Cross-Cultural Adaptation and Validation of the Modern Standard Arabic Versions of the Berlin Questionnaire and Epworth Sleepiness Scale
Zainab Lahrichi, Imane El Bassity, Zineb Serhier, Samir Diouny, Adil Khoubila, El Mehdi Jouhadi

TL;DR
This study adapted and validated two sleep assessment tools for use in Arabic-speaking populations, showing they are reliable and effective for diagnosing sleep apnea.
Contribution
The study provides the first validated Modern Standard Arabic versions of the Berlin Questionnaire and Epworth Sleepiness Scale for use in Moroccan clinical settings.
Findings
The MSA versions of the BQ and ESS showed strong reliability with Kappa indices of 0.98-1.00 and an ICC of 0.99.
High-risk OSAS identification was significantly associated with obesity and menopause.
Excessive daytime sleepiness was reported by 61.9% of high-risk OSAS participants.
Abstract
Background The Berlin Questionnaire (BQ) and Epworth Sleepiness Scale (ESS) have been validated in various studies across diverse sociocultural contexts. Despite their significant impact, there is a lack of standardized assessment tools for obstructive sleep apnea syndrome (OSAS) in Arabic-speaking populations. This study aimed to adapt the BQ and the ESS to Modern Standard Arabic (MSA) for use in Moroccan clinical settings and assess their psychometric properties. Methodology The BQ and ESS were translated into MSA using a standardized process involving forward and backward translation. The psychometric properties of the Arabic versions of the BQ and ESS were assessed in 125 Moroccan