Case Report: Gastric submucosal neoplasm with CTNNB1 mutation showing GLI1 overexpression and epithelial differentiation
Karin Ashizawa, Tsuyoshi Saito, Yukinori Yube, Shinji Mine, Tetsu Fukunaga, Cristina R. Antonescu, Takashi Yao

TL;DR
A rare gastric tumor with a CTNNB1 mutation and GLI1 overexpression was identified in a 66-year-old man, showing epithelial features and slow growth.
Contribution
This case report describes a novel gastric submucosal neoplasm with CTNNB1 mutation and GLI1 overexpression, distinct from known tumor types.
Findings
The tumor exhibited CTNNB1 mutation (S33C) and diffuse β-catenin nuclear expression.
GLI1 overexpression was observed without gene rearrangements or amplification.
The tumor showed epithelial differentiation and remained stable for 5 years without significant progression.
Abstract
New disease entities have been emerging based on molecular pathological findings, such as pseudoendocrine sarcoma and mesenchymal neoplasm with GLI1 gene alterations, which resemble well-differentiated neuroendocrine tumors. We report a unique case of a gastric submucosal neoplasm of approximately 1.5 cm in size with CTNNB1 mutation showing GLI1 overexpression and epithelial differentiation in a 66-year-old man. It was incidentally identified by routine health screening, and was a slowly growing tumor. Macroscopically, it was a slightly protruded tumor into the mucosa, and was primarily located from the submucosa to the muscularis propria. It was a well-defined lesion measured approximately 20 mm, and was almost stable during almost 5 years after initial identification of the tumor. Uniform round-to-epithelioid cells arranged in solid trabeculae with a microtubular/acinar appearance…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
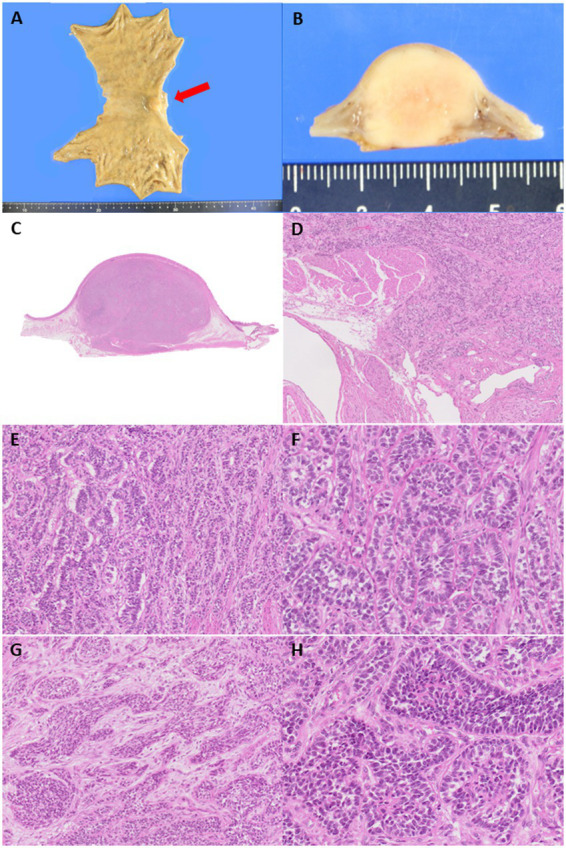 Figure 1
