Contraception in adolescents with mental disorders: adherence and satisfaction in the use of depot medroxyprogesterone acetate
Giani Silvana Schwengber Cezimbra, Edward Araujo Júnior, Cristina Aparecida Falbo Guazzelli

TL;DR
This study examines how well adolescents with mental disorders stick to and are satisfied with a specific contraceptive method.
Contribution
The study provides insights into contraceptive adherence and satisfaction among adolescents with mental disorders, a less-researched population.
Findings
About half of the adolescents continued using DMPA after 12 months.
The most common reasons for discontinuation were irregular bleeding and weight gain.
Satisfaction with DMPA was reported by over half of the participants.
Abstract
To evaluate the continuation rate, satisfaction, and reasons for discontinuation of depot medroxyprogesterone acetate (DMPA) in adolescents treated in a mental health service. Prospective cohort study conducted in a reference unit for the care of adolescents with mental disorders (MDs) and intellectual disabilities (IDs). All patients received a gynecological consultation and an educational group on contraceptive methods. Sociodemographic data on age, education and gynecological data (menarche, coitarche, regularity of menstrual cycles and presence of symptoms) were collected. Follow-up was quarterly for 12 months, during which symptoms, desire to continue, and satisfaction with the use of the quarterly injectable were assessed. Eight hundred and sixty-two sexually active adolescents were supported, 532 adolescents chose to use the quarterly injectable, and 69 of these agreed to…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
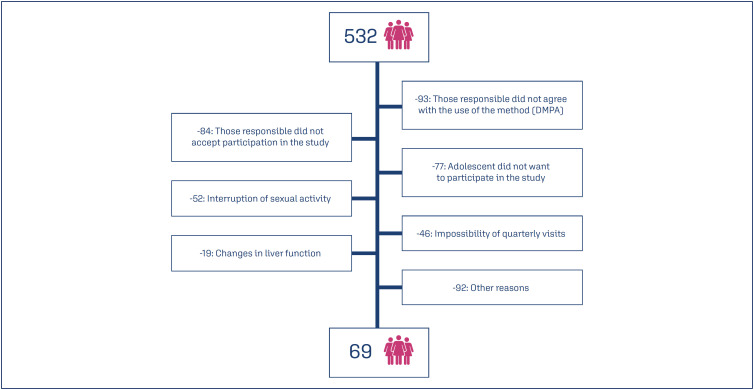 Figure 1
Figure 1| Data | Mean | SD | |
|---|---|---|---|
| Age (years) | 15.4 | 0.91 | |
| Sexual initiation (years) | 14.2 | 1.52 | |
| Menarche (years) | 11.7 | 1.50 | |
|
|
| ||
| ≤ 9 | 42(60.8) | ||
| 9 to 12 | 27(39.2) | ||
| Previous pregnancy | |||
| None | 68(98.5) | ||
| One | 1(1.5) | ||
| Sexual violence | |||
| Yes | 34(49) | ||
| No | 35(51) | ||
| Mental disorder treatment | |||
| Medication | 57(82.6) | ||
| Psychotherapy | 12(17.4) | ||
| n(%) | ||
|---|---|---|
| Blending pattern | ||
| Amenorrhea | 37(54) | |
| Infrequent bleeding | 8(11.6) | |
| Prolonged or frequent bleeding | 22(31.8) | |
| Standard bleed | 2(2.9) | |
| Most frequent complaints | ||
| Weight gain | 35(50.7) | |
| Prolonged or frequent bleeding | 22(31.8) | |
| Mood changes | 11(15.9) | |
| Edema | 8(11.6) | |
| Headache | 5(7.2) | |
| DMPA | n(%) | |
|---|---|---|
| Continuity | ||
| 6 months | 57(82.6) | |
| 9 months | 45(65.2) | |
| > 12 months | 34(49.3) | |
| Dropout | 2(2.9) | |
| Satisfaction | ||
| Satisfied | 36(52.3) | |
| Dissatisfied | 31(44.9) | |
| Dropout | 2(2.9) | |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsMaternal Mental Health During Pregnancy and Postpartum · Adolescent Sexual and Reproductive Health · Reproductive Health and Contraception
Introduction
Adolescents with mental disorders (MDs) and intellectual disabilities (IDs) almost always become pregnant unplanned and are more vulnerable to this risk than adolescents without the condition.^(1)^ Some factors that contribute to this occurrence are lack of knowledge in contraception methods, impulsivity and lack of behavioral control. Difficulties in regular contraceptive use and possible drug interactions are also worth mentioning.^(2-4)^
Reproductive health problems, such as pubertal characteristics, sexuality and menstrual difficulties, may be more common in these adolescents and their families. This period is associated with concerns about menstrual hygiene, risk of abuse, vulnerability and mood changes.^(5)^