patients recruited from the University Dental Clinic Ibn Rochd in Casablanca at two time points (T1 and T2). Reliability was assessed using Cohen’s kappa index, and internal consistency was measured…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
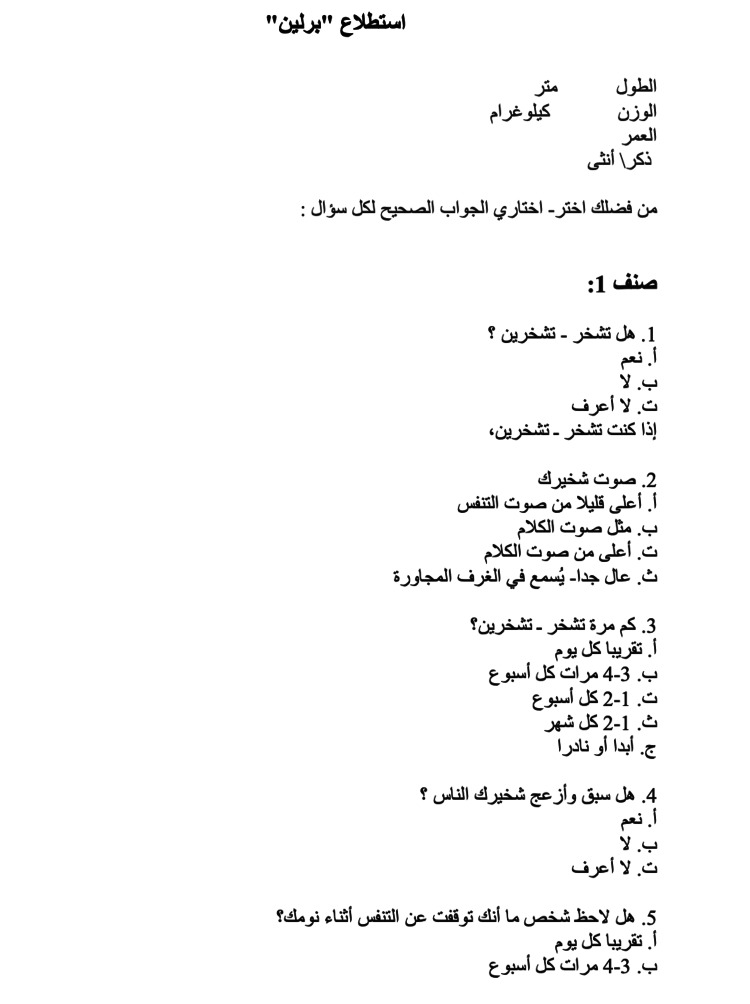 Figure 1
Figure 1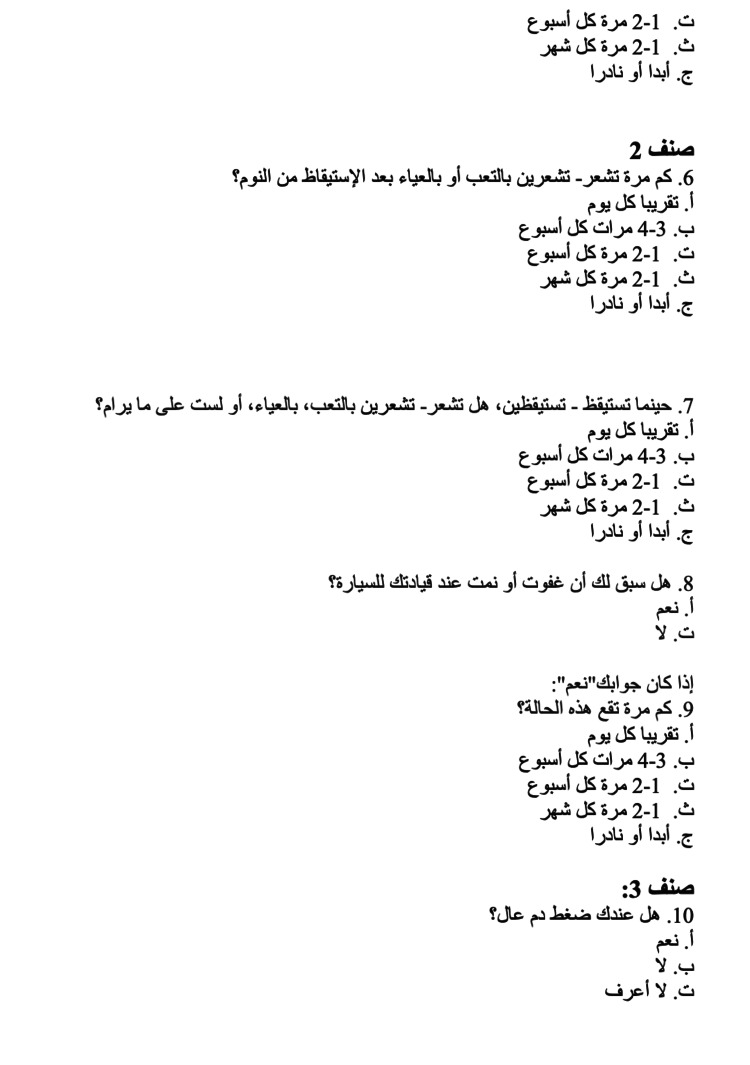 Figure 2
Figure 2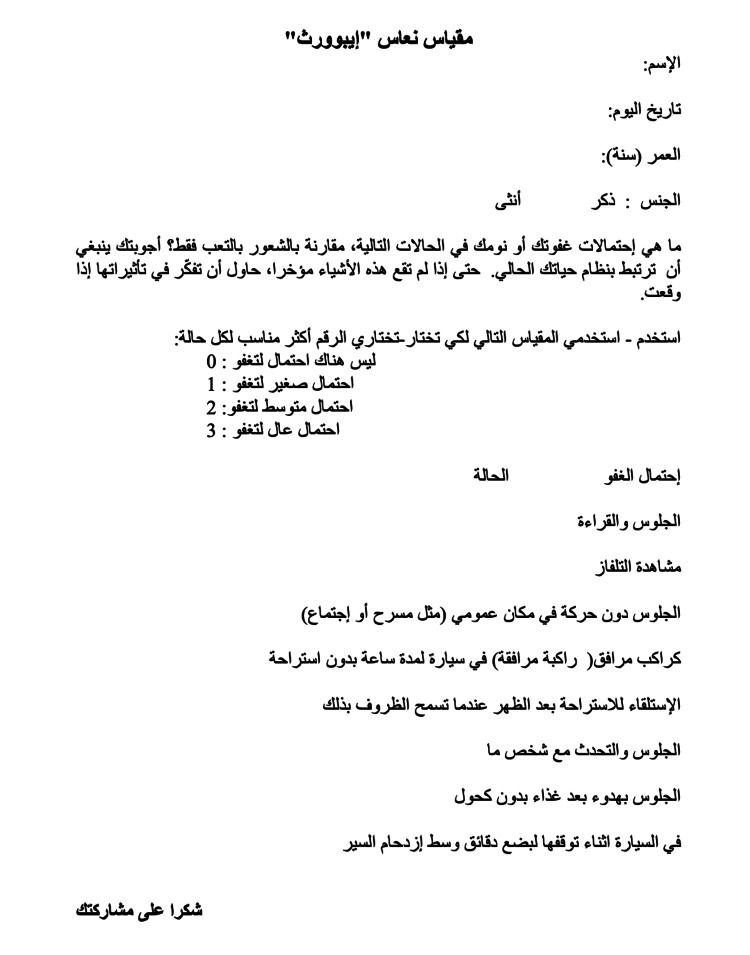 Figure 3
Figure 3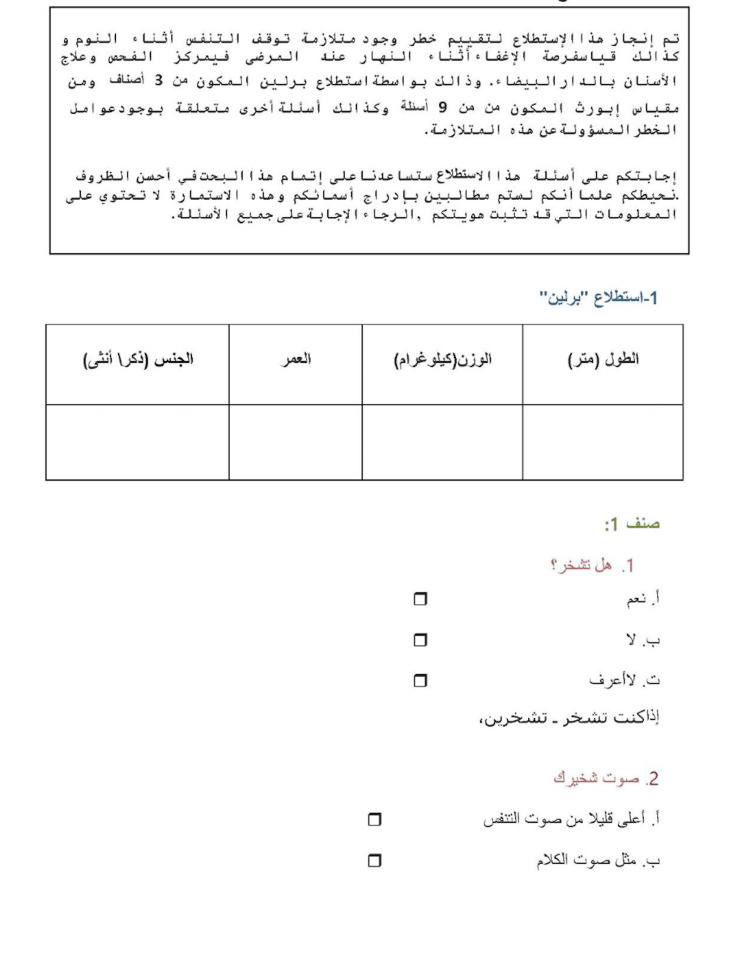 Figure 4
Figure 4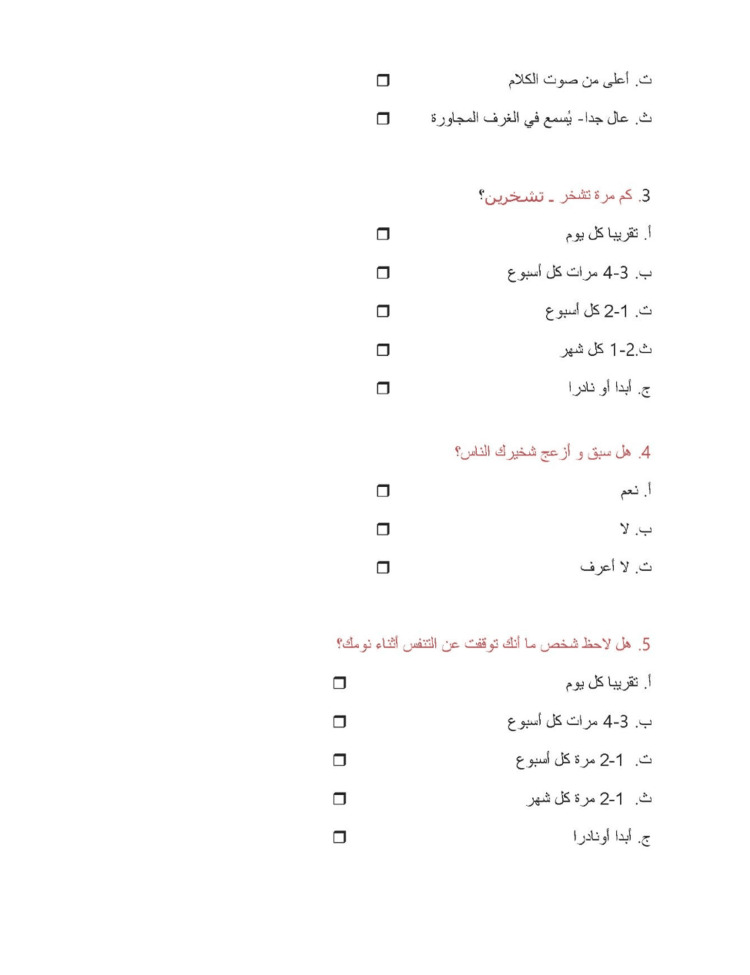 Figure 5
Figure 5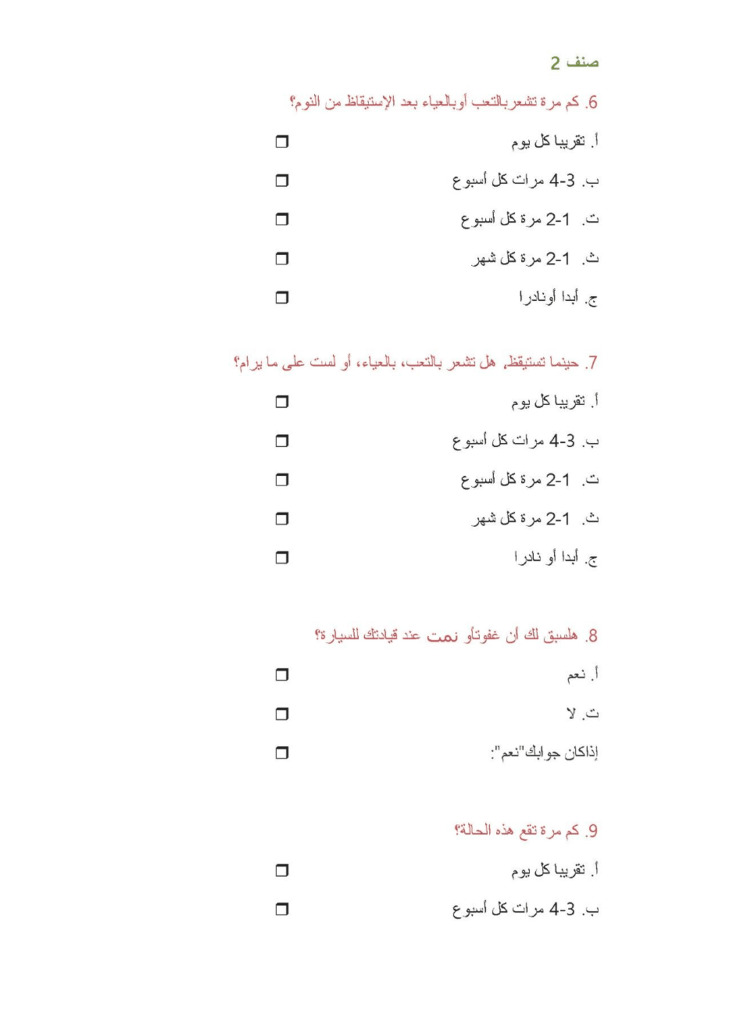 Figure 6
Figure 6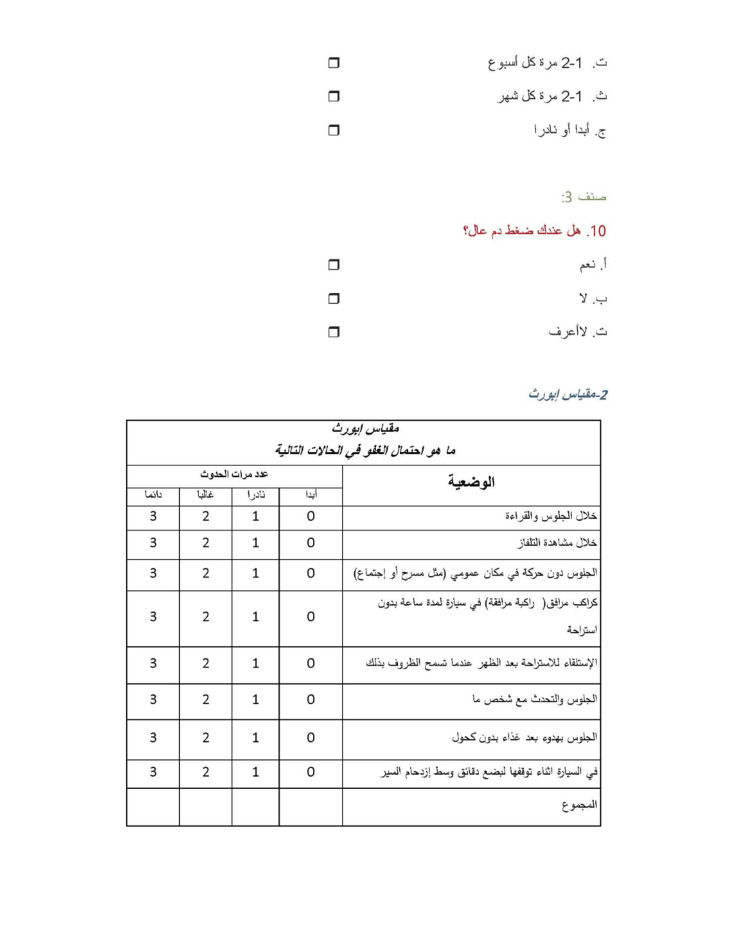 Figure 7
Figure 7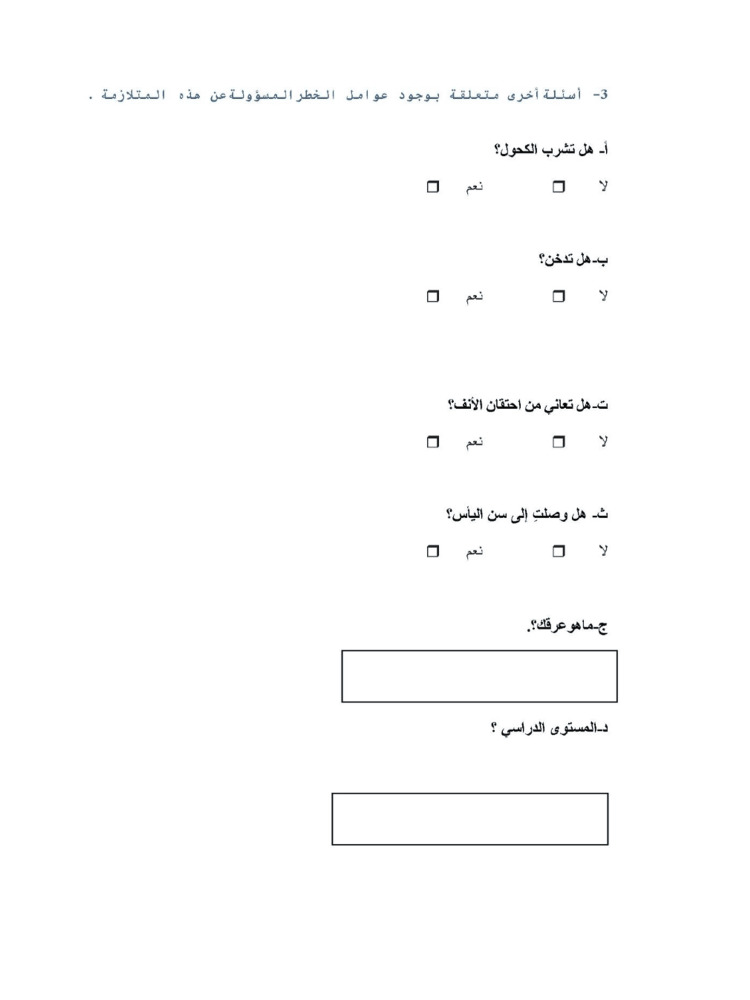 Figure 8
Figure 8| Number | Percentage (%) | ||
| Gender | Female | 72 | 57.6 |
| Male | 53 | 42.4 | |
| Age, mean (SD) = 47.7 (11.2) | <45 years old | 51 | 40.8 |
| ≥45 years old | 74 | 59.2 | |
| BMI, mean (SD) = 26.7 (4.6) | ≤30 | 101 | 80.8 |
| >30 | 24 | 19.2 | |
| Level of education | Primary | 30 | 24.0 |
| Lower secondary | 16 | 12.8 | |
| Upper secondary | 30 | 24.0 | |
| University | 49 | 39.2 | |
| Alcohol | 6 | 4.80 | |
| Smoking | 12 | 9.6 | |
| Nasal obstruction | 34 | 27.2 | |
| Menopause | 26 | 36 | |
| Number (n = 125) | Percentage (%) | 95% CI | |
| OSAS according to the BQ* | 63 | 50.4 | 41.8-59.0 |
| Sleepiness according to the ESS** | 48 | 38.4 | 30.4-47.2 |
| Number of questions | Kappa index/ICC | Cronbach’s alpha index | |
| First category of BQ | 5 | 0.988 | 0.58 |
| Second category of BQ | 4 | 1.00 | 0.67 |
| Third category of BQ | 1 | 1.00 | - |
