Small bowel metastasis from endometrial cancer presenting as a bowel obstruction: A case report with literature review
Yasuhiko Hamada, Hiroki Yukimoto, Yohei Ikenoyama, Yuhei Umeda, Yasuko Fujiwara, Akina Shigefuku, Hiroto Suzuki, Misaki Nakamura, Noriyuki Horiki, Hayato Nakagawa

TL;DR
A rare case of endometrial cancer spreading to the small bowel six years after initial treatment is reported, emphasizing the importance of early detection and proper diagnosis.
Contribution
This case highlights the diagnostic value of balloon-assisted enteroscopy and immunohistochemical profiling in identifying rare small bowel metastases from endometrial cancer.
Findings
Balloon-assisted enteroscopy identified a metastatic lesion in the jejunum six years after initial endometrial cancer treatment.
Immunohistochemical analysis confirmed the metastasis as endometrial adenocarcinoma with specific marker positivity.
The patient experienced symptom relief post-surgery with no further metastases detected.
Abstract
This report describes a rare case of small bowel metastasis from endometrial cancer, diagnosed six years after initial treatment. A 62‐year‐old woman with a history of grade 2 stage IA endometrial cancer, previously treated with hysterectomy and bilateral salpingo‐oophorectomy, presented with intermittent abdominal pain and nausea. Imaging studies revealed small bowel obstruction and balloon‐assisted enteroscopy identified an annular ulcer with luminal narrowing in the jejunum. Histopathological examination of the biopsy specimen suggested carcinoma; however, its primary origin remained unclear. Subsequent surgical resection confirmed metastatic endometrial adenocarcinoma based on immunohistochemical analysis, which demonstrated positivity for estrogen receptor and paired box gene 8, while CK7, CK20, and CDX2 were negative. Following surgery, the patient experienced symptomatic relief,…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 FIGURE 1
FIGURE 1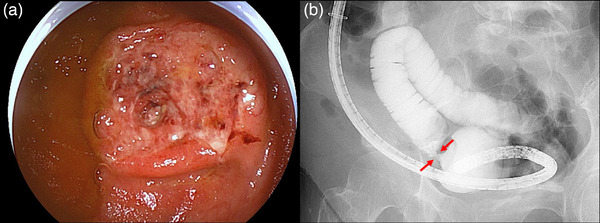 FIGURE 2
FIGURE 2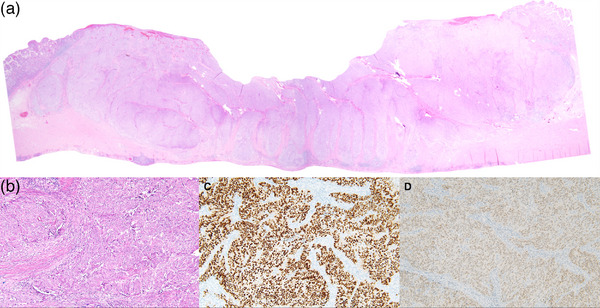 FIGURE 3
FIGURE 3|
Case No. | Author | Year | Patient age (years) |
Initial stage |
Time period from primary surgery |
Clinical symptom | Endoscopy | Metastatic site in the small bowel | Metastatic lesion outside the small bowel | Treatment of small bowel lesion |
|---|---|---|---|---|---|---|---|---|---|---|
| 1 | Bosscher et al. | 1994 | 55 | IVB | 0 month | Not available | No | Proximal ileum | No |
Small bowel resection |
| 2 | Kirk et al. | 1999 | 64 | Not described | 10 months | Abdominal pain Melena | No | Mid‐ileum | Spleen |
Small bowel resection |
| 3 | Thijs et al. | 2007 | 85 | IIIB | 24 months |
Anemia Melena | Capsule endoscopy | Small bowel | Not described |
Small bowel resection |
| 4 | Tsai et al. | 2007 | 67 | Early stage | 96 months | Abdominal pain Melena | Upper endoscopy | Duodenum | No |
Segmental duodenectomy |
| 5 | Gallotta et al. | 2015 | 58 | IB | 13 months | Not described | No | Small bowel | Vaginal cuff |
Small bowel resection |
| 6 | Hubers et al. | 2017 | 75 | IB | 36 months | Hematochezia | No |
Proximal jejunum | Sigmoid colon |
Small bowel resection |
| 7 | Leitão et al. | 2017 | 72 | Not described | 60 months | Melena | Upper endoscopy | Duodenum |
Paraaortic mass |
Palliative chemotherapy |
| 8 | Makki et al. | 2019 | 88 | Not described | 5 months |
Anemia Abdominal pain | No | Mid‐jejunum | Mesenteric lymph node |
Small bowel resection |
| 9 | Huynh et al. | 2019 | Not described | Not described | 36 months | Back pain | Upper endoscopy | Duodenum |
Retroperitoneal mass |
Duodenal resection |
| 10 | Singh et al. | 2019 | 77 | IA | 41 months |
Melena Anemia | Upper endoscopy | Duodenum | Retroperitoneal mass | Radiotherapy |
| 11 | Emiloju et al. | 2020 | 60 | Not described | 10 months | Abdominal pain Anemia | Upper endoscopy | Duodenum | No |
Pancreatico‐ duodenectomy |
| 12 | Nikolvski et al. | 2024 | 88 | II | 14 months | Cutaneous fistula | No | Mid‐ileum | No |
Small bowel resection |
| 13 | Present case | 2025 | 62 | IA | 72 months | Abdominal pain Vomiting |
