Lymphoedema Development Following a Cancer Diagnosis: An Anonymised Data Linkage Study in Wales, United Kingdom
Ioan Humphreys, Alan Watkins, Ashley Akbari, Rowena Griffiths, Marie Gabe‐Walters, Melanie Thomas, Cheryl Pike, Angela Williams, Tom Dobbs, John Gibson, Iain S. Whitaker, Hayley A. Hutchings

TL;DR
This study examines how cancer diagnoses in Wales are linked to lymphoedema development and finds that cancer type strongly influences the time to lymphoedema diagnosis.
Contribution
The study identifies cancer type as the most significant factor affecting the time to lymphoedema development after cancer diagnosis.
Findings
7538 cases of lymphoedema were identified following cancer diagnoses in Wales.
Breast cancer patients developed lymphoedema the fastest, likely due to surgical interventions.
Cancer type was the strongest predictor of time to lymphoedema diagnosis.
Abstract
This observational cohort study explored lymphoedema development following a cancer diagnosis and whether demographic factors impacted the time to lymphoedema development. We identified cases through the Secure Anonymised Information Linkage (SAIL) Databank. We used cancer diagnostic codes to identify a cohort of six broad cancer ‘types’. We independently used lymphoedema diagnostic codes to identify a cohort who developed lymphoedema. We linked these two cohorts to develop a single cohort of cases and describe the number of cases who went on to develop lymphoedema after a cancer diagnosis, and the time to lymphoedema diagnosis. We used Cox regression models to calculate hazard ratios and produced survival curves to explore whether pre‐defined factors (gender, age, deprivation, cancer type) had any impact on time to lymphoedema development. We identified 7538 cases of lymphoedema…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
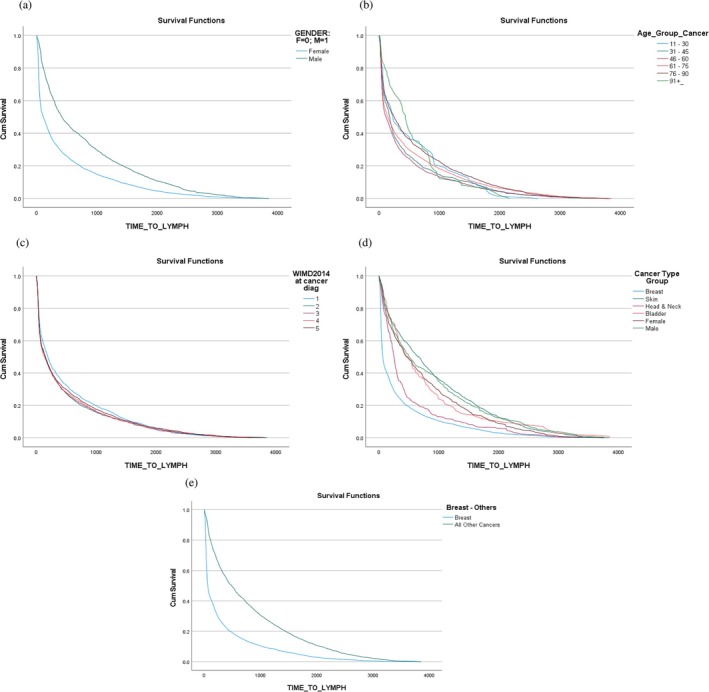 FIGURE 1
FIGURE 1| Sail data source | Data source full name | Data source link |
|---|---|---|
| ADDE | Annual District Death Extract |
|
| PEDW | Patient Episode Database for Wales |
|
| WDSD | Welsh Demographic Service Dataset |
|
| WLGP | Welsh Longitudinal General Practice |
|
| WCSU | Welsh Cancer Intelligence and Surveillance Unit |
|
| Factor |
|
|---|---|
| Gender | |
| Female | 6148 (84.5%) |
| Male | 1131 (15.5%) |
| Age group (years) | |
| 11–30 | 63 (0.9%) |
| 31–45 | 637 (8.8%) |
| 46–60 | 2287 (31.4%) |
| 61–75 | 2902 (39.9%) |
| 76–90 | 1341 18.4(%) |
| 91+ | 49 (0.7%) |
| WIMD quintile ( | |
| 1 (most deprived) | 1146 (16.2%) |
| 2 | 1390 (19.7%) |
| 3 | 1412 (20.0%) |
| 4 | 1430 (20.3%) |
| 5 (least deprived) | 1680 (23.8%) |
| Cancer type | |
| Breast | 4874 (67.0%) |
| Skin | 1051 (14.4%) |
| Head & neck | 334 (4.6%) |
| Bladder | 100 (1.4%) |
| Female specific | 575 (7.9%) |
| Male specific | 345 (4.7%) |
