Parenteral Nutrition and Anaphylaxis: A Case Report and Literature Review
Otilda M Valderrama V, Stephanie Monteza

TL;DR
A patient had a severe allergic reaction to parenteral nutrition, highlighting the need for careful monitoring and allergen identification.
Contribution
This case report adds to the understanding of rare but severe hypersensitivity reactions to parenteral nutrition.
Findings
A patient with gastric cancer developed anaphylaxis within minutes of receiving parenteral nutrition.
Symptoms resolved after discontinuing PN and administering antihistamines and steroids.
The case emphasizes the importance of allergen identification and vigilance in PN administration.
Abstract
Parenteral nutrition (PN) is a high-risk therapy for patients unable to meet their nutritional needs enterally, carrying risks of hypersensitivity reactions, including anaphylaxis. We present the case of a patient with advanced gastric cancer and a distal subocclusive process that could not tolerate enteral nutrition. PN was initiated, but within five minutes, he developed severe allergic symptoms, which resolved completely after the discontinuation of PN and treatment with antihistamines and steroids. Although hypersensitivity reactions to PN are rare, they can be severe and potentially fatal. Intravenous fat emulsions (IVFEs) and multivitamin solutions are common allergens. This case highlights the need for heightened vigilance during PN administration and the importance of identifying potential allergens. Careful monitoring and individualized care are essential for patients receiving…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
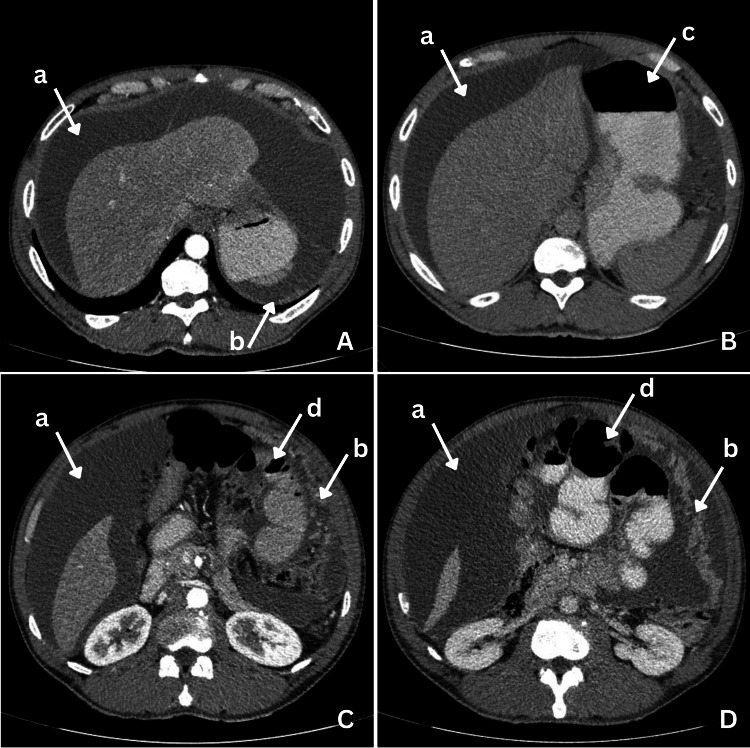 Figure 1
Figure 1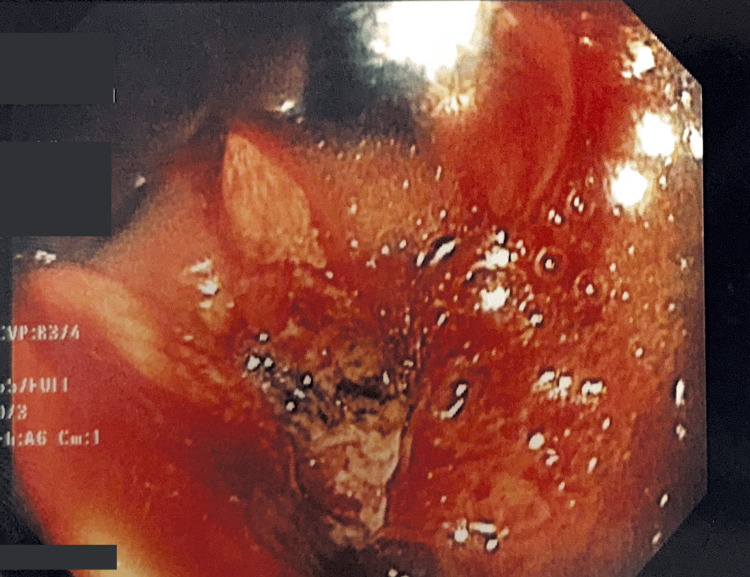 Figure 2
Figure 2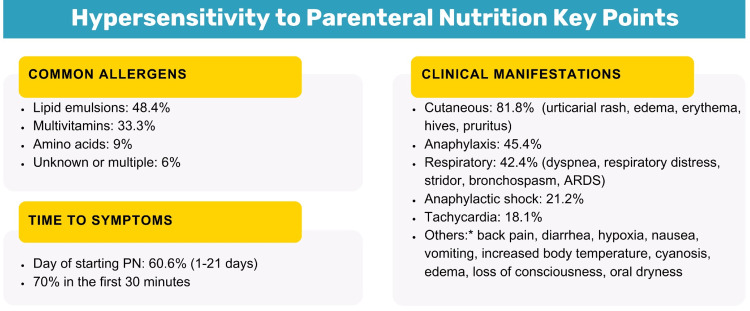 Figure 3
Figure 3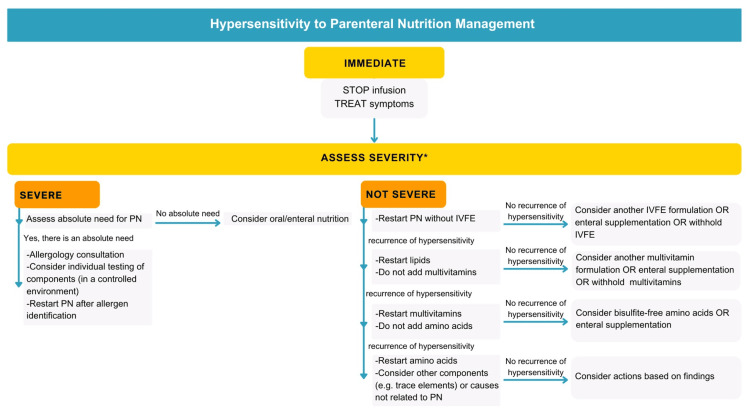 Figure 4
Figure 4| Study/publication year | Age of the patient (years) | Onset of reaction | Suspected allergen | Clinical manifestations | Management |
| Connon et al., 1979 [ | 49 | Within 24 hours | IVFE (Intralipid®) | Diarrhea | Symptomatic treatment |
| Faintuch et al., 1981 [ | 58 | Day 14 | IVFE (Intralipid®) | Diarrhea | IVFE discontinuation |
| Bass et al., 1984 [ | 68 | Within 30 minutes of adding IVFE to PN for the first time | IVFE (Intralipid®) | Anaphylaxis, acute respiratory distress syndrome, cutaneous manifestations, and death | PN discontinuation, supportive care, antihistamines, steroids, and mechanical ventilation |
| Hiyama et al., 1989 [ | 41 | 5 hours | IVFE (Intralipid®) | Anaphylaxis, cutaneous manifestations, and respiratory distress | IVFE discontinuation and supportive care |
| Buchman and Ament, 1991 [ | 36 | Day 2 | IVFE (Intralipid®) | Cutaneous manifestations | IVFE discontinuation and antihistamines |