Adolescents with MDs often use psychotropic drugs, which can be teratogenic and increase the risk of preterm birth.^(6)^ The most recommended methods for these adolescents are LARCS, especially hormonal intrauterine devices and subcutaneous implants, as well as depot medroxyprogesterone acetate (DMPA), considering the benefit of reducing bleeding in this population.^(5)^ The American College of Obstetricians and Gynecologists (ACOG) recommends the use of DMPA to promote a reduction in blood flow, amenorrhea and perimenstrual symptoms.^(7)^ The use of DMPA has been widely recommended due to its high efficacy, ease of dosing and safety.^(8)^ The choice of DMPA in this study is due to its frequent use in recent decades for contraception in adolescents with mental disorders.^(9)^ There are few studies focusing on reproductive planning and contraception in this population with its specificities.
The aim of this study was to evaluate the continuation rate, satisfaction and reasons for discontinuation of DMPA in adolescents treated in a mental health service.
Methods
This study was a prospective cohort conducted in a reference unit for the care of adolescents (aged 10-19 years) with mild to moderate intensity MDs and their families, the ADOLESCENTRO (Secretaria Estadual de Saúde / Distrito Federal), Brasília, DF, Brazil. All patients who received a gynecological consultation and an educational group on contraceptive methods were invited to participate in the study.
The inclusion criteria were female adolescents in need and desire of contraception, between 10 and 19 years of age, with sexual activity for contraception, and with IDs and other mild to moderate MDs, according to the criteria of the Diagnostic and Statistical Manual of Mental Disorders 5th edition (DSM-5),^(10)^ in treatment. Adolescents with mild cases of IDs were included in the study based on their ability to understand, make choices, and function in general.
Among the exclusion criteria were: presenting any contraindication listed in the package insert of the chosen method; presenting any systemic disease such as liver disease, coagulopathy, cancer or any other factor that contraindicates the use of the chosen method; presenting any gynecological disease such as uterine malformation, vaginal bleeding without etiological diagnosis or any other factor that contraindicates the use of the chosen method; not demonstrating cognitive conditions to understand their contraceptive choice.
At baseline, sociodemographic data on age, education, and gynecological data were collected. Information on medical history and medications used was recorded. The adolescents were followed for 12 months and evaluated every 3 months. At the return visits, clinical assessments were performed, including weight and blood pressure measurements.
This study was approved by the Research Ethics Committee of the Federal University of São Paulo (UNIFESP), number: 2.659.135, on May 16, 2018, and the participants signed the informed consent form.
Results
After attending an educational group, the choice of method was made freely by the adolescent with the help of her guardian and evaluated with the gynecologist according to her needs and indications. A total of 532 adolescents who were interested in using the quarterly injectable method were recruited, of whom 69 agreed to participate in the study. Figure 1 shows the flowchart of the included patients.
Flowchart of the included patients
Sociodemographic and other characteristics are shown in table 1. The mean age was 15.4 years (SD: 0.91). Among the data collected, we observed a high rate (60.8%) of academic delay, represented by the low number of years of study. This data was evaluated according to the study subjects in relation to the age they were at the time of the research and the number of years of education they should have had if they had not failed or dropped out. Another finding that draws attention is the incidence of sexual violence in this group (49%). Notification is always made in the Violence and Accident Surveillance System (Viva/Sinan) and they are taken for evaluation and psychotherapeutic, medication and other treatment, when necessary. The most common MDs were: depression (30.10%), anxiety (22.20%), epilepsy (9.50%), bipolar affective disorder (7.90%), attention deficit hyperactivity disorder (7.90%), attempted suicide (7.90%) and eating disorders (6.3%). IDs were present in 9.5% of cases. Of the 69 participants, 57 (82.6%) were taking psychiatric medication at baseline and 12 (17.4%) were receiving psychotherapy (Table 1).