Figure 1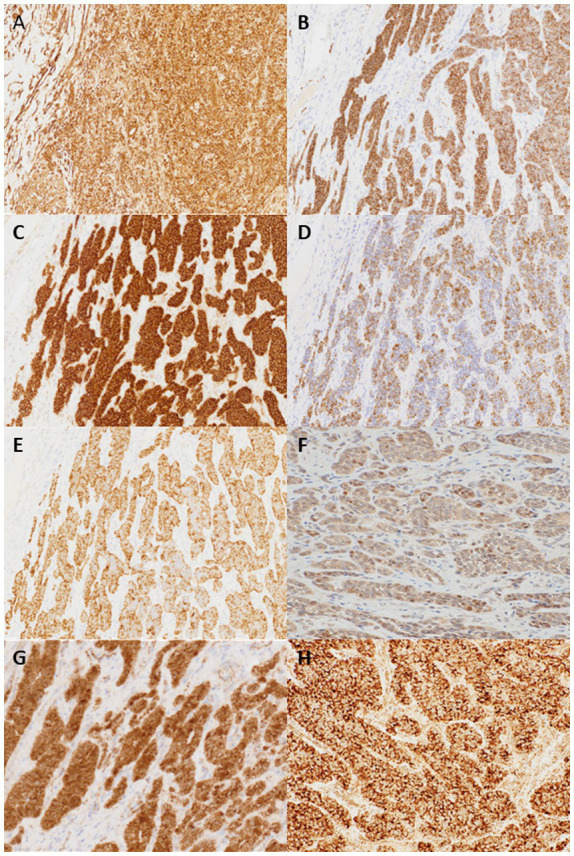 Figure 2
Figure 2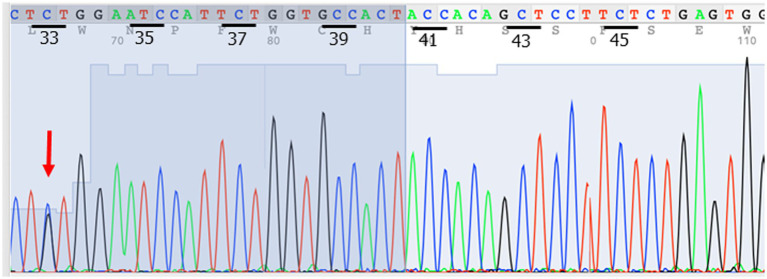 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGastrointestinal Tumor Research and Treatment · Neuroendocrine Tumor Research Advances · Hedgehog Signaling Pathway Studies
Introduction
Molecular pathological research is rapidly advancing, and new disease entities that are based on molecular pathological findings have emerged. For example, disease entities that resemble well-differentiated neuroendocrine tumors, such as pseudoendocrine sarcoma, mesenchymal neoplasms with GLI1 gene alterations described as “distinctive nested glomoid neoplasm,” gastroblastoma, and plexiform fibromyxoma have been reported (1–7). Gastroblastoma is a distinctive biphasic stomach tumor that shows epithelioid or spindle cells and harbors the MALAT::GLI1 fusion gene (5). Pseudoendocrine sarcoma is a recently recognized entity among soft tissue sarcomas, characterized by its close resemblance to well-differentiated neuroendocrine tumors, but lacking epithelial/neuroendocrine differentiation by immunohistochemistry (IHC). Additionally, nearly all cases exhibit aberrant nuclear accumulation of β-catenin caused by the secondary activating hot spot CTNNB1 mutations (1). These lesions commonly occur in deep soft tissues (1–4). These entities are morphologically similar to well-differentiated neuroendocrine tumors, which often makes their diagnosis difficult. Herein, we report a unique case of a gastric submucosal tumor that demonstrated strong expression of monoclonal antibodies directed against keratins in the absence of neuroendocrine differentiation by IHC. However, this case did not fit any of these criteria, and we report it as a gastric submucosal neoplasm with CTNNB1 mutation, showing GLI1 overexpression and epithelial differentiation.