Balloon‐assisted enteroscopy |
Distal jejunum | No |
Small bowel resection |
- —None.
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsMetastasis and carcinoma case studies · Gastric Cancer Management and Outcomes · Gastrointestinal Tumor Research and Treatment
INTRODUCTION
Metastatic tumors of the small bowel are rare and can originate from various primary malignancies, including those of the lung, kidney, skin, and stomach.1 These tumors often present with clinical manifestations, such as anemia, gastrointestinal bleeding, obstruction, or perforation. Balloon‐assisted enteroscopy plays a critical role in the diagnosis and surgical planning of metastatic small bowel tumors by enabling histopathological confirmation or precise tumor localization.1
Endometrial cancer is the fourth most common malignancy among women worldwide.2 While early‐stage disease is associated with a favorable prognosis and a low recurrence rate, late recurrences and metastases have been reported in various locations years after initial treatment.3 However, metastasis to the small bowel is rare, and its true incidence remains undetermined due to its rarity and the frequently asymptomatic nature of the disease until advanced stages.4
Here, we present a rare case of small bowel metastasis from endometrial cancer, detected by balloon‐assisted enteroscopy six years after the initial surgical treatment.
CASE REPORT
A 62‐year‐old female patient presented with a 5‐month history of intermittent abdominal pain and nausea, and was referred to our hospital for further evaluation. The patient had a 20‐pack‐year smoking history but had quit 15 years prior. She also had a history of endometrial cancer (endometrioid adenocarcinoma) for which she was treated with a modified radical hysterectomy and bilateral salpingo‐oophorectomy 6 years earlier. The tumor exhibited no myometrial invasion, cervical stromal invasion, lymph node metastasis, or positive peritoneal cytology, and was classified as grade 2, stage IA cancer according to the International Federation of Gynecology and Obstetrics classification.5
On admission, the patient was afebrile, and her vital signs were within normal limits. Physical examination revealed diffuse abdominal tenderness without signs of peritoneal irritation, such as voluntary guarding or rebound tenderness. Laboratory investigations, including complete blood count, liver function tests, renal function tests, and C‐reactive protein levels, were unremarkable. Tumor markers, including CEA, CA19‐9, and CA125, were within the normal range and showed no significant changes over time. Contrast‐enhanced abdominal computed tomography revealed small bowel wall thickening with proximal loop dilatation, indicative of small bowel obstruction (Figure 1a, coronal image; Figure 1b, sagittal image, arrows). No other significant lesions were identified. The patient was initially treated with ileus tube placement. Following the resolution of the bowel obstruction, antegrade balloon‐assisted enteroscopy was performed for diagnostic purposes. The enteroscopy detected a submucosal tumor‐like protruded lesion with luminal narrowing in the jejunum (Figure 2a). Small bowel radiography through the enteroscopy demonstrated an annular stenosis (Figure 2b, arrows). The lesion was biopsied and marked at a site proximal to the lesion by inking. Retrograde balloon‐assisted enteroscopy, in conjunction with small bowel radiography, did not reveal any additional small bowel lesions. Based on the endoscopic findings and imaging studies, the differential diagnosis included malignant lymphoma, metastatic tumors from other organs, and atypical primary small bowel cancer. Initial biopsies of the lesion demonstrated atypical cells that were positive for CK‐AE1/AE3 on immunohistochemical staining, raising suspicion of adenocarcinoma; however, the tissue of origin remained inconclusive. Therefore, a partial resection of the small bowel (proximal jejunum) was performed for diagnostic and therapeutic purposes. Pathological examination of the resected specimen revealed tumor cells arranged in solid and