mg cohort, with a treatment difference of 2.7% (95% CI − 1.8%, 7.0%) (Table 2, Fig. 1). This result supports the hypothesis that goserelin 10.8 mg is non-inferior to goserelin 3.6 mg at the prespecified − 15% margin.Table 2. Weighted Non-Inferiority^a^ Analysis of 12-Month rwEFS Rate by Dosage of GoserelinNon-Inferiority TestGoserelin3.6 mgGoserelin10.8 mg^b^Treatment DifferenceOverall n700****670 12-month rwEFS rate76.6%79.2%2.7% 95% CI72.8%, 79.9%68.2%, 86.8%−1.8%, 7.0%Early-stage/locally advanced breast cancer at index date n427****409 12-month rwEFS rate93.2%90.9%−2.3% 95% CI89.9%, 95.4%77.7%, 96.4%−6.0%, 1.4%Metastatic breast cancer at index date n273****261 12-month rwEFS rate50.6%61.0%10.4% 95% CI43.8%, 57.0%41.2%, 75.9%2.0%, 18.9%Time origin: Start date of initial goserelin treatment (index date)Terminal event: Date of disease progression, recurrence, or deathCensoring: End of recordResults after inverse probability of treatment weighting. The covariates used in weighting are presented in Online Resource 1^a^Non-inferiority for rwEFS was based on a prespecified margin of 15% between treatment groups using a 2-sided 95% CI^b^Patients who received goserelin 10.8 mg and switched to or from 3.6 mg were included in the 10.8 mg categoryCI: confidence interval, rwEFS: real-world event-free survivalFig. 1Weighted Bar Graph (a) and Forest Plot (b) of 12-Month rwEFS Rate by Dosage of Goserelin. Results after inverse probability of treatment weighting. The covariates used in weighting are presented in Online Resource 1. rwEFS: real-world event-free survival
For patients with early-stage/locally advanced breast cancer at the time of initial goserelin treatment, the 12-month rwEFS rate was 93.2% for the 3.6 mg cohort and 90.9% for the 10.8 mg cohort, with a treatment difference of − 2.3% (95% CI − 6.0%, 1.4%). For patients with metastatic breast cancer at the time of initial goserelin treatment, the 12-month rwEFS rate was 50.6% for the 3.6 mg cohort and 61.0% for the 10.8 mg cohort, with a treatment difference of 10.4% (95% CI 2.0%, 18.9%). These results suggested that goserelin 10.8 mg was non-inferior to goserelin 3.6 mg at the prespecified − 15% margin regardless of stage of disease at time of initiation.
Real-world event-free survival
Kaplan–Meier analysis showed patients in the 3.6 mg cohort had a rwEFS rate at 1 year of 76.6% and 79.2% for the 10.8 mg cohort (Fig. 2). The rwEFS rate at 3 years for the 3.6 mg cohort was 61.5% and 63.4% for the 10.8 mg cohort. The rwEFS rate at 5 years for the 3.6 mg cohort was 55.8% and 46.9% for the 10.8 mg cohort. The restricted means for each cohort are presented in Fig. 2.Fig. 2. Weighted Kaplan–Meier Analysis of rwEFS by Dosage of Goserelin
For patients with early-stage/locally advanced breast cancer at the time of initial goserelin treatment, the rwEFS rate at 1 year for the 3.6 mg cohort was 93.2% and 90.9% for the 10.8 mg cohort. The rwEFS rate at 3 years for the 3.6 mg cohort was 83.2% and 81.5% for the 10.8 mg cohort. The rwEFS rate at 5 years for the 3.6 mg cohort was 77.3% and 62.5% for the 10.8 mg cohort. The restricted means for patients with early-stage/locally advanced breast cancer are presented in Fig. 2.
For patients with metastatic breast cancer at the time of initial goserelin treatment, the rwEFS rate at 1 year for the 3.6 mg cohort was 50.6% and 61.0% for the 10.8 mg cohort. The rwEFS rate at 3 years for the 3.6 mg cohort was 27.4% and 32.9% for the 10.8 mg cohort. The rwEFS rate at 5 years for the 3.6 mg cohort was 21.4% and 19.4% for the 10.8 mg cohort. The restricted means for patients with metastatic breast cancer are presented in Fig. 2.