Case presentation
Clinical course
In 2017, a routine health screen incidentally revealed a submucosal gastric tumor in a 66-year-old man. The tumor located on the lesser curvature of the cardia, measuring approximately 1.5 cm, has been monitored since its discovery. Endoscopic ultrasonography (EUS) showed an almost uniform hypoechoic area contiguous to the fourth layer. There was no obvious non-echoic area or blood flow signal. While initially clinically diagnosed as leiomyoma, the possibility of a gastrointestinal stromal tumor was considered. EUS-guided fine needle aspiration (EUS-FNA) in May 2022 revealed a tumor characterized by the monotonous proliferation of epithelioid cells. IHC analysis demonstrated positive staining for CD56 but negative staining for chromogranin A, synaptophysin, and INSM-1. The MIB-1-labeling index (LI) was approximately 2%, which led to the diagnosis of a grade 1 (G1) neuroendocrine tumor, although the immunohistochemical findings were inconsistent. Upon admission, laboratory testing revealed slight abnormalities in renal function. The tumor was expected by EUS to be located in the submucosa and deeper, so the endoscopic resection was considered to be difficult. Therefore, proximal gastrectomy and lymph node dissection was performed by robotic technique in June 2022 as part of the patient’s management. The tumor was located on the lesser curvature of the cardia, allowing resection without confirmation of the tumor location during surgery, despite its small size. The operative time was 5 h and 5 min, with a blood loss of 10 mL. On 10 days after surgery, the patient developed a fever. Gastroendoscopy was performed and it revealed leakage on the left side of the esophageal margin slightly apart from the anastomotic site. Stomach tube was placed for drainage, and a central venous catheter (CV) was inserted. At 1 month after surgery, leakage improved and the drain tube was removed. However, the patient developed a fungal infection and fungal endophthalmitis associated with CV insertion. The patient received intravenous antifungal treatment for additional 1 month, then changed to oral medication. Finally, the patient discharged 2 months post-surgery.
Pathological findings of the surgically resected specimen
Macroscopically, the tumor exhibited a slight protrusion into the mucosa (Figure 1) but was primarily located from the submucosa to the muscularis propria. This well-defined lesion measured approximately 20 mm. Microscopically, the tumor was composed of uniform round-to-epithelioid cells arranged in solid trabeculae with a microtubular/acinar appearance. Tumor cells showed scant eosinophilic cytoplasm and monomorphic round-to-ovoid nuclei with fine chromatin and no pleomorphism. Occasional mitotic figures were observed (1/50 high power fields) and no necrosis was observed. In a few areas, short spindle-shaped cells arranged in tight nests were noted within the fibromyxoid stromal background (Figure 1). Totally, 31 lymph nodes were retrieved and no metastases were identified.
(A) A submucosal-centered tumor with slight protrusion toward the mucosal aspect is identified at the cardia and lesser curvature (red arrow). (B) The cut surface of the tumor shows a well-demarcated, white-yellow solid lesion measuring 20 mm in the largest dimension. (C) The tumor extends from the submucosa to the muscularis propria. (D,E) Tumor cells are arranged in microacinar and trabecular architectural arrangements without necrosis, reminiscent of a well-differentiated neuroendocrine tumor. The tumor mainly appeared well-demarcated but irregularly infiltrated the surrounding tissue in a few areas. (F) Tumor cells are monomorphic and exhibited scant, pale eosinophilic cytoplasm, round nuclei, and speckled chromatin. Occasional rosette-like structural formations are observed, similar to those observed in well-differentiated neuroendocrine tumors. (G) In a few areas, short, spindle-shaped cells arranged in tight nests are observed within the fibromyxoid stroma. (H) Tumor cells form solid sheets with small amounts of hyalinized stromal bodies.
IHC analysis revealed that the tumor cells were diffusely positive for vimentin, CD56, CD10, CAM5.2, AE1/AE3, estrogen receptor (ER), progesterone receptor (PgR) and androgen receptor (AR), STAT6 (cytoplasmic), and focally positive for S-100, E-cadherin, cyclinD1 and ATRX, whereas they were negative for chromogranin A, synaptophysin, INSM-1, smooth muscle antibody, c-kit, calretinin, epithelial membrane antigen, inhibin, SALL4, AFP, Glypican-3, p53, p40, CD34, bcl-10, SF-1, PAX-8, CDX2, CD99, MelanA, CEA, CA19-9, and CA125 (Figure 2). As this immune profile was deemed nondiagnostic for neuroendocrine neoplasms, further molecular studies were performed. As one of the primary differential diagnoses was gastroblastoma, RT-PCR for MALAT1::GLI1 fusion was performed, which yielded a negative result. Furthermore, DDIT3/GLI1 FISH analysis was negative for GLI1 gene rearrangements, and targeted RNA sequencing using the Illumina TruSight panel (500 genes) was negative for gene fusion candidates. RNA sequencing was predominantly performed to identify gene fusions rather than mutations, and coincidentally, manual inspection revealed a 10-fold increase in the mRNA expression of STAT6 and GLI1; however, no gene amplification was detected by FISH. Additional IHC showed focal and weak staining for GLI1 of uncertain significance.