| Andersen and Nissen, 1993 [ | 48 | Shortly after | IVFE (Lipofundin®) | Respiratory distress/symptoms, hemodynamic instability, and anaphylaxis | Unknown |
| Mounier et al., 1995 [ | 30 | Few minutes | Multivitamin solution | Anaphylaxis, cutaneous manifestations, and respiratory distress | PN discontinuation, antihistamines, and PN reintroduction without multivitamins |
| Weidmann et al., 1997 [ | 45, 50, and 51 | 15 minutes | IVFE (long-chain triglyceride solution) | Cutaneous manifestations, respiratory distress/symptoms, hemodynamic instability, tachycardia, anaphylaxis, and back pain | PN discontinuation, antihistamines, and PN reintroduction with different lipid solutions |
| Crespí Monjo et al., 2005 [ | 55 | Day 1 | Multivitamin solution | Cutaneous manifestations | PN discontinuation, antihistamines, and PN reintroduction without multivitamins |
| Scolapio et al., 2005 [ | 53 | Day 16 | Multivitamin solution | Cutaneous manifestations | Antihistamines and PN continued without multivitamin |
| Cragun et al., 2013 [ | 65 | Immediately | Multivitamin solution and IVFE | Anaphylaxis, hemodynamic instability, tachycardia, hypoxia, and cutaneous manifestations | PN discontinuation, antihistamines, and PN reintroduction without multivitamins and IVFE |
| Sánchez Acera et al., 2014 [ | 43 | Day 13 | Not identified | Angioedema, respiratory distress, and cutaneous manifestations | PN discontinuation, antihistamines, steroids, supportive care, and PN reintroduction with different amino acid solution and without IVFE |
| Honda et al., 2015 [ | 50 | 3 days | Amino acid solution (Aminotripa®) | Cutaneous manifestations | PN discontinuation and change of amino acid solution |
| Çetin et al., 2021 [ | 70 | Within two hours | Trace elements | Cutaneous manifestations | PN discontinuation, antihistamines, steroids, and PN reintroduction without trace elements |
| Present case, 2025 | 50s | 5 minutes | Not identified | Cutaneous manifestation, angioedema, bronchospasm, and anaphylaxis | PN discontinuation, antihistamines, steroids, and transition to enteral feeding |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsFood Allergy and Anaphylaxis Research · Eosinophilic Esophagitis · Pharmaceutical studies and practices
Introduction
Parenteral nutrition (PN) involves the intravenous administration of macro- and micronutrients in a complex mixture that can contain up to 40 components, classified as a high-risk medication due to its complexity and potential risks [1,2]. It is indicated for patients who have contraindications to enteral nutrition, those with compromised gastrointestinal tract integrity or function, and those unable to meet their nutritional requirements enterally despite optimization efforts [1].