| ESS | - | 0.99* | 0.74 |
| Berlin positive | Epworth score ≥10 | ||||||
| Number (%) | P-value | χ² | Number (%) | P-value | χ² | ||
| Gender | Female | 37 (51.4) | 0.797 | 0.067 | 29 (40.4) | 0.615 | 0.254 |
| Male | 26 (49.1) | 19 (35.9) | |||||
| Obesity | Obese | 19 (79.2) | 0.002 | 9.833 | 13 (54.2) | 0.077 | 3.122 |
| Not obese | 44 (43.6) | 35 (34.7) | |||||
| Smoking | Smokers | 6 (50.0) | 0.977 | 0.001 | 6 (50.0) | 0.578 | 0.311 |
| Non-smokers | 57 (50.5) | 42 (37.2) | |||||
| Alcohol | Alcoholics | 3 (50.0) | 1 | --* | 45 (37.9) | 0.675 | --* |
| Non-alcoholics | 60 (50.5) | 3 (50.0) | |||||
| Nasal obstruction | Yes | 22 (64.8) | 0.051 | 3.824 | 14 (41.2) | 0.696 | 0.153 |
| No | 41 (45.1) | 34 (37.4) | |||||
| Menopause | Yes | 18 (69.3) | 0.023 | 5.186 | 12 (46.2) | 0.445 | 0.585 |
| No | 19 (41.3) | 17(37.0) | |||||
| Epworth Score ≥10 | P-value | χ² | |||
| Number | Percentage | ||||
| Berlin score | Positive | 39 | 61.9 | <0.001 | 29.67 |
| Negative | 9 | 14.5 | |||
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsObstructive Sleep Apnea Research · Neuroscience of respiration and sleep · Sleep and related disorders
Introduction
Obstructive sleep apnea syndrome (OSAS) is a prevalent sleep disorder that affects nearly one billion individuals worldwide [1]. The disorder is characterized by episodes of a complete (apnea) or partial collapse (hypopnea) of the upper airway, accompanied by a decrease in oxygen saturation or arousal from sleep [2]. OSAS is clinically diagnosed based on polysomnographic data, with the Apnea-Hypopnea Index (AHI) serving as a key indicator. For adults, an AHI of more than five events and fewer than 15 events per hour is considered mild OSAS. Moderate OSAS is defined as 15 to 30 events per hour, while severe OSAS is characterized by an AHI of more than 30 events per hour [2]. OSAS affects both physical and mental health [3] and contributes to a range of conditions, including cardiovascular, neurological, endocrine, metabolic, and ophthalmological disorders. Additionally, it causes fragmented sleep and diminished alertness [4]. These effects collectively impair productivity, safety, and overall quality of life.
Polysomnography and respiratory polygraphy are the gold-standard diagnostic tools for sleep apnea [5]. However, for screening, several measures have been developed, including the Berlin Questionnaire (BQ) (Appendix 1) [6,7] and the Epworth Sleepiness Scale (ESS) (Appendix 2) [8], both of which have been validated in several studies across diverse sociocultural settings.
Despite their widespread use, there is a significant lack of validated Arabic versions of these scales for Arabic-speaking adults. This study aimed to fill that gap. The main objectives of the present study were two-fold: (1) to adapt the BQ and the ESS to Modern Standard Arabic (MSA), and (2) to test the psychometric properties of these adapted versions. The results obtained will have implications for early detection and clinical intervention for individuals with OSAS.
Materials and methods
