Sacrospinous Hysteropexy—Video Tutorial of Construction and Application of a Feasible and Inexpensive Teaching Model for Simulation
Greta Lisa Carlin, Wolfgang Umek, Barbara Bodner-Adler, Fanny Carolina Mikula, Sören Lange

TL;DR
This paper introduces a low-cost, easy-to-build model for training in sacrospinous hysteropexy, a uterus-preserving surgery for pelvic organ prolapse.
Contribution
The novelty lies in creating an affordable and reproducible surgical training model using easily accessible materials.
Findings
The model accurately represents key anatomical landmarks for surgical training.
The total cost per model is approximately 2 EUR using readily available materials.
A detailed instructional video and handout are provided to guide trainees through the procedure.
Abstract
Sacrospinous hysteropexy is one of the preeminent uterus-preserving surgical techniques for treating pelvic organ prolapse supported by level one evidence. As training on models greatly improves surgical skills and outcomes, we developed a simple and inexpensive model to simulate sacrospinous hysteropexy. A step-by-step instruction for the production of the model is available to be viewed online. To keep production costs low, readily available materials were used, with a total cost per model of about 2 EUR (Austria, August 2023). All important anatomical landmarks (prolapsing uterus, vagina, ischial spine and sacrospinous ligament) were all represented. We present a detailed instructional video on how to construct the model and the practical training, detailing the individual steps of a successful sacrospinous hysteropexy, available online. Thus, trainees are able to practice the…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1 Figure 2
Figure 2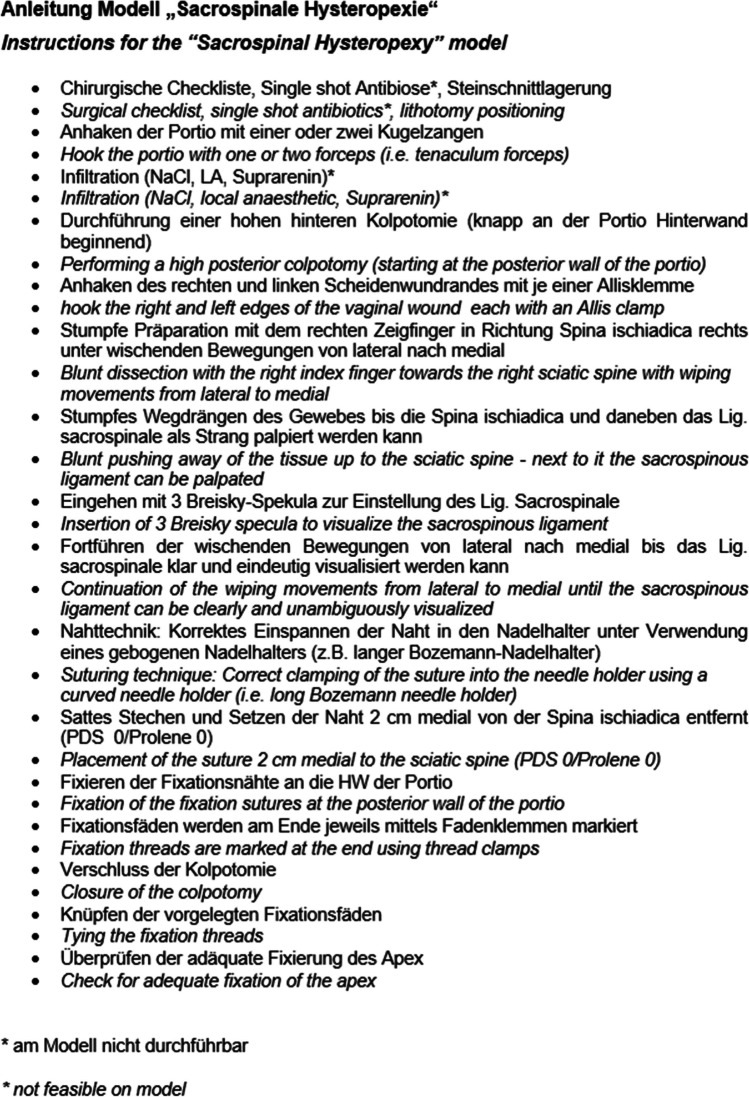 Figure 3
Figure 3- —Medical University of Vienna
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPelvic floor disorders treatments · Pelvic and Acetabular Injuries · Anorectal Disease Treatments and Outcomes
Introduction
Pelvic organ prolapse is a bulging of the vaginal wall into, or out of, the vagina due to a weakness of the pelvis muscles and sagging of one or more pelvic organs. The lifetime risk is high, especially because of an increasingly aging population worldwide, and leads to a significant deterioration of the quality of life. Treatment options range from conservative to various surgical procedures performed laparoscopically, abdominally, or vaginally [1].
