Carotid body tumor associated with complete heart block: A rare case report with long-term follow-up
Ahmad Hoseinzadeh, Hamed Nozari, Ebrahim Zeraatpisheh, Ali Tajaddini, Mohsen Mohebbiniya, Hamid Zaferani Arani

TL;DR
A rare case of carotid body tumor combined with complete heart block is reported, showing successful surgical treatment with multidisciplinary care.
Contribution
This case highlights the rare coexistence of carotid body tumor and congenital complete heart block, emphasizing collaborative surgical management.
Findings
A 47-year-old female had a carotid body tumor confirmed by CT angiography.
Complete tumor resection was achieved with temporary pacemaker support and close monitoring.
Multidisciplinary collaboration improved surgical outcomes in this complex case.
Abstract
Carotid body tumor (CBT) is one of the most common paragangliomas in the head and neck region, accounting for only 0.6 % of tumors in this area. Here, we present a rare case of CBT associated with congenital complete heart block (CHB). We report the case of a 47-year-old female with a history of left neck and ear pain, accompanied by a gradually enlarging neck mass over 2.5 years. Following initial evaluations and multiple differential diagnoses, CT angiography revealed an oval-shaped mass measuring 30 × 50 mm at the left carotid bifurcation, confirming a Shamblin type II CBT. Preoperative assessments demonstrated congenital CHB on electrocardiogram and echocardiography. The patient underwent complete tumor resection with all necessary precautions, including temporary pacemaker placement and careful monitoring. CBTs are considered rare neoplasms, comprising only 0.6 % of head and neck…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
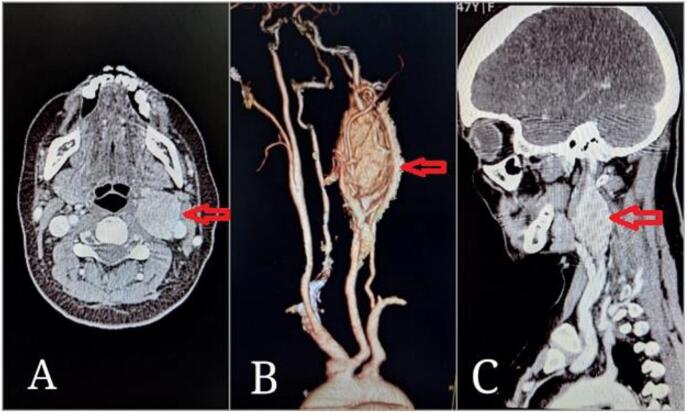 Figure 1
Figure 1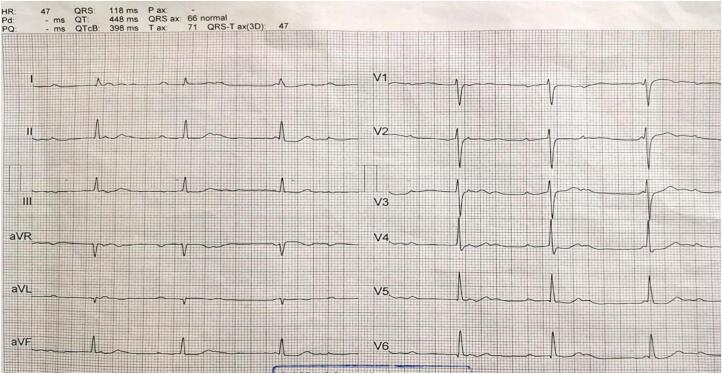 Figure 2
Figure 2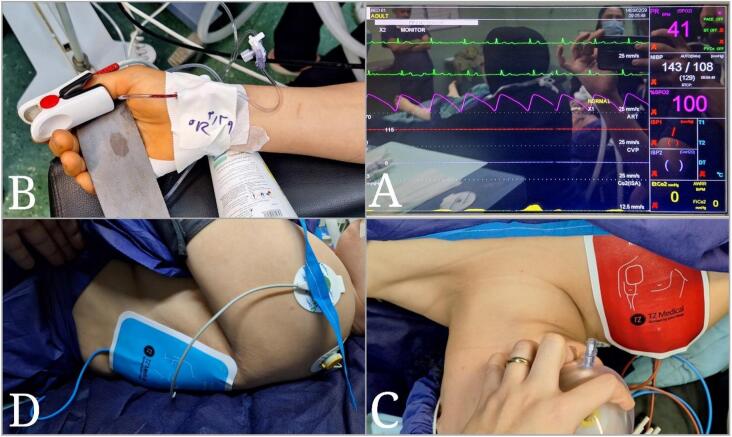 Figure 3
Figure 3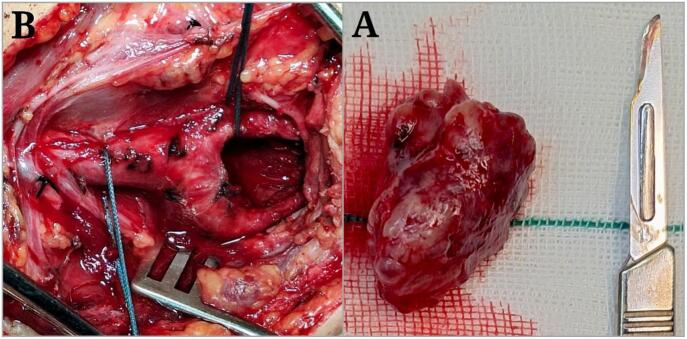 Figure 4
Figure 4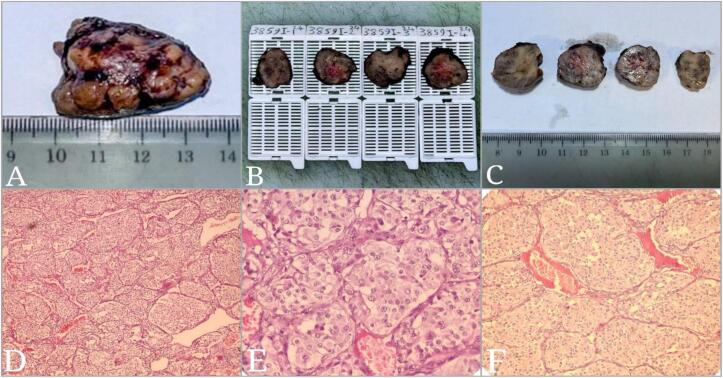 Figure 5
Figure 5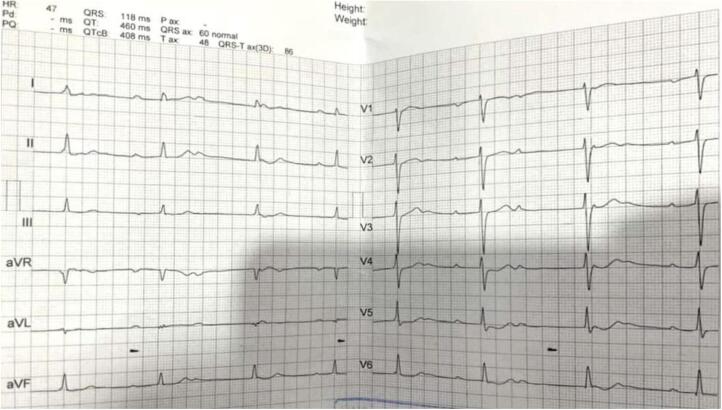 Figure 6
Figure 6Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAdrenal and Paraganglionic Tumors · Neurofibromatosis and Schwannoma Cases · Cardiac tumors and thrombi