cribriform patterns, extending from the mucosa to the subserosa (Figure 3a,b). Immunohistochemical staining demonstrated that the tumor cells were positive for estrogen receptor (Figure 3c) and paired box gene 8 (Figure 3d) and negative for CK7, CK20, and CDX2. Considering these findings and the patient's history of endometrial cancer, she was ultimately diagnosed with a solitary metastatic small bowel tumor secondary to the endometrial cancer. The patient experienced significant symptom improvement following surgical resection and was discharged 7 days postoperatively. Positron emission tomography/computed tomography revealed no other metastatic lesions. After a thorough discussion, the patient opted for close follow‐up without additional treatment. No recurrence was observed four months after surgical resection.
Contrast‐enhanced abdominal computed tomography showing a small bowel wall thickening with proximal loop dilatation (a: coronal image, b: sagittal image, arrows).
Balloon‐assisted enteroscopy showing an annular ulcer with luminal narrowing in the jejunum (a). Small bowel radiography through the enteroscopy showing an annular stenosis (b, arrows).
Pathological findings of the resected specimen. Hematoxylin and eosin staining showing that tumor cells are arranged in solid and cribriform patterns, extending from the mucosa to the subserosa (a, original magnification ×12.5, b, original magnification ×100). Immunohistochemical staining (original magnification ×100) showing that the tumor cells were positive for estrogen receptor (c) and paired box gene 8 (d).
DISCUSSION
The most common sites of metastasis or recurrence in endometrial cancer are the pelvic and para‐aortic lymph nodes.4 Other typical metastatic sites include the cervix, vagina, peritoneum, and lungs. However, metastasis to the small bowel is extremely rare. The proposed mechanisms of small bowel metastasis secondary to endometrial cancer include: (1) invasion into the small bowel parenchyma via lymphatic metastasis to peri‐small bowel lymph nodes, (2) hematogenous metastasis, (3) peritoneal dissemination, and (4) direct invasion from adjacent organs.6 In the present case, no lymph node metastasis was observed in the pelvic or para‐aortic regions at the time of the initial surgery, nor were there findings suggestive of carcinomatous peritonitis during the current surgery. Therefore, hematogenous spread was considered the most likely pathway of metastasis rather than lymphatic or peritoneal dissemination. Regarding the possible hematogenous route, venous drainage from the uterus flows into the internal iliac vein via the venous plexus, suggesting the inferior vena cava as a potential pathway. However, given the rarity of solitary small bowel metastases from endometrial cancer, further case accumulation is necessary for a more comprehensive understanding.
Takahashi et al. analyzed the reported recurrence factors, including older age (>60 years), tumor grade G3, cervical stromal invasion, and positive peritoneal cytology, and developed a novel recurrence prediction score.7 Based on this prediction score, the current case exhibited a low recurrence risk. However, reported cases of small bowel metastasis from endometrial cancer included cases with low recurrence risk, warranting careful follow‐up even in these cases.
A systematic MEDLINE search of the English‐language literature up to 2024 using the keywords “endometrial cancer,” “endometrial carcinoma”, “small bowel,” “small intestine,” and “metastasis” identified 13 studies, including the present case, documenting small bowel metastases from endometrial cancer (Table 1; reference articles are listed in Doc S1). The timing of metastasis onset varies considerably, ranging from immediately after the initial surgery to as long as 96 months postoperatively. These metastases are often asymptomatic until the disease reaches an advanced stage and typically present with nonspecific symptoms, such as abdominal pain, anemia, and melena. Consequently, a substantial delay exists from symptom onset to diagnosis and definitive identification.