To address the linguistic and cultural differences between English and Arabic, the BQ and ESS were adapted into MSA following Beaton et al.’s (2000) five-stage process [9]. The first step involved forward translation, where two bilingual translators independently translated the BQ and ESS into MSA. Next, an expert committee reviewed and compared both translations, synthesizing them into a single consensus version. In the back-translation phase, the MSA versions were translated back into English by two independent bilingual translators to ensure consistency with the original versions. The expert committee then carefully reviewed the original and back-translated versions to verify accuracy, cultural relevance, and conceptual equivalence. Finally, the pre-testing phase involved piloting the finalized MSA versions on six patients at the CCTD Ibn Rochd in Casablanca to assess their comprehension of all items and response options. Once the final Arabic versions of the BQ and ESS (Appendices 3 and 4) were produced, the clinical validation phase was initiated through an epidemiological survey conducted over one month, from the beginning to the end of March 2022, at the CCTD Ibn Rochd in Casablanca.
In our study, one interviewer was present to conduct the interviews. This interviewer received comprehensive training to ensure consistency and reliability in data collection. The survey instrument was an anonymous questionnaire consisting of 28 questions aimed at collecting data for the study. It was structured into the following four sections: the first section focused on patient characteristics, the second section screened patients at high and low risk of obstructive sleep apnea (OSA) (BQ), the third section assessed excessive daytime sleepiness (ESS), and the fourth section identified risk factors for OSA.
The BQ consists of 10 questions, along with information on height and weight arranged in the following three categories: (1) snoring and cessation of breathing (five questions), high risk in Category 1 is defined as persistent symptoms in two or more snoring-related questions; (2) excessive daytime sleepiness (four questions), high risk in Category 2 is determined by persistent daytime sleepiness, drowsy driving, or both; and (3) body mass index (BMI) and hypertension (one question), high risk in Category 3 is defined as a history of hypertension or a BMI greater than 30 kg/m². A positive score in two or more categories indicates a high risk for OSA [6].
The ESS consists of eight items representing more or less soporific situations [10,11], namely, describing hypothetical situations such as sitting and reading, watching television, sitting inactive in a public space, as a passenger in a car for an hour without a break, lying down to rest in the afternoon when circumstances permit, sitting and talking to someone, sitting quietly after a lunch without alcohol, and in a car while stopped for a few minutes in traffic [8,12]. Scores range from 0 to 3 (0 = none; 1 = slight; 2 = moderate; 3 = high), resulting in a total score ranging from 0 to 24 points [8,12]. According to Johns [8], a higher score suggests a higher propensity to fall asleep. Conventionally, scores above or equal to 10 may indicate sleep disorders.