Real-world overall survival
For OS, the rate at 1 year for the 3.6 mg cohort was 92.9% and 97.4% for the 10.8 mg cohort (Fig. 3). The OS rate at 3 years for the 3.6 mg cohort was 81.3% and 86.2% for the 10.8 mg cohort. The OS rate at 5 years for the 3.6 mg cohort was 69.0% and 67.4% for the 10.8 mg cohort. The restricted means for each cohort are presented in Fig. 3.Fig. 3. Weighted Kaplan–Meier Analysis of OS by Dosage of Goserelin
For patients with early-stage/locally advanced breast cancer at the time of initial goserelin treatment, the OS rate at 1 year for the 3.6 mg cohort was 98.2% and 97.7% for the 10.8 mg cohort. The OS rate at 3 years for the 3.6 mg cohort was 94.1% and 94.3% for the 10.8 mg cohort. The OS rate at 5 years for the 3.6 mg cohort was 87.2% and 70.5% for the 10.8 mg cohort. The restricted means for patients with early-stage/locally advanced breast cancer are presented in Fig. 3.
For patients with metastatic breast cancer at the time of initial goserelin treatment, the OS rate at 1 year for the 3.6 mg cohort was 84.6% and 96.9% for the 10.8 mg cohort. The OS rate at 3 years for the 3.6 mg cohort was 61.1% and 72.8% for the 10.8 mg cohort. The OS rate at 5 years for the 3.6 mg cohort was 39.6% and 61.2% for the 10.8 mg cohort. The restricted means for patients with metastatic breast cancer are presented in Fig. 3.
Real-world time to discontinuation
The proportion of patients who remained on the initial goserelin treatment at 1 year for the 3.6 mg cohort was 39.6% and 51.2% for the 10.8 mg cohort (Fig. 4). The proportion of patients who remained on the initial goserelin at 2 years for the 3.6 mg cohort was 23.1% and 32.4% for the 10.8 mg cohort. The median rwTTD for the 3.6 mg cohort was 8.6 months and 12.9 months for the 10.8 mg cohort. For patients with early-stage/locally advanced breast cancer at the time of initial goserelin treatment, the median rwTTD for the 3.6 mg cohort was 8.8 months and 15.7 months for the 10.8 mg cohort. For patients with metastatic breast cancer at the time of initial goserelin treatment, the median rwTTD for the 3.6 mg cohort was 8.4 months and 10.0 months for the 10.8 mg cohort.Fig. 4. Weighted Kaplan–Meier Analysis of rwTTD by Dosage of Goserelin
Discussion
This real-world analysis indicated that goserelin 10.8 mg was non-inferior to goserelin 3.6 mg among premenopausal patients with breast cancer in terms of 12-month rwEFS rate, regardless of the stage of breast cancer at initiation of goserelin treatment. The OS rates were similar among both groups at 1, 3, and 5 years. At 1 year, almost 40% of patients in the goserelin 3.6 mg cohort remained on goserelin treatment while more than half of patients remained on goserelin in the goserelin 10.8 mg cohort.
This study adds to the literature by examining the clinical outcomes of goserelin 10.8 mg versus goserelin 3.6 mg in the real-world setting, which to our knowledge has not been previously examined. The study also used IPTW to balance patient cohorts while observing the differences between dosages, which was necessary because goserelin 3.6 mg has been approved in the treatment of breast cancer in the U.S. for decades and goserelin 10.8 mg is not currently approved in the U.S. for breast cancer.
The results of the non-inferiority analysis are similar to those reported by Noguchi and colleagues, who reported a treatment difference between goserelin 3.6 mg and goserelin 10.8 mg of 1.3% for the 24-week progression-free survival rate in a Phase 3 clinical trial for patients with advanced-stage breast cancer [14]. Our study, which reported 12-month rwEFS rates, showed a treatment difference of 2.7% between the two groups overall and 10.4% for patients with metastatic breast cancer at initial goserelin treatment. The observed non-inferiority of goserelin 10.8 mg in this real-world study may support the use of goserelin 10.8 mg as an alternative treatment option in this patient population.