Tumor cells are positive for vimentin (A), CD56 (B), CD10 (C), CAM5.2 (D), AE1/3 (E). Focal and weak nuclear staining for GLI1 (F) and cytoplasmic and partial nuclear staining for β-catenin (G) are also noted. STAT6 IHC shows cytoplasmic staining but not nuclear staining (H) (×200).
The next possibility to be considered was a pseudoendocrine sarcoma. β-catenin immunostaining was performed, which showed aberrant nuclear expression (Figure 2). This result was further confirmed by Sanger sequencing, which showed a hot spot CTNNB1 mutation (S33C) (Figure 3). Consistent with these results was the tumor content of 80% in this case, which equated to an allele frequency of the CTNNB1 mutation (S33C) of 40%. Therefore, the CTNNB1 mutation was deemed to be clonal.
Sanger sequencing confirmed the CTNNB1 mutation (S33C) (red arrow).
Discussion
Gastric mesenchymal tumors are rare, with gastrointestinal stromal tumors, schwannomas, and leiomyomas being the most common. Based on the histological features observed in the initial biopsy, a diagnosis of a well-differentiated neuroendocrine tumor was considered; however, the IHC findings were not fully supportive. Gastric neuroendocrine neoplasms typically exhibit positive immunohistochemical staining for chromogranin A, synaptophysin, and INSM-1. In contrast, IHC findings suggested the possibility of gastroblastoma (5). However, gastroblastomas, similar to synovial sarcomas, usually exhibit a biphasic pattern characterized by a mixture of spindle cells and nests of epithelioid cells with abundant eosinophilic cytoplasm. These features were not observed in the present case. In addition, RT-PCR, FISH, and RNA sequencing failed to identify the presence of GLI1 gene rearrangements, MALAT1::GLI1 fusion, PTCH1::GLI1 fusion, or an EWSR1-CTBP1, recently identified in a patient with Wiskott-Aldrich syndrome (6, 8). Therefore, a diagnosis of gastroblastoma was excluded. The next possibility was a pseudoendocrine sarcoma. CTNNB1 mutation and nuclear expression for β-catenin IHC are consistent with pseudoendocrine sarcoma; however, these sarcomas occur commonly in the truncal locations such as the soft tissues of the vertebral body region and posterior head (1), so the site, in this case, did not fit pseudoendocrine sarcoma. In addition, short spindle cells arranged in tight nests were observed within a fibromyxoid stromal background that did not fit pseudoendocrine sarcoma. The case also showed focal and weak staining expression of GLI1 on IHC and monoclonal antibodies directed against keratins, such as CAM5.2 and AE1/AE3, although prior studies have not reported any positive staining for monoclonal antibodies directed against keratins and GLI1 on IHC (1, 2, 9). Based on these findings, the diagnosis of pseudoendocrine sarcoma was excluded.
The presence of the CTNNB1 mutation and the morphological similarity in this case may raise the possibility of a solid pseudopapillary neoplasm or Sertoli-like neoplasm, such as a Sertoli cell tumor of the testis. However, ectopic pancreatic tissue was not observed in the present case. Furthermore, the absence of a history of gonadal systemic tumors and no abnormalities in the gonads on PET-CT ruled out this possibility. However, the overexpression of hormone receptors such as ER, PgR, and AR in this case remains puzzling.
The possibility of a mesenchymal neoplasm with GLI1 gene alterations was raised because of GLI1 mRNA and protein overexpression (7). Recent studies have highlighted the morphological similarities between well-differentiated neuroendocrine tumors and soft tissue sarcomas with GLI1 gene alterations described as “distinctive nested glomoid neoplasm” (1, 7, 10, 11). However, it was excluded because of the absence of GLI1 fusion and the presence of the CTNNB1 mutation. Furthermore, irregular fibrous septa, lobular growth patterns, a prominent capillary network, or lobules protruding into vascular lumina beneath intact endothelium are frequently seen in distinctive nested glomoid neoplasms, but were not observed in this case. A study by Parrack et al. reported that GLI1 IHC was highly sensitive (91.3%) and specific (98.0%) for mesenchymal tumors with driver GLI1 alterations among morphological mimics (9). However, in this case, GLI1 IHC was focally and weakly positive rather than diffusely and strongly positive, which does not positively support a GLI1-altered mesenchymal neoplasm.