The study included 125 patients attending the CCTD Ibn Rochd in Casablanca who agreed to voluntarily answer the questionnaire. Participants had to be over 30 years of age and have attained at least a primary school education. Patients previously diagnosed with OSA, those with facial trauma, and those with bruxism were excluded from the study. Pregnant women, patients with occlusion disorders, and those working at night were also excluded. The study’s objective was explained to the patients before they completed the questionnaire, following which they provided verbal consent. After completion, the BQ and ESS scores were calculated in the patient’s presence. Patients completed the questionnaire once (T1) and a second time (T2), either an hour later for some or a week later for those with a follow-up appointment.
The psychometric properties of the final MSA versions of the BQ and ESS were evaluated based on reliability (internal consistency and test-retest reliability) and validity. Internal consistency was measured using Cronbach’s alpha, with a threshold of 0.6 set to determine scale reliability. Test-retest reliability was assessed using the kappa index and the intraclass correlation coefficient (ICC) to evaluate consistency over time, with all participants completing the questionnaires twice. Statistical analysis was conducted using a Student’s t-test and chi-square test to explore the association between variables and verify construct validity. A p-value ≤0.05 was considered statistically significant. Data were entered into Microsoft Excel version 2021 (Microsoft Corp., Redmond, WA, USA) and analyzed using SPSS version 25.0 (IBM Corp., Armonk, NY, USA).
Results
The study initially included 135 patients, resulting in a response rate of 92.6% (125 completed questionnaires returned). Demographic information of the participants is shown in Table 1. Of the participants, 57.6% were female, the mean age was 47.7 years (SD = 11.2), 39.2% had a university level of education, and 24% had a secondary school level of education. Additionally, 9.6% of patients were smokers, 4.8% consumed alcohol, 27.2% had nasal obstruction, and 35.6% of female participants had gone through menopause.
Table 2 highlights the number and proportion of participants at high risk of OSAS according to the BQ, as well as those experiencing excessive daytime sleepiness based on the ESS. According to the BQ, 50.4% of patients were identified as being at high risk of OSAS, with a 95% confidence interval (CI) of 41.8%-59.0%. Additionally, 38.4% of patients had a positive ESS, with a 95% CI of 30.4%-47.2%.
Table 3 presents data about the reliability of the BQ and the ESS. The kappa index for the first category of the BQ was 0.98, indicating almost perfect agreement. For the second and third categories of the BQ, the kappa index was 1.00, indicating perfect agreement. For the ESS, the ICC was 0.99, indicating almost perfect agreement. The internal consistency of the questionnaire was assessed using Cronbach’s alpha. The values obtained were 0.58 for the first category of the BQ, 0.67 for the second category, and 0.74 for the ESS, indicating acceptable internal reliability.
Discriminant validity was evaluated by analyzing associations between variables, as shown in Table 4. The association between the risk of apnea (positive BQ) and sociodemographic characteristics and risk factors for sleep apnea was statistically significant for obesity (p = 0.002) and menopause (p = 0.023) . Obese people were at higher risk of OSAS (79% vs. 44%), and the frequency of OSAS was higher among menopausal women (69% vs. 41%). The associations between excessive daytime sleepiness according to the ESS and all sociodemographic characteristics and risk factors for sleep apnea were not statistically significant.
Table 5 shows the associations between high risk of OSAS according to the BQ and the excessive daytime sleepiness according to ESS. The p-value was <0.001, indicating that this association is statistically significant. Among the patients at high risk of OSAS according to the BQ, 61.9% reported excessive daytime sleepiness according to the ESS. These results suggest that the questionnaire may be considered reasonably valid and reliable.
Discussion
Given the significant prevalence of OSAS and its well-documented impact on both physical and mental health, systematic screening plays a critical role in the early identification and management of this disorder [13]. Therefore, it is crucial to validate simple tools for early diagnosis. Our work on the translation and cross-cultural adaptation of the BQ and ESS is particularly significant for one main reason, i.e., the relevance of these tools in diagnosing and managing patients with suspected apnea/hypopnea. The choice of MSA as the target language for these translations was driven by the objective of extending the use of these tools across North Africa. This ensures broader comprehension in neighboring countries where the Moroccan dialect may not be widely understood.
The internal consistency of the BQ and the ESS was measured using Cronbach’s alpha, a psychometric statistic that assesses the reliability of questionnaire items, with values closer to 1.0 indicating higher reliability. Generally, an alpha of 0.7 is considered acceptable [14]. Cronbach’s alpha coefficient was 0.58 for the first category of the BQ, 0.67 for the second category, and 0.74 for the ESS, indicating acceptable internal consistency in the latter two categories in both instruments. Although the alpha value of 0.58 is slightly below the commonly accepted threshold of 0.7, it is relatively close and may still be considered acceptable.
These results are satisfactory but somewhat lower than those reported in validation studies by Sharma et al. and Netzer et al. [6,15], who reported Cronbach’s alpha values of 0.92-0.96 and 0.86-0.92, respectively. Similarly, a Thai validation study of the BQ reported an acceptable Cronbach’s alpha of 0.68 [16]. However, another Thai study on the ESS achieved a higher Cronbach’s alpha of 0.87, and the Japanese version of the ESS demonstrated good reliability, with a Cronbach’s alpha of 0.83 [17].
The reproducibility of the BQ, assessed through test-retest reliability for categories 1, 2, and 3, showed almost perfect agreement with kappa values of 0.98, 1.00, and 1.00, respectively. This indicates nearly perfect ICC. The Thai version also showed high reliability with a kappa value of 0.97 [16], consistent with the Korean validation [18], which reported an almost perfect kappa of 0.92.
In our sample, statistically significant associations were observed between risk of apnea (BQ) and obesity (p = 0.002), with 79.2% at high risk of OSAS, and risk of apnea (BQ) and menopause (p = 0.023), with 69.3% at high risk of OSAS. These findings align with existing research indicating that obesity and menopause are predisposing factors for sleep apnea [19]. Conversely, associations between the risk of apnea (BQ) and gender, smoking, alcohol use, and nasal obstruction were not statistically significant, with p-values of 0.797, 0.977, 0.100, and 0.051, respectively. In the present study, among patients with high risk of OSAS according to the BQ, 61.9% also reported excessive daytime sleepiness according to the ESS.
During this survey, we encountered several difficulties. Some patients refused to complete the questionnaire, while others were unwilling to wait to fill it out a second time. The intervals between assessments varied based on participant availability, with some participants reassessed an hour later and others a week after their initial appointment. This variability could potentially impact the test-retest reliability of our measurements. However, previous research comparing two-day and two-week intervals found no significant differences in reliability for health status instruments. Nonetheless, we acknowledge this variability as a limitation and recommend that future studies explore the impact of such time interval differences on measurement reliability. Additionally, some participants returned incomplete questionnaires, leaving certain sections blank. Nevertheless, it is important to emphasize that the majority of respondents showed a genuine interest in the subject, particularly those experiencing symptoms of sleep apnea. However, overall, our study yielded a reliable and valid version of these questionnaires suitable for clinical use.
Conclusions
The BQ and ESS are valuable tools for assessing daytime sleepiness, screening for OSAS, and aiding dentists in managing sleep disorders, particularly sleep apnea syndrome. The Arabic translation of these tools has demonstrated sufficient internal consistency and reproducibility in Moroccan patients, making them reliable resources for screening and prevalence studies of OSAS risk among literate Arabic-speaking populations.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Estimation of the global prevalence and burden of obstructive sleep apnoea: a literature-based analysis Lancet Respir Med Benjafield AV Ayas NT Eastwood PR 687698720193130033410.1016/S 2213-2600(19)30198-5PMC 7007763 · doi ↗ · pubmed ↗
- 2Obstructive sleep apnea-hypopnea syndrome: etiology and diagnosis Avicenna J Med Sankri-Tarbichi AG 38220122321001310.4103/2231-0770.94803 PMC 3507069 · doi ↗ · pubmed ↗
- 3Les Troubles du Sommeil Elsevier Masson Dauvilliers Y 2019 Paris Elsevier Masson 2019
- 4[Retinal vein occlusion and obstructive sleep apnea syndrome]J Fr Ophtalmol Leroux les Jardins G Glacet-Bernard A Lasry S Housset B Coscas G Soubrane G 4204243220091952371410.1016/j.jfo.2009.04.012 · doi ↗ · pubmed ↗
- 5Diagnostic studies in obstructive sleep apnea Otolaryngol Clin North Am Thakkar K Yao M 7858054020071760602310.1016/j.otc.2007.04.005 · doi ↗ · pubmed ↗
- 6Using the Berlin Questionnaire to identify patients at risk for the sleep apnea syndrome Ann Intern Med Netzer NC Stoohs RA Netzer CM Clark K Strohl KP 48549113119991050795610.7326/0003-4819-131-7-199910050-00002 · doi ↗ · pubmed ↗
- 7Validation of the Berlin questionnaire and American Society of Anesthesiologists checklist as screening tools for obstructive sleep apnea in surgical patients Anesthesiology Chung F Yegneswaran B Liao P 82283010820081843111710.1097/ALN.0b 013e 31816 d 91b 5 · doi ↗ · pubmed ↗
- 8A new method for measuring daytime sleepiness: the Epworth sleepiness scale Sleep Johns MW 540545141991179888810.1093/sleep/14.6.540 · doi ↗ · pubmed ↗