| Cancer type | |
| Breast | 4874 (67.0%) |
| ‘Other’ | 2405 (33.0%) |
| Factor | Time between diagnoses (percentiles) | Hazard ratio (unadjusted) | Figure | ||||
|---|---|---|---|---|---|---|---|
| 25th | 50th | 75th | Estimate |
| (95% CI) | ||
| Gender | |||||||
| Female | 34 | 108 | 530 |
| 1(a) | ||
| Male | 147 | 419 | 1179 | 0.621 | < 0.001 | (0.583, 0.662) | |
| Age (years) | |||||||
| All | n/a | n/a | n/a | 0.994 | < 0.001 | (0.992, 0.996) | n/a |
| Age group (years) | |||||||
| 11–30 | 60 | 224 | 896 | n/a | n/a | n/a | 1(b) |
| 31–45 | 39 | 169 | 544 | ||||
| 46–60 | 35 | 111 | 470 | ||||
| 61–75 | 37 | 143 | 698 | ||||
| 76–90 | 47 | 244 | 891 | ||||
| 91+ | 141 | 432 | 835 | ||||
| WIMD quintile | |||||||
| 1 | 43 | 190 | 742 |
| 1(c) | ||
| 2 | 38 | 149 | 567 | 1.086 | 0.038 | (1.005, 1.175) | |
| 3 | 36 | 150 | 579 | 1.094 | 0.023 | (1.012, 1.183) | |
| 4 | 36 | 134 | 618 | 1.097 | 0.019 | (1.015, 1.186) | |
| 5 | 38 | 147 | 672 | 1.055 | 0.164 | (0.978, 1.137) | |
| Cancer type | |||||||
| Breast | 31 | 62 | 330 |
| |||
| Skin | 172 | 662 | 1428 | 0.455 | < 0.001 | (0.425, 0.487) | 1(d) |
| Head & neck | 116 | 252 | 483 | 0.700 | < 0.001 | (0.627, 0.782) | |
| Bladder | 159 | 480 | 991 | 0.471 | < 0.001 | (0.386, 0.575) | |
| Female specific | 134 | 469 | 1141 | 0.524 | < 0.001 | (0.481, 0.572) | |
| Male specific | 175 | 502 | 1333 | 0.462 | < 0.001 | (0.414, 0.515) | |
| Cancer type | |||||||
| Breast | 31 | 62 | 330 |
| 1(e) | ||
| ‘Other’ | 149 | 483 | 1220 | 0.498 | < 0.001 | (0.474, 0.523) | |
| Variable | Model | ||||
|---|---|---|---|---|---|
| 1 (Full) | 2 | 3 | 4 (Final) | ||
| Gender | Coefficient ( | 0.030 (0.552) | Omitted | Omitted | Omitted |
| Cancer type group (1) | Coefficient ( | −0.812 (< 0.001) | −0.798 (< 0.001) | −0.801 (< 0.001) | −0.787 (< 0.001) |
| Cancer type group (2) | Coefficient ( | −0.376 (< 0.001) | −0.358 (< 0.001) | −0.357 (< 0.001) | −0.357 (< 0.001) |
| Cancer type group (3) | Coefficient ( | −0.781 (< 0.001) | −0.762 (< 0.001) | −0.765 (< 0.001) | −0.753 (< 0.001) |
| Cancer type group (4) | Coefficient ( | −0.652 (< 0.001) | −0.652 (< 0.001) | −0.650 (< 0.001) | −0.646 (< 0.001) |
| Cancer type group (5) | Coefficient ( | −0.798 (< 0.001) | −0.768 (< 0.001) | −0.782 (< 0.001) | −0.782 (< 0.001) |
| WIMD2014 quintile | Coefficient ( | 0.010 (0.258) | 0.009 (0.264) | Omitted | Omitted |
| Age (years) | Coefficient ( | 0.001 (0.189) | 0.001 (0.190) | 0.001 (0.166) | Omitted |
- —NHS 10.13039/100030827
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsLymphatic System and Diseases · Cancer survivorship and care · Breast Cancer Treatment Studies
Summary
- This study had a large sample size and used data available within the SAIL Databank, which covers 84% of primary care data of the Welsh population, and 100% of secondary care data.