The most common signs and symptoms associated with DMPA use were menstrual irregularity (43.4%) and weight gain (46.4%). Headache, edema, mood changes and pelvic pain were also reported. Regarding the bleeding pattern, 54% of them experienced amenorrhea after 12 months of use, and the most common complaints were characterized as prolonged or frequent bleeding (31.8%) and infrequent bleeding (11.6%), according to table 2.^(11)^
Among the 32 (46.4%) adolescents who showed weight gain, the range was from 2 to 20 kg, with a mean of 6.5 kg (standard deviation - SD= 4.6 kg and 95% confidence interval - CI = 6.5 ± 1.59). Regarding continuation of the method, after 12 months of follow-up, 49.2% (34) continued to use DMPA, while 47.8% (33) stopped using it and 2.9% (2) discontinued. Satisfaction with the method was 52.3% among users (Table 3).
Discussion
The mean age of our population was 15.4 years (SD: 0.91) and sexual initiation was 14.2 years (SD: 1.52). These data show a delay in the introduction of contraception, considering the risk of pregnancy and that none of them had used any method before entering the study. These adolescents are patients who undergo many medical and psychological consultations, where there is no guidance on contraception. Other studies have linked this fact to the invisibility and inattention of parents and health professionals to the sexual and reproductive needs of these adolescents.^(12)^
DMPA is a well-accepted contraceptive method among adolescents with MDs or IDs due to its ease of dosing and the possible presence of amenorrhea. In addition, there is a non-contraceptive benefit due to its anticonvulsant effects, with the possibility of reducing the frequency and intensity of epileptic seizures.^(5)^ In our study, the most common adverse effects of DMPA use were weight gain (46.4%) and menstrual irregularities (43.4%). Some adolescents reported the presence of headache, edema and mood changes. These symptoms may often be associated with MDs or adverse effects of the medications used and were therefore not evaluated in this specific group.
Weight gain was observed in a large proportion (46.4%) of adolescents using the quarterly injectable, which is in line with several articles on weight gain in users of quarterly injectable DMPA, although there may be many other factors associated with this and many women are able to maintain their weight with dietary measures and physical activity.^(13,14)^ A recent study reported that DMPA users had significantly greater increases in weight (5.1 kg) and body fat (3.4%) over a period of time 3 years compared to women using non-hormonal or oral contraceptives.^(13)^
Appropriate counseling prior to initiation may improve the perception of weight change and reduce the discontinuation rate. On the other hand, it is important to note that factors related to the MD itself and the psychiatric medications used (such as lithium, quetiapine, and risperidone) may be associated with changes in appetite and weight in the adolescents studied.^(13)^ In the case of adolescents with MDs using psychiatric medications that may interfere with weight gain, we consider this an additional reason for the results obtained in this study.
Regarding the change in bleeding pattern, amenorrhea was observed in 37 (54%) of the adolescents. In most cases, amenorrhea was desired and well accepted by the adolescents and their caregivers, which influenced the level of acceptance and continuation. Among other bleeding changes, the main factors that suggests having motivated the early interruption of the method in this study was weight gain in 50.7% of the adolescents and the occurrence of prolonged or frequent bleeding in 31.8% of cases. These data were similar to other studies reporting the occurrence of irregular bleeding in 49% to 90% of patients.^(7)^
A relevant fact observed was the incidence of sexual violence in 49% of the population studied. In Brazil, according to Instituto Brasileiro de Geografia e Estatística (IBGE) data,^(15)^ between 2009 and 2019, one in five adolescents in general (20.1%) between the ages of 13 and 17 reported having experienced some form of sexual violence. An American study of high school students with physical disabilities or health problems found a higher incidence of forced sexual intercourse (19.6%) compared to adolescents without health problems (9.4%).^(16)^ These data indicate the increased vulnerability of this group to this type of violence.