Reports on endoscopic findings are limited, particularly for lesions distal to the ligament of Treitz. To date, only a single case has been documented using capsule endoscopy, which revealed luminal narrowing, similar to the findings in the present case.3 However, metastatic small intestinal tumors exhibit diverse endoscopic features, making definitive diagnosis based solely on endoscopic findings challenging. Therefore, immunohistochemical analysis plays a crucial role in achieving an accurate diagnosis. While primary bowel adenocarcinomas typically express CDX2, CK7, and CK20, endometrial adenocarcinomas are negative for CDX2 and CK20. CK7 is generally positive in endometrial cancer; however, it is negative in approximately 10% of cases, including the present case.8 Estrogen receptor and paired box gene 8 are often positive, and notably, paired box gene 8 serves as a useful diagnostic marker for identifying tumors of Müllerian duct origin.9
Surgical resection has been the primary treatment modality in previously reported cases, primarily to alleviate symptoms. A previous meta‐analysis showed that complete resection of the tumor is the only significant prognostic factor for improving outcomes in recurrent endometrial cancer.10 However, the optimal management following cytoreductive surgery remains inconclusive. A comprehensive approach is required, incorporating radiotherapy, systemic chemotherapy, or observation without further intervention, while considering the patient's health status, metastasis, time interval from primary treatment to recurrence, and initial treatment modality. In the present case, positron emission tomography/computed tomography did not reveal any additional recurrent lesions. Moreover, a meta‐analysis indicated that adjuvant chemotherapy is negatively associated with survival.10 Therefore, after a thorough discussion with the patient, we opted for close follow‐up without additional treatment.
In conclusion, endoscopists should maintain a high index of suspicion for metastatic small bowel tumors originating from endometrial cancer to facilitate timely diagnosis and prompt treatments.
CONFLICT OF INTEREST STATEMENT
None.
ETHICS STATEMENT
All procedures were performed in accordance with the ethical standards of the Declaration of Helsinki and its later amendments.
PATIENT CONSENT STATEMENT
Informed consent was obtained from the patient for the publication of this case report.
Supporting information
Reference articles in Table 1
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Nishimura N , Mizuno M , Shimodate Y et al. The role of Double‐balloon enteroscopy in the diagnosis and surgical treatment of metastatic small bowel tumors. Intern Med 2018; 57: 1209–1212.29279517 10.2169/internalmedicine.9877-17PMC 5980799 · doi ↗ · pubmed ↗
- 2Bray F , Laversanne M , Sung H et al. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA: A Cancer Journal for Clinicians 2024; 74: 229–263.38572751 10.3322/caac.21834 · doi ↗ · pubmed ↗
- 3Thijs W , Karrenbeld A , van der Zouwen LS et al. Metastatic endometrial cancer; A rare intestinal localization. Endoscopy 2007; 39 (Suppl 1): E 131.17611883 10.1055/s-2007-966372 · doi ↗ · pubmed ↗
- 4Huynh KN , Nguyen BD , Wu KJ . Gastrointestinal: Caval tumor thrombus and duodenal metastasis from endometrial carcinoma. J Gastroenterol Hepatol 2019; 34: 309.30136307 10.1111/jgh.14411 · doi ↗ · pubmed ↗
- 5Berek JS , Matias‐Guiu X , Creutzberg C et al. FIGO staging of endometrial cancer: 2023. Int J Gynaecol Obstet 2023; 162: 383–394.37337978 10.1002/ijgo.14923 · doi ↗ · pubmed ↗
- 6Caramella E , Bruneton JN , Roux P et al. Metastases of the digestive tract. Report of 77 cases and review of the literature. Eur J Radiol 1983; 3: 331–338.6653567 · pubmed ↗
- 7Takahashi K , Yunokawa M , Sasada S et al. A novel prediction score for predicting the baseline risk of recurrence of stage I‐II endometrial carcinoma. J Gynecol Oncol 2019; 30: e 8.30479092 10.3802/jgo.2019.30.e 8PMC 6304400 · doi ↗ · pubmed ↗
- 8Dum D , Menz A , Völkel C et al. Cytokeratin 7 and cytokeratin 20 expression in cancer: A tissue microarray study on 15,424 cancers. Exp Mol Pathol 2022; 126: 104762.35390310 10.1016/j.yexmp.2022.104762 · doi ↗ · pubmed ↗