- A large number of individuals experience lymphoedema following a cancer diagnosis and that with some types of cancer, breast cancer in particular, this can develop within weeks of the initial diagnosis.
- Early diagnosis would also allow more targeted treatment plans and care to be put in place quicker, leading to a more cost‐effective treatment of the condition.
- Lymphoedema can develop with all cancer types and that there is a wide variation in the time to diagnosis. However, patients need to be most vigilant within the first 18‐months post diagnoses.
- All cancer healthcare professionals should have a general awareness of lymphoedema, tools for screening and knowledge surrounding the referral process enabling prompt treatment.
Background
1
Lymphoedema is defined as a long‐term condition that causes swelling in the body's tissues. It can affect any part of the body but usually develops in the arms or legs (https://www.nhs.uk/conditions/Lymphoedema/). It can also involve the trunk, head, or perineum [1, 2]. It develops when the lymphatic system (the system to remove excess interstitial fluid and fight infection in the body, whilst also providing a nutritional function) is not working properly, and the demand for lymphatic drainage exceeds the capacity of the lymphatic circulation [3]. Lymphoedema is a progressive condition with excess tissue oedema being the predominant feature during the early stages. As the condition advances, the limb becomes firm, tight, non‐pitting, and fibrotic, with deepened natural skin folds [4]. It causes a range of symptoms, including an aching, heavy feeling and difficulty with movement. There is an increased risk of repeated skin infections such as cellulitis, which can lead to skin changes such as wart‐like growths developing on the skin and fluid leaking through the skin (lymphorroea). It significantly impacts the lives of people who experience it and has been shown to have a detrimental effect on health‐related quality of life [1, 2, 5]. Lymphoedema can have a major physical, psychological, and social impact on patients [3, 6, 7].
Lymphoedema can be classified as primary or secondary. Secondary lymphoedema is the result of obliteration, removal, or obstruction of the lymph nodes, or from damage or obstruction of the lymphatic vessels [8]. One of the major causes of secondary lymphoedema is following treatment for cancer, in particular when the lymph nodes are removed following surgery [9]. Figures from the UK (https://www.nhs.uk/conditions/Lymphoedema/) suggest that there are around 400,000 people affected by lymphoedema (https://www.lymphoedema.org/index.php/information‐and‐support/what‐is‐lymphoedema). In Wales, the prevalence in 2024 was demonstrated as 7.2 per 1000 people, equating to 25,000 people in Wales living with lymphoedema with an incidence of 3 per 1000 [10]. As cancer incidence is increasing, this figure will increase further. The prevalence of cancer‐related lymphoedema has been suggested to be upwards of 25% [11, 12, 13].
Although survival rates for cancers are increasing, treatment‐associated morbidity is common and can persist well beyond the treatment period [14]. Paradoxically, it is the improvement in survival and the increasingly successful outcomes of oncological therapy that have led to an increase in the incidence of lymphoedema and its associated burden [1]. It has been suggested that lymphoedema develops in approximately one‐fifth of cancer survivors, with incidence increasing over time [14]. From an economic perspective, the treatment of chronic lymphoedema is becoming more common, with the therapeutic regime often being complex, time‐consuming, and requiring constant and steady treatment and self‐management regimes [2, 15, 16]. In addition, lymphoedema is associated with a high rate of complications such as chronic wounds and cellulitis [9, 17, 18]. For this reason, lymphoedema leads to high costs and disease burden. A 2017 European study found that the average cost per patient was almost €6000 [17] and this has almost certainly increased further since that time.
Given the increasing number of patients being diagnosed and successfully treated for cancer, and the growing number of patients experiencing lymphoedema, there is a need to understand more about this complex disease to promote early intervention.
There is a developing body of research aimed at identifying, preventing, and treating lymphoedema, including exploration of potential risk factors that may contribute to the development of lymphoedema. Most of this work has focussed on patients undergoing surgical treatment for breast cancer [9, 14, 19, 20]. A 2019 review estimated that 1 in 6 women treated for breast cancer will develop lymphoedema within months to years after diagnosis and treatment [21] and a 2020 systematic review [12] similarly identified arm‐related lymphoedema as the most reported symptom after breast cancer treatment. A 2008 Australian population‐based study reported that oedema presented 6 to 18 months after surgery for invasive breast cancer in 33% of women, with 40% identified as having lymphoedema [22]. A recent systematic review estimates that prevalence rates could be as high as 74% [23].