Introduction
1
Carotid body tumor (CBT), or glomus tumor, is the most common paraganglioma of the head and neck, originating from neural crest-derived chemoreceptor cells. These rare neoplasms, accounting for only 0.6 % of head and neck tumors, are often associated with chronic hypoxemia, such as in chronic obstructive pulmonary disease or high-altitude living, and exhibit a female predominance, typically presenting between ages 30 and 40 [1,2]. While most CBTs are benign, 2–8 % demonstrate malignant potential, and a subset may secrete catecholamines, complicating their clinical management [3,4]. The development of CBTs is influenced by genetic predisposition, environmental hypoxia, and hormonal factors, particularly estrogen, which has been linked to tumor growth acceleration [5].
Clinically, CBTs present as painless neck masses that, with progressive growth, compress surrounding structures, potentially invading the skull base or cranial nerves. Symptoms may include dysphagia, voice changes, Horner's syndrome, or vagal nerve compression, with diagnosis relying on imaging due to the high bleeding risk associated with biopsy [2,6]. The carotid sinus, a critical baroreceptor, regulates blood pressure and heart rate through parasympathetic pathways. In pathological conditions, CBTs can induce abnormal vagal stimulation, either through direct compression or neural invasion, leading to severe cardiovascular complications such as bradycardia, hypotension, sinus node arrest, or atrioventricular (AV) conduction disturbances [7]. Hence, in line with the SCARE criteria [8], this case highlights the rare coexistence of CBT with congenital CHB, emphasizing the potential for CBTs to exacerbate pre-existing cardiac conduction abnormalities through vagal interference.
Case presentation
2
A 47-year-old female with a history of congenital CHB presented with complaints of left-sided neck pain and left ear pain. Approximately 30 months prior to presentation, the patient had noticed a small mass on the left side of her neck, which had gradually increased in size. The pain was initially localized to the neck region but had intensified over time and extended to the left ear area.