In terms of continuity, of the 69 adolescents who started the study, 49.2% continued to use depot medroxyprogesterone acetate for 1 year or more. The most common reasons for early discontinuation among our adolescents were irregular bleeding (43.4%) and weight gain (46.4%). It is important to note that adolescents with MDs have other difficulties related to their specific mental condition that increase the risk of failure or discontinuation.^(3,14)^ In the literature, we found few studies evaluating the use of this method in adolescents with MDs. In disease-free adolescents participating in the CHOICE project, it was observed that among girls aged 14-19 years who used DMPA for 12 months, the continuation rate was 47.3%.^(17)^ In another 12-month longitudinal cohort study of 1,387 adolescents and young women aged 15-24 years attending public family planning clinics, the 12-month continuation rate with DMPA was 12.1%.^(18)^ Similar to our results, another study found that 45% of adolescents discontinued the method in the first year of use, mainly due to irregular bleeding and weight gain, data consistent with our study.^(19)^
In terms of satisfaction, after 12 months of use, 52.3% of adolescents were satisfied with DMPA use, although 2 of them discontinued use for other reasons. The most common reasons for continued use were safety, ease of dosing, and amenorrhea. In a study of 262 adolescents and young adults with special needs who wanted or needed to suppress menstruation, such as women with cerebral palsy and autism, or with gynecological conditions, it was shown that patients tended to have a high percentage of satisfaction (93.3%) with the use of DMPA due to its menstrual suppression effect.^(20)^
Conclusion
Adolescents with MDS showed a significant rate of continuation and satisfaction with use of the quarterly injectable. Weight gain and irregular bleeding were the most common reasons for discontinuation. DMPA may be a contraceptive option for adolescents with MDs.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Wu J Zhang J Mitra M Parish SL Minama Reddy GK Provision of moderately and highly effective reversible contraception to insured women with intellectual and developmental disabilities Obstet Gynecol 2018132356557410.1097/AOG.000000000000277730095771 PMC 6105436 · doi ↗ · pubmed ↗
- 2Zengin Eroglu M Lus MG Impulsivity, unplanned pregnancies, and contraception among women with bipolar disorder Neuropsychiatr Dis Treat 20201640741410.2147/NDT.S 23888732103960 PMC 7012326 · doi ↗ · pubmed ↗
- 3Schonewille NN van den Eijnden MJ Jonkman NH van Kempen AA van Pampus MG Goedhart FG Experiences with family planning amongst persons with mental health problems: a nationwide patient survey Int J Environ Res Public Health 20232043070307010.3390/ijerph 2004307036833766 PMC 9966993 · doi ↗ · pubmed ↗
- 4Quint EH Menstrual issues in adolescents with physical and developmental disabilities Ann N Y Acad Sci 2008113523023610.1196/annals.1429.02018574229 · doi ↗ · pubmed ↗
- 5DuralÖ TaşİS Akhan SE Management of menstrual and gynecologic concerns in girls with special needs J Clin Res Pediatr Endocrinol 202012 Suppl 1414510.4274/jcrpe.galenos.2019.2019.S 017432041391 PMC 7053443 · doi ↗ · pubmed ↗
- 6Creeley CE Denton LK Use of prescribed psychotropics during pregnancy: a systematic review of pregnancy, neonatal, and childhood outcomes Brain Sci 20199923523510.3390/brainsci 909023531540060 PMC 6770670 · doi ↗ · pubmed ↗
- 7American College of Obstetricians and Gynecologists' Committee on Adolescent Health Care Committee Opinion No. 668: menstrual manipulation for adolescents with physical and developmental disabilities Obstet Gynecol 20161282 e 20e 252745473210.1097/AOG.0000000000001585 · doi ↗ · pubmed ↗
- 8Haider S Darney P Injectable contraception Clin Obstet Gynecol 200750489890610.1097/GRF.0b 013e 318159 c 20a 17982332 · doi ↗ · pubmed ↗