Other cancer types (gynaecological, urological, melanoma etc.) also carry a risk of lymphoedema development depending on the extent of the tumour and cancer treatment intensity. A recent study identified that 34% of endometrial, 35% of cervical, and 43% of vulvar patients experienced lymphoedema [24]. Two studies identified that greater than 50% and greater than 75% of patients developed lymphoedema secondary to head or neck cancer treatment [25, 26]. A recent systematic review identified much higher rates with wide variation in the reported incidence of other cancer‐related lymphoedema, reporting 8%–45% for gynaecological and urological cancer, 7%–90% in head and neck cancer, and 2%–29% in melanoma cancers [23]. The body of literature, particularly in relation to other cancer types, is still limited.
This study aimed to describe the number of cases in Wales diagnosed with breast, skin, head and neck, bladder, female gynaecological, and male genitalia/prostate cancers; the time duration to lymphoedema development following a cancer diagnosis; and whether demographic information had any impact on the time to lymphoedema development.
Method
2
We utilised anonymised routinely collected individual‐level, population‐scale electronic health record (EHR) data sources available within the Secure Anonymised Information Linkage (SAIL) Databank to undertake this study (https://saildatabank.com) [27, 28, 29]. The SAIL Databank is the national Trusted Research Environment (TRE) for Wales, a privacy‐protecting TRE containing data including primary care events from 84% of general practices around Wales (population coverage ~3.2 million people) and secondary care in‐patient hospital episodes from 100% of National Health Service (NHS) Wales. All data are anonymised within SAIL, but individual‐level linkage is possible through an encrypted anonymised linking field which allows associations to be made between data sources and longitudinal patient pathways for analyses. We designed and reported our study in accordance with the Reporting of studies Conducted using Observational Routinely collected health Data (RECORD) statement [30].
For our study, we had data coverage from 1st January 2010 to 31st December 2020. Table 1 gives details of the specific data sources approved for use by our study within the SAIL Databank and that were used for the cohort selection and outcome identification.
Two patient cohorts (a cancer cohort of pre‐specified cancers and a lymphoedema cohort) were developed and subsequently merged to undertake analysis.
Cancer Cohort
2.1
We developed a cancer cohort by identifying all patients with a diagnosis of any of six pre‐specified cancer types (breast, skin, head and neck, bladder, female gynaecological, and male genitalia/prostate) registered within either the Welsh Cancer Intelligence and Surveillance Unit (WCSU) or Patient Episode Database for Wales (PEDW) data sources between 1st January 2010 and 31st December 2020. At the time of our study, WCSU updates were suspended due to the COVID‐19 pandemic (mid 2020), so we identified any new cancer cases after this date using PEDW data only. We identified the date of cancer diagnosis as the first admission recorded for each respective cancer. International Classification of Diseases version 10 (ICD‐10) codes were used to identify each cancer type of interest (breast, skin, head and neck, bladder, female gynaecological, and male genitalia/prostate) in PEDW and WCSU. Details of the specific codes used are documented in Table S1.
Lymphoedema Cohort
2.2
We developed a lymphoedema cohort by identifying patients with a diagnosis of lymphoedema in either PEDW or WLGP data sources. We used the earliest date recorded in either PEDW or WLGP as the date of diagnosis for lymphoedema. We used ICD‐10 and Read codes version 2 to identify lymphoedema in WLGP and PEDW. Details of the specific codes used are documented in Table S2.
Combined Cohort
2.3
Following the development of the two patient cohorts (cancer and lymphoedema), we undertook data matching using their Anonymised Linking Field (ALF) [29] to create a single cohort of cases with both cancer and lymphoedema. We also collected data from the WDSD to gather basic demographic information (age, sex). We used the Welsh Index of Multiple Deprivation (WIMD; https://www.gov.wales/welsh‐index‐multiple‐deprivation) version 2014 quintile to measure area‐level socio‐economic status and deprivation assigned based on each individual's Lower‐layer Super Output Area (LSOA) of residence version 2011.
Statistical Methods
2.4
We used SPSS (Version 25) to analyse an integrated study dataset, created using SQL via Eclipse from data accessed within the SAIL Databank using IBM DB2.
We defined our primary variable as the time (in days) between cancer and lymphoedema diagnoses. We allocated patients to age bands (using age at cancer diagnosis) and grouped cancers into 6 broad classes (‘types’), with a further simplification into ‘breast’ and ‘other’.
We obtained summaries of the primary variable across a range of factors—gender (female/male); age band; cancer location; and WIMD quintile—and supplemented these with Kaplan–Meier survival curves. We then used Cox regression models to assess the relationship between our primary variable and this set of explanatory factors, both individually and collectively.