Furthermore, the strong and diffuse cytokeratin expression in this case seemed unusual for a GLI1-altered mesenchymal neoplasm (12). Since this case does not fit the disease concepts reported to date, we report it as “gastric submucosal neoplasm with CTNNB1 mutation showing GLI1 overexpression and epithelial differentiation.”
Regarding the prognosis of this case, the patient was followed up for almost 5 years without any treatment before undergoing surgery, during which the tumor size remained relatively stable. The MIB-1 proliferation index in the surgical specimen was approximately 5%, and the patient survived for 2 years without any evidence of recurrence or metastasis after surgery. Gastroendoscopy has been performed every year after surgery, and no new lesions are observed. These outcomes show the slow growth and low-grade nature of this tumor. This case report provides new insights into the clinicopathological characteristics of this disease.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Papke DJ Jr Dickson BC Sholl L Fletcher CDM. Pseudoendocrine sarcoma: Clinicopathologic analysis of 23 cases of a distinctive soft tissue neoplasm with metastatic potential, recurrent CTNNB 1 mutations, and a predilection for truncal locations. Am J Surg Pathol. (2022) 46:33–43. doi: 10.1097/PAS.0000000000001751, PMID: 34081037 · doi ↗ · pubmed ↗
- 2Vizcaino MA Folpe AL Huffman H Panchal RR Nielsen GP Kipp BR. Pseudoendocrine sarcoma: clinicopathologic, molecular, and epigenetic features of one case. Virchows Arch. (2023) 483:899–904. doi: 10.1007/s 00428-023-03695-3, PMID: 37953374 · doi ↗ · pubmed ↗
- 3Bellan E Zanco F Baciorri F Toffolatti L Dei Tos AP Sbaraglia M. Case report: pseudoendocrine sarcoma, a clinicopathologic report of a newly described soft tissue neoplasm. Virchows Arch. (2023) 482:1057–63. doi: 10.1007/s 00428-022-03476-4, PMID: 36564514 · doi ↗ · pubmed ↗
- 4Moran JMT Hung YP Selig MK Nielsen GP. Meningioma-like ultrastructural features of Pseudoendocrine sarcoma. Am J Surg Pathol. (2022) 46:1014–6. doi: 10.1097/pas.0000000000001890, PMID: 35297787 · doi ↗ · pubmed ↗
- 5Graham RP Nair AA Davila JI Jin L Jen J Sukov WR. Gastroblastoma harbors a recurrent somatic MALAT 1-GLI 1 fusion gene. Mod Pathol. (2017) 30:1443–52. doi: 10.1038/modpathol.2017.68, PMID: 28731043 · doi ↗ · pubmed ↗
- 6Koo SC La Haye S Kovari BP Schieffer KM Ranalli MA Aldrink JH. Gastroblastoma with a novel EWSR 1-CTBP 1 fusion presenting in adolescence. Genes Chromosomes Cancer. (2021) 60:640–6. doi: 10.1002/gcc.22973, PMID: 34041825 · doi ↗ · pubmed ↗
- 7Papke DJ Jr Dickson BC Oliveira AM. Distinctive nested Glomoid neoplasm: Clinicopathologic analysis of 20 cases of a mesenchymal neoplasm with frequent GLI 1 alterations and indolent behavior. Am J Surg Pathol. (2023) 47:12–24. doi: 10.1097/pas.0000000000001979, PMID: 36395474 · doi ↗ · pubmed ↗
- 8Chen C Lu J Wu H. Case report: submucosal gastroblastoma with a novel PTCH 1::GLI 2 gene fusion in a 58-year-old man. Front Oncol. (2022) 12:935914. doi: 10.3389/fonc.2022.935914, PMID: 36147912 PMC 9487307 · doi ↗ · pubmed ↗