Initially, due to left ear pain, the patient consulted several otolaryngologists and was treated for a preliminary diagnosis of otitis media. However, despite treatments, the pain persisted. Eventually, an otolaryngologist referred the patient for an ultrasound, which revealed a mass in the left side of the neck, leading to a surgical referral. After initial evaluations, a CT angiography was requested, which revealed an oval-shaped mass measuring 30 by 50 mm at the left carotid artery bifurcation, suggestive of a Shamblin type II CBT (Fig. 1).Fig. 1. Pre-operative CT Angiography Images: Axial view (A), 3D reconstruction (B), and Sagittal view (C) (Red arrows).Fig. 1
Preoperative cardiovascular evaluations
2.1
Given the patient's history of congenital CHB, a comprehensive preoperative cardiovascular assessment was conducted. This included a 12‑lead electrocardiogram (ECG), which confirmed the presence of CHB with a stable ventricular escape rhythm (Fig. 2). Transthoracic echocardiography was performed to evaluate cardiac structure and function, revealing normal ventricular systolic function with no evidence of structural abnormalities. Additionally, a cardiology consultation was obtained to assess the patient's fitness for surgery and to optimize perioperative management.Fig. 2. Patient's pre-operative ECG showing complete heart block.Fig. 2
Anesthetic considerations
2.2
Due to the patient's congenital CHB and the potential for hemodynamic instability during surgery, a detailed anesthetic plan was formulated. The patient was classified as American Society of Anesthesiologists (ASA) physical status III. Preoperatively, an external temporary pacemaker was placed to ensure adequate heart rate control, and an arterial catheter was inserted for continuous blood pressure monitoring (Fig. 3). Induction of anesthesia was performed using a combination of etomidate (0.3 mg/kg) and fentanyl (2 μg/kg) to minimize hemodynamic fluctuations. Maintenance was achieved with sevoflurane (1–2 %) and rocuronium (0.6 mg/kg) for muscle relaxation. Hemodynamic parameters, including heart rate, blood pressure, and oxygen saturation, were continuously monitored. Additionally, a central venous catheter was placed to monitor central venous pressure and administer vasoactive medications if needed. The anesthesia team maintained close communication with the surgical team to promptly address any intraoperative hemodynamic changes.Fig. 3. Images of patient preparation before surgery: Vital signs monitor (A), Arterial line (B), External pacemaker (C), External pacemaker (D).Fig. 3
Surgical approach
2.3
The patient underwent surgery on May 19, 2024, after precise localization of the CBT via CT angiography. The surgical approach was chosen based on the Shamblin type II classification, indicating partial encasement of the carotid arteries. Given the tumor's proximity to critical neurovascular structures, including the vagus and hypoglossal nerves, an open surgical approach was deemed the most appropriate to ensure complete resection while minimizing complications.
Following general anesthesia induction, the patient was positioned supine with the neck extended and rotated to the right. An oblique incision was made parallel to the left sternocleidomastoid muscle, extending from the mastoid process to the sternal notch. After skin incision and platysma dissection, the carotid sheath was carefully exposed. The common carotid artery and its bifurcation into the internal and external carotid arteries were identified. The tumor, measuring 30 × 50 mm, was observed at the carotid bifurcation and meticulously dissected from surrounding tissues (Fig. 4).Fig. 4. Images of the carotid body tumor: Resected CBT (A), Carotid artery bifurcation after CBT removal (B).Fig. 4
Specific maneuvers and precautions
2.4
- 1.Temporary vascular clips were applied to the internal and external carotid arteries to control blood flow during tumor dissection. This minimized bleeding and provided a clear surgical field.
- 2.Intraoperative neuromonitoring was used to assess the integrity of the vagus and hypoglossal nerves. Continuous feedback ensured that neural structures were preserved during dissection.
- 3.The tumor was carefully separated from the carotid arteries and surrounding neural structures using a combination of sharp and blunt dissection. Hemostasis was achieved using bipolar cautery and surgical clips to minimize bleeding.
- 4.The external pacemaker was actively monitored throughout the procedure to ensure stable heart rate and rhythm. The anesthesia team was prepared to administer atropine or epinephrine if significant bradycardia or hypotension occurred.
Postoperative management
2.5
After ensuring no active bleeding and reestablishing blood flow, tissues were returned to their original position, and the wound was closed in multiple layers. Appropriate dressing was applied. The surgery was completed without complications and with minimal bleeding in 2 h and 10 min. The patient was then transferred to the vascular ICU for close monitoring.
Postoperatively, the patient was monitored in the ICU for 24 h and later transferred to the general ward after clinical improvement. The external pacemaker was removed on postoperative day 1, as the patient maintained a stable ventricular escape rhythm. The patient was discharged in good general condition on postoperative day 3 without specific complaints.
Follow-up and long-term outcomes
2.6
Histopathological examination confirmed