Results
3
Cancer and Lymphoedema Cohorts
3.1
We identified 107,649 people with one of the pre‐defined cancers. The mean age of the cancer diagnosis cohort was 63.4 years, with a range from 11 to 100 years.
We identified 26,843 patients with a lymphoedema diagnosis. The mean age of the lymphoedema diagnosis cohort was 64.8 years, with a range from 11 to 102 years.
Combined Cohort
3.2
We identified 9131 cases of both a cancer diagnosis and a lymphoedema diagnosis, with 7538 cases where the lymphoedema developed after the cancer diagnosis. These 7538 cases related to 7279 unique people, who form our combined cohort. Table 2 summarises their demographic characteristics. Most cases were female. The most common age categories were 46–60 and 61–75 years, and breast cancer was the most common cancer identified.
Distributions of Times Between Cancer and Lymphoedema Diagnoses
3.3
Across the combined cohort, the mean time between cancer and lymphoedema diagnoses was 483.3 (days), with considerable variation around this value; the standard deviation of 701.8 (days) indicates significant skewness. Table 3, therefore, summarises the distribution of this variable across each factor using the 25th, 50th and 75th percentiles—that is, the median and lower and upper quartile—with a formal comparison via hazard ratios from Cox regression models, supported by survival curves in Figure 1a–e.
Survival curves for the time between diagnosis and our pre‐defined factors. (a) Survival curves for time between diagnoses, by gender. (b) Survival curves for the time between diagnoses by age group. (c) Survival curves for time between diagnoses by WIMD quintile. (d) Survival curves for the time between diagnoses, by cancer type. (e) Survival curves for time between diagnoses for ‘breast’ and ‘non‐breast’ cancers.
Comparison of time to lymphoedema diagnosis identified that ‘other’ cancers had much longer times to diagnosis when compared with breast cancer. Cases with breast cancer developed lymphoedema a median of 2 months after their cancer diagnosis (upper and lower quartile, 12 to 12 months). Cases with ‘other’ cancers developed lymphoedema a median of 16 months (upper and lower quartile, 5 to 39 months).
Full Cox Regression Models
3.4
Figure 1 implies that all factors are potentially useful in explaining observed variation in time between diagnoses. We therefore fitted a sequence of Cox regression models, starting with a full model including all factors, and then removing any non‐significant factors until only statistically significant factors remained.
This process is summarised in Table 4, which shows that cancer type is the single most useful explanatory factor. The final model in Table 4 (Model 4) is as shown in Table 3, with hazard ratios obtained by exponentiating the coefficients.
Conclusion
4
This is the first attempt to describe the numbers of cases of lymphoedema in Wales following a cancer diagnosis using the SAIL Databank. Across our 10‐year period, 7538 cancer types were identified for 7279 distinct individuals. The mean age at cancer diagnosis was 63.4 years, with the mean age at lymphoedema diagnosis of 64.8 years. This means, on average, that lymphoedema tends to develop around 12 months after diagnosis. Most cases were female. The most common age categories were 46–60 and 61–75 years, and breast cancer was the most common cancer identified. There was considerable variation between the mean time to diagnosis of lymphoedema in our combined cohort of 483.3 days, with a standard deviation of 701.8 days. Initial analysis of the pre‐defined factors (sex, age, deprivation, cancer type) indicated that they could all be useful in explaining the time to lymphoedema diagnosis. However, when further analysis was undertaken using Cox regression models, only cancer type was the single most explanatory factor. Comparison of time to lymphoedema diagnosis identified that ‘other’ cancers had much longer times to diagnosis when compared with breast cancer.
Our findings mirror those of a 2019 review which identified that 1 in 6 women treated for breast cancer will develop lymphoedema within months to years after diagnosis and treatment [21]. The high number of cases of lymphoedema following a breast cancer diagnosis could be due to the fact that there is an increasing incidence of breast cancer, with more patients undergoing breast surgery [31]. In addition, there is likely to be increased vigilance and standard referral pathways for breast cancer patients to lymphoedema services which may not exist or be formalised for ‘other’ cancer types. Chest wall radiotherapy is also commonly performed in breast cancer patients, and both surgery and radiotherapy can cause lymphedema, with significant impairment of the normal lymphatic drainage producing an abnormal collection of protein‐rich fluid within the upper limb [31]. Similarly, the earlier median onset time of lymphoedema in breast cancer cases of 2 months aligns with previous research indicating that lymphoedema can develop within days postoperatively, with an increased prevalence over time [32].
