Magnetic guided stereotactic radioablation for mid-wall ventricular tachycardia: how to overcome limits of catheter ablation
Michele Magnocavallo, Pietro Rossi, Domenico Marchesano, Stefano Bianchi

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
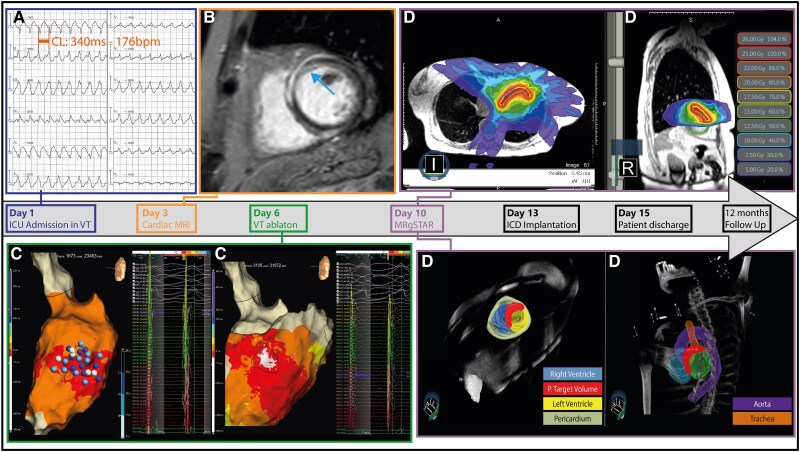 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCardiac Arrhythmias and Treatments · Atrial Fibrillation Management and Outcomes · Cardiac pacing and defibrillation studies
Case description
A 64-year-old female was admitted to our intensive care unit for incessant ventricular tachycardia (VT) unresponsive to antiarrhythmic medication (beta-blocker plus amiodarone) (Figure 1A). Cardiac magnetic resonance imaging (MRI) revealed a preserved left ventricular function with an ejection fraction of 60% and a basal antero-septal mid-myocardial late gadolinium enhancement (Figure 1B). Ultra-high-density left ventricular endo-epicardial maps with the HD grid catheter (Abbott, Minneapolis, USA) performed in sinus rhythm did not show low voltage areas and fragmented/prolonged electrograms; VT activation map identified only the exit site of the tachycardia, and it remained inducible despite multiple radiofrequency applications performed at 50 W using the Tactiflex catheter (Figure 1C).
Workflow for magnetic resonance guided sterotactic arrhythmia radioablation (MRgSTAR). Radiotherapy target was achieved by combining electrophysiological [ECG (Panel A), electroanatomic maps (Panel C—Blue dots represent the ablation lesions)] and anatomical/functional [cardiac MRI—blue arrow showed a basal antero-septal mid-myocardial scar (Panel B)] data. A multi-disciplinary team (radiation oncologist, electrophysiologist, and cardiac radiologist) delineated the CTV and planned target volume was obtained, adding a 2–3 mm margin to the target area (Panel D). CTV, clinical target volume; MRI, magnetic resonance imaging.
Considering the acute VT recurrence after catheter ablation, the clinical implication of a partial diastolic pathway mapping^1^ and the lack of a well-established strategy for the treatment of arrhythmias originating from mid-wall substrate, we planned a magnetic resonance guided sterotactic arrhythmia radioablation (MRgSTAR). We delineated the clinical target volume (CTV)—antero-septal scar—and the planning target volume was obtained by adding a 2–3 mm margin to the CTV (Figure 1D). Radiotherapy energy (25 Gy) was delivered on the CTV, and a sagittal cine MRI was performed during the whole delivery time (see Supplementary material online, Video S1). ICD implantation was performed after MRgSTAR and the patient was discharged 2 days later. Genetic test revealed a LMNA gene mutation [c.185G > T;p.(Arg62Leu)] and ICD interrogation at 12-months after MRgSTAR did not show VT recurrence.
STAR was introduced for the treatment of VT refractory to catheter ablation and demonstrated a strong reduction in the arrhythmia burden.^2^ However, no data are available for patients with mid-myocardial scar. In this scenario, radiotherapy energy seems to provide changes in conduction tissue properties and myolisis acutely and after months myocardial fibrosis.^3^ For these reasons, MRgSTAR may represent a safe and effective strategy for the treating of these patients.
Supplementary Material
ytaf158_Supplementary_Data
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Hadjis A, Frontera A, Limite LR, Bisceglia C, Bognoni L, Foppoli L, et al Complete electroanatomic imaging of the diastolic pathway is associated with improved freedom from ventricular tachycardia recurrence. Circ Arrhythm Electrophysiol 2020;13:e 008651.32755381 10.1161/CIRCEP.120.008651 PMC 7495983 · doi ↗ · pubmed ↗
- 2Cuculich PS, Schill MR, Kashani R, Mutic S, Lang A, Cooper D, et al Noninvasive cardiac radiation for ablation of ventricular tachycardia. N Engl J Med 2017;377:2325–2336.29236642 10.1056/NEJ Moa 1613773 PMC 5764179 · doi ↗ · pubmed ↗
- 3Kautzner J, Jedlickova K, Sramko M, Peichl P, Cvek J, Ing LK, et al Radiation-induced changes in ventricular myocardium after stereotactic body radiotherapy for recurrent ventricular tachycardia. JACC Clin Electrophysiol 2021;7:1487–1492.34600851 10.1016/j.jacep.2021.07.012 · doi ↗ · pubmed ↗