Sacrospinous hysteropexy (SSHP) has become a first-line treatment for pelvic organ prolapse based on level one evidence [2]. Compared with vaginal hysterectomy with uterosacral ligament suspension, SSHP was shown to have similar anatomical and subjective outcomes while having a shorter operating time, shorter hospitalisation, and lower intraoperative blood loss [3]. It is therefore an important urogynaecological operating technique for gynaecology trainees to master. However, learning vaginal operating techniques can be challenging, as visualisation of the operating steps performed by the surgeon is rather difficult for an observer, owing to the limited size of the vaginal canal as the primary operating site [4, 5]. Furthermore, surgical skills training using simulators and models has been shown to improve surgical performance, trainees’ confidence levels, and patients’ outcomes in different settings [6, 7]. To date, there have been no simulator models available for vaginal sacrospinous hysteropexy to the best of our knowledge.
Materials and Methods
We set out to construct a simple model to simulate sacrospinous hysteropexy from widely available, inexpensive and sustainable materials on which to easily practice the execution of the individual movements required during a vaginal sacrospinous hysteropexy in correct succession. The full construction of the model from its individual components is demonstrated step by step during the first part of the tutorial video (Supplemental digital content Appendix 1). Materials include a cardboard roll, a sock, loose cotton, felt, rubber stopper and a wooden skewer, all of which are readily available and inexpensive (Fig. 1). All anatomical landmarks relevant during sacrospinous hysteropexy (i.e. vagina, cervix, rectovaginal space, ischial spine and sacrospinous ligament) are represented in the model: the cardboard roll functions as the vaginal canal in which a cotton stuffed sock represents the vaginal wall and prolapsing uterus, attached to which there is a felt cervix. The sock’s loose cotton filling represents the rectovaginal space and a rubber stopper the ischial spine, adjacent to which a felt-covered wooden skewer functions as the sacrospinous ligament. Additionally, a piece of hook-and-loop tape was attached to the finished model so that it could be affixed to a stable surface, allowing for an easier training experience (Fig. 2). Total cost per model was calculated to be as low as 1.85 EUR (central Europe, September 2023), corresponding to about US$2. Construction time per model was measured to be 6 min and 30 s.Fig. 1. Required materials: sock, felt, felt patch, pen, skewer, hook and loop tape, stapler, paper roll, scissors, ruler, attachment site on a stable surfaceFig. 2Finished model
The second part of the video showcases a practical demonstration of the simulator model in use, detailing all necessary steps of a successful sacrospinous hysteropexy, as performed at our institution, demonstrated by an experienced urogynaecology surgeon. First, a high posterior colpotomy towards the posterior cervix is performed, followed by blunt preparation of the rectovaginal space to visualise the sacrospinous ligament. Then, a suture is placed through the ligament and thereafter through the posterior cervical wall, without being knotted yet. Next, the colpotomy is closed, and only afterwards is the pre-laid fixation suture tied, elevating and attaching the cervix towards the sacrospinous ligament.
Results
The model was tested by 52 participants. All received an introduction to the model itself with an exact explanation of all anatomical landmarks. Additionally, a standardised explanation of the surgery’s individual steps was given and a handout detailing them in German (Fig. 3) distributed. After training all participants were asked for feedback by assessing the training they had received on a grading system from 1 to 5 (1 = excellent; 5 = very bad). The results were overwhelming positive.Fig. 3. Handout detailing the surgical steps of sacrospinous hysteropexy in German, with English translation in cursive
Discussion
This instructional video details the construction of a simple, realistic, inexpensive model for the surgical skills training of sacrospinous hysteropexy. It is designed to help increase a trainee’s operative performance by allowing them to practice the execution of each individual step of the surgical procedure. Feedback obtained from users after training was overwhelmingly positive.
Supplementary Information
Below is the link to the electronic supplementary material.Supplementary file1 (MP4 52012 KB)