Other studies have found estimates of varying incidence of lymphoedema ranging from 2% to 83% in various cancers [22, 23, 33, 34, 35]. Most of these have indicated increased incidence of breast cancer when compared with other cancer types [23, 33, 36]. Many risk factors for the development of lymphoedema have been identified depending on the site of the cancer and include a diagnosis of breast cancer, advanced cancer stage, types of surgery, radiotherapy, and being overweight to name but a few [37].
This study had a large sample size and used data available within the SAIL Databank, which covers 84% of primary care data of the Welsh population and 100% of secondary care data. Extrapolations made from these data are likely to represent a realistic estimate of the problem. Although clinical coding may be an issue, we have tried to improve data quality using pre‐specified codes for our cancers of interest and lymphoedema codes. We only explored a limited number of factors and specific cancer types in this study, so more work is needed to determine whether other factors may be significant predictors of time to lymphoedema development in addition to cancer type.
The results illustrate that a large number of individuals experience lymphoedema following a cancer diagnosis and that, with some types of cancer—breast cancer in particular—this can develop within weeks of the initial diagnosis. Lymphoedema is an expensive problem for the NHS [9, 17, 18, 38], can result in substantial discomfort, and have a detrimental impact on health‐related quality of life [1, 2, 5]. More work is needed to define risk factors that could be used to inform treatment strategies for patients with cancer. Initiatives to identify early signs/risks of lymphoedema after cancer diagnosis would greatly improve the health‐related quality of life of such patients. Early diagnosis would also allow more targeted treatment plans and care to be put in place quicker, leading to a more cost‐effective treatment of the condition.
Ethics Statement
We received approval for the use of anonymised data within the SAIL Databank from the SAIL independent Information Governance Review Panel (IGRP) under project 0969. The IGRP provides independent guidance and advice on information governance policies, procedures and processes for SAIL Databank (https://saildatabank.com/governance/approvals‐public‐engagement/information‐governance/). Data held within the SAIL Databank are made available to researchers in an anonymised format and are therefore not subject to data protection legislation. SAIL follows all relevant legislative and regulatory frameworks in using population data for research.
Conflicts of Interest
The authors declare no conflicts of interest.
Supporting information
Data S1. Supporting Information.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1A. Szuba and S. G. Rockson , “Lymphedema: Classification, Diagnosis and Therapy,” Vascular Medicine 3, no. 2 (1998): 145–156, 10.1177/1358836 X 9800300209.9796078 · doi ↗ · pubmed ↗
- 2C. J. Moffatt , P. J. Franks , D. C. Doherty , et al., “Lymphoedema: An Underestimated Health Problem,” Quarterly Journal of Medicine 96 (2003): 731–738.10.1093/qjmed/hcg 12614500859 · doi ↗ · pubmed ↗
- 3C. Rymal , “Lymphedema Management in Patients With Lymphoma,” Nursing Clinics of North America 36, no. 4 (2001): 709–734.11726349 · pubmed ↗
- 4J. R. Casley‐Smith , Modern Treatment for Lymphoedema, 5th ed. (Lymphoedema Association of Australia, 1997).
- 5M. Gabe‐Walters and M. Thomas , “Development of the Lymphoedema Patient Reported Outcome Measure (LYMPROM),” British Journal of Nursing 30, no. 10 (2021): 592–598, 10.12968/bjon.2021.30.10.592.34037455 · doi ↗ · pubmed ↗
- 6R. Thomas‐Mac Lean , B. Miedema , and S. R. Tatemichi , “Breast Cancer‐Related Lymphedema: Women's Experiences With an Underestimated Condition,” Canadian Family Physician 51 (2005): 246–247.16926934 PMC 1472970 · pubmed ↗
- 7S. D. Passik and M. V. Mc Donald , “Psychosocial Aspects of Upper Extremity Lymphedema in Women Treated for Breast Carcinoma,” Cancer 83, no. 12 Suppl American (1998): 2817–2820, 10.1002/(sici)1097-0142(19981215)83:12b+<2817::aid-cncr 32>3.0.co;2–2.9874404 · doi ↗ · pubmed ↗
- 8P. S. Mortimer , “Managing Lymphoedema,” Clinical and Experimental Dermatology 20, no. 2 (1995): 98–106.8565266 10.1111/j.1365-2230.1995.tb 02665.x · doi ↗ · pubmed ↗