We observed a longer rwTTD for patients in the goserelin 10.8 mg cohort compared with patients in the goserelin 3.6 mg cohort. A possible reason is the convenience of 3-month intervals (goserelin 10.8 mg) versus 1-month intervals (goserelin 3.6 mg) for treatment administration, making it more practical for patients to continue treatment longer. There may be other factors that could influence a patient’s choice of dosing schedule such as cost, insurance coverage, gauge of needle (larger size of 10.8 mg implant which may lead to injection discomfort), or tolerance to the amount of medication. The longer time to rwTTD for patients who received goserelin 10.8 mg needs to be confirmed in future studies as this outcome was not comparative in nature.
The observed 3-year OS results were slightly lower compared with those reported by Wu and colleagues [9]. For patients with metastatic breast cancer at the time of initial goserelin treatment, our study found that the goserelin 3.6 mg cohort had a 3-year OS rate of 61.1% and those in the goserelin 10.8 mg cohort had a rate of 72.8%. Wu and colleagues reported a 3-year OS rate of 76.6% for patients with advanced-stage breast cancer who received goserelin 3.6 mg in combination with endocrine therapy in China. However, our study included a much larger sample size (698 patients versus 40 patients), and it also included patients who developed distant metastases after initial treatment or who received goserelin 3.6 mg before disease progression. Additionally, the management of patients with HER2-positive disease may differ in the U.S.
The strengths of this study include the use of IPTW to help balance the two cohorts for comparison. The study also included a large sample of patients with breast cancer from a geographically diverse area of the U.S. and had the ability to include patients treated with goserelin 10.8 mg, even though this dosage is not FDA approved in the U.S. IPTW was used to mitigate any potential differences in patient characteristics in those who received goserelin 10.8 mg off-label compared with patients who received goserelin 3.6 mg on-label. Additionally, the study only included patients with at least 360 days of follow-up or death within 360 days. This was necessary to accurately estimate the main study objective, which was the 12-month rwEFS rate. Finally, this study used data created through manual human review, including disease recurrence, which was the main endpoint of this study.
There are several limitations to this study. First, the retrospective nature of this study lends itself to inherent challenges such as data missingness and potential misclassification, and findings should be interpreted with caution. However, potential biases were reduced using both structured and human-reviewed unstructured EMR data. Next, while IPTW was used to help balance the cohorts, other unmeasurable differences may exist between the two cohorts. The study also included patients in the goserelin 10.8 mg cohort who switched to and from goserelin 3.6 mg. Only 28.5% of the goserelin 10.8 mg cohort used goserelin 3.6 mg, and the inclusion criteria required the patients to have started goserelin 10.8 mg within 6 months of initial goserelin treatment. Additionally, our study could not differentiate whether goserelin was prescribed for ovarian function preservation during curative chemotherapy or ovarian function suppression. Finally, this study reflected treatment practice patterns primarily within community oncology practices in the U.S. that are part of the ConcertAI network. As a result, the results may not be generalizable to patients treated in academic settings or outside the U.S.
Conclusion
This U.S.-based real-world analysis indicated that 3-month goserelin 10.8 mg is non-inferior to monthly 3.6 mg in premenopausal patients with breast cancer in terms of 12-month rwEFS rate. These findings are similar to those previously reported in clinical trials and may support the use of the 3-month goserelin 10.8 mg implant as an alternative treatment option for this patient population.
Supplementary Information
Below is the link to the electronic supplementary material.Supplementary file1 (DOCX 112 KB)
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Ter Sera Therapeutics LLC: ZOLADEX® (goserelin implant) 3.6 mg [prescribing information]. https://documents.tersera.com/zoladex-us/3.6mg_Magnum PI.pdf (2023). Accessed September 11, 2024.
- 2Ter Sera Therapeutics LLC: ZOLADEX® (goserelin implant) 10.8 mg [prescribing information]. https://documents.tersera.com/zoladex-us/10.8mg_Magnum PI.pdf (2020). Accessed.
- 3Health Canada: ZOLADEX® LA product monograph. https://health-products.canada.ca/dpd-bdpp/info?lang=eng&code=43433 (2024). Accessed September 11, 2024.
- 4US Food and Drug Administration: Non-inferiority clinical trials to establish effectiveness: Guidance for industry. https://www.fda.gov/media/78504/download (2016). Accessed September 11, 2024.