The numerous components in PN pose a broad potential for hypersensitivity reactions and make identifying specific allergens challenging. However, the prevalence of these reactions is rare, estimated at approximately 1.5 per one million patients receiving PN in the United States [3]. These hypersensitivity reactions can range from mild, self-limiting symptoms to severe, potentially fatal [4]. Their management requires the early identification of symptoms and prompt management [4,5].
We present the case of a patient who experienced a rare but potentially dangerous hypersensitivity reaction to PN and provide a literature review to highlight the need for heightened awareness and vigilance in PN administration, as well as the importance of individualized patient care strategies.
Case presentation
An adult patient in his mid-50s, without a history of allergies, was admitted to Hospital Santo Tomás in Panama. This is the only highest-level-care hospital operated by the Ministry of Health in this developing country. It is a public adult general hospital with 734 beds, including 30 intensive care unit (ICU) beds, and receives all its funding through state subsidies. As a national referral center, the hospital provides care to a large and diverse patient population, often under resource-constrained conditions.
The patient presented with a two-week history of generalized abdominal pain and distention, unquantified weight loss, nausea, and vomiting. Abdominal computed tomography (Figure 1) revealed ascites, the dilatation of the stomach and small bowel loops (suggestive of a subocclusive process), and images compatible with peritoneal carcinomatosis.
Abdominal CT ScanAbdominal CT scan with oral (A, B, C, and D) and intravenous contrast (A and C). (a) Ascites, (b) images suggestive of carcinomatosis peritoneal, (c) the distension of the gastric chamber and the alteration of the wall, and (d) distended small bowel loopsCT: computed tomography
Upper endoscopy showed an infiltrating, rigid, and non-distensible lesion of irregular surface and friable to biopsy, occupying the lesser curvature, posterior wall, and anterior wall of the body, extending from the cardia to the angular incisure (Figure 2). The histopathological report revealed a poorly differentiated carcinoma.
Upper Endoscopy FindingsA friable, infiltrating, rigid, and non-distensible lesion of irregular surface
The patient had a 13.6% weight loss, with a current weight of 62.2 kg. Due to the distal subocclusive process, PN was requested. Given the high risk of refeeding syndrome, PN was initiated with 1 g/kg/day of protein, 150 g of carbohydrates, and lipids at 0.4 g/kg/day (15 kcal/kg/day).
PN was initiated at 2:17 pm. At 2:22 pm, the patient reported a sensation of warmth at the catheter site, accompanied by generalized pruritus, respiratory difficulty, angioedema involving the lips and periorbital region, and bronchospasm. He exhibited tachycardia (heart rate of 121 beats per minute {bpm}) and tachypnea (respiratory rate of 22 bpm), with a blood pressure of 116/81 mmHg and an oxygen saturation of 95% on room air. Arterial blood gases revealed mild hypoxemia (partial pressure of oxygen {pO₂} of 70 mmHg) and compensated respiratory alkalosis. PN was immediately discontinued, and treatment was initiated with antihistamines and steroid nebulizations, resulting in the complete resolution of symptoms.
PN was identified as the likely cause, given that the patient had not received any medications or food in the previous eight hours, and the reaction occurred immediately after its administration.
Due to the severity of the reaction and the absence of diagnostic tools in our institution, no allergen-specific tests or skin tests were performed. Moreover, the hospital lacks an allergology specialist, precluding the possibility of a formal allergy consultation.
Considering these limitations and the potential risk of recurrence, a re-challenge with PN, even under antihistamine premedication, was deemed unsafe without appropriate allergological evaluation. However, as the subocclusive process was expected to resolve in the short term, the clinical team opted for a conservative approach: delaying further PN while closely monitoring gastrointestinal recovery. This strategy offered a window of opportunity to transition to enteral feeding, minimizing risk while ensuring that nutritional needs would not be neglected. Had enteral access remained unfeasible, alternative PN formulations would have been considered.
Once the subocclusive process improved, oral nutrition with a hyperproteic and hypercaloric formula was initiated. This approach allowed nutritional requirements to be met with low volumes, which the patient tolerated well.
Discussion
The presented case describes a patient with advanced gastric cancer who, due to a distal subocclusive process, could not tolerate enteral nutrition, leading to the initiation of PN. Shortly after, the patient developed a severe hypersensitivity reaction consistent with anaphylaxis. His clinical manifestations align with the literature regarding time to presentation and common clinical manifestations as shown in Figure 3 [3].
*Hypersensitivity to Parenteral Nutrition (PN) Key PointsThe images are original creations by the authors and created using data/information from the specified source [3]They presented along with cutaneous and/or respiratory manifestations (exception: diarrhea)ARDS: acute respiratory distress syndrome
The diagnosis of anaphylaxis in adults is clinical and based on established criteria. According to current guidelines, anaphylaxis is highly likely when one of three diagnostic criteria is met: (a) acute onset of symptoms involving the skin, mucosa, or both, plus either respiratory compromise or hypotension; (b) rapid onset of at least two symptoms such as skin-mucosal involvement, respiratory difficulty, hypotension, or gastrointestinal symptoms after exposure to a likely allergen; or (c) isolated hypotension after exposure to a known allergen [4]. In our case, the patient developed generalized pruritus, angioedema, respiratory difficulty, and bronchospasm within minutes of PN initiation, fulfilling the first and second criteria for anaphylaxis diagnosis.
Anaphylaxis is a severe allergic reaction involving multiple systems and can be potentially life-threatening with a lifetime prevalence of 1.6%-5.1% [4,5]. Its onset is rapid and can cause death due to respiratory and/or circulatory compromise, which may occur without typical allergic manifestations [5]. Severe anaphylaxis is associated with older age, preexisting cardiopulmonary diseases, or pharmacological etiology [5].
In patients receiving PN, hypersensitivity reactions can occur across all age groups, mostly within the first half hour of initiation, though cases of up to 21 days later are reported [3]. The most common clinical manifestations are cutaneous, anaphylactic, and respiratory, with 21.2% of patients developing hemodynamic instability [3].
Intravenous fat emulsions (IVFEs) and multivitamin solutions are the most frequently identified allergens [3]. Reactions to IVFEs are not associated with a specific generation, as most contain egg yolk phospholipids or soybean oil [3,6]. Christian et al. highlight that, although IgE-mediated reactions are not usually directed toward lipid molecules, it is thought that the reaction is due to protein contamination from the mentioned sources [3]. Additionally, they noted fewer reactions to IVFE after 2000, likely due to improved manufacturing [3].
Hypersensitivity reactions can occur to any component of PN, including uncommon ones such as trace elements [3,6,7]. In our case, the specific allergen could not be determined due to the lack of specific diagnostic methods in our institution and the severity of the reaction.
Although most patients with hypersensitivity reactions do not have known allergies to PN components, allergic reactions can still occur [3]. Their potential severity is increased by intravenous administration, necessitating careful monitoring [8]. Furthermore, while hypersensitivity reactions often appear within minutes of PN initiation, cases have been reported where reactions develop after several days of uneventful administration [6,9,10]. This underscores the importance of continuous vigilance, as allergic reactions may not be immediately apparent, requiring ongoing assessment throughout PN therapy.
To better understand our case in the context of previously documented hypersensitivity reactions to PN, we compiled a summary of reported cases in the literature (Table 1). This table highlights the variability in patient demographics, the onset of symptoms, suspected allergens, and clinical manifestations. Similar to our patient, many cases involve rapid-onset anaphylactic reactions occurring within minutes of PN initiation.
Management begins with identifying the allergic reaction, stopping PN, and treating symptoms. Christian et al. propose that further management should be based on reaction severity (Figure 4) [3]. For severe reactions, such as anaphylaxis or cardiorespiratory compromise, it is essential to evaluate the absolute need for PN. If necessary, consulting an allergist for the identification and elimination of the allergic component is needed before restarting PN [3].
*Hypersensitivity to Parenteral Nutrition Management RecommendationsThe images are original creations by the authors and created using data/information from the specified source [3]Severe reaction: anaphylaxis or any cardiorespiratory compromisePN, parenteral nutrition; IVFE, intravenous fat emulsion
For non-severe reactions, resuming PN without IVFE is recommended, as it is the most identified allergen [3]. If no hypersensitivity recurrence occurs, a different IVFE can be considered, or PN can continue without lipids, with possible enteral supplementation. If allergic reactions persist, it is recommended to start a systematic approach of therapeutic trials to diagnose the allergen through a process of exclusion, as Figure 4 shows [3].
For patients with egg or soy allergies, few alternatives exist. A 100% fish oil lipid emulsion is effective for soy-allergic patients, while those allergic to eggs should discontinue IVFE and resume enteral feeding as soon as possible [8].
This approach requires close monitoring to detect and treat hypersensitivity reactions early, and successful cases have been reported utilizing this strategy to manage the patient [6].
A significant limitation in our case was the inability to identify the specific allergen due to the absence of specialized diagnostic tests and the unavailability of an allergology specialist. This limited our capacity to confirm the etiology of the reaction and to implement a tailored prevention strategy and safely reintroduce parenteral nutrition. These limitations are not unique to our setting; they reflect common constraints in public healthcare systems in developing countries.
The decision not to re-challenge the patient with PN was based not only on the severity of the initial reaction and limited diagnostic resources but also on the clinical expectation that the subocclusive process would improve. This cautious approach allowed for a safe transition to oral feeding. Nonetheless, contingency plans for nutritional support were in place should the enteral route remain contraindicated, ensuring that nutritional needs would not be compromised.
Conclusions
Although hypersensitivity reactions to parenteral nutrition are rare, they can be severe and even life-threatening, requiring immediate recognition and management. This case highlights the importance of maintaining a high index of suspicion for allergic reactions in patients receiving parenteral nutrition, even in the absence of a prior allergy history. Given the complexity of parenteral nutrition formulations, careful monitoring during administration is essential to promptly identify adverse events and minimize risks. Additionally, the lack of widely available diagnostic tools in some hospitals to determine specific allergens presents a challenge in clinical practice. Clinicians must adopt an individualized and proactive approach, balancing the benefits of parenteral nutrition with its potential risks, to optimize patient outcomes.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1The ASPEN Nutrition Support Core Curriculum: A Case-Based Approach - the Adult Patient American Society for Parenteral & Enteral The ASPEN Nutrition Support Core Curriculum: A Case-Based Approach - The Adult Patient American Society for Parenteral and Enteral Nutrition Silver Spring, MD American Society for Parenteral and Enteral Nutrition 2017
- 2ISMP list of high-alert medications in acute care settings 7 2024 2024 https://online.ecri.org/hubfs/ISMP/Resources/ISMP_High Alert_Acute Care_List.pdf
- 3Systematic review of hypersensitivity to parenteral nutrition JPEN J Parenter Enteral Nutr Christian VJ Tallar M Walia CL Sieracki R Goday PS 122212294220182976192810.1002/jpen.1169 · doi ↗ · pubmed ↗
- 4Overview of allergy and anaphylaxis Emerg Med Clin North Am Dribin TE Motosue MS Campbell RL 1174020223478208210.1016/j.emc.2021.08.007PMC 8604419 · doi ↗ · pubmed ↗
- 5Anaphylaxis: a 2023 practice parameter update Ann Allergy Asthma Immunol Golden DB Wang J Waserman S 12417613220243810867810.1016/j.anai.2023.09.015 · doi ↗ · pubmed ↗
- 6[Hypersensibility reaction to parenteral nutrition approach; a case report] (Article in Spanish)Nutr Hosp Sanchez Acera E Arenas Villafranca JJ Abilés J Faus Felipe V 6956972920142455901710.3305/nh.2014.29.3.7156 · doi ↗ · pubmed ↗
- 7A case of hypersensitivity developing against trace element solution in total parenteral nutrition, proved by skin prick test Eur J Clin Nutr Çetin GP Türk M Bahçecioğlu SN Yılmazİ 182918317520213374215710.1038/s 41430-021-00892-8 · doi ↗ · pubmed ↗
- 8A mnemonic for pharmacists to ensure optimal monitoring and safety of total parenteral nutrition: I AM FULL Ann Pharmacother Bohl CJ Parks A 6036135120172862273710.1177/1060028017697425 · doi ↗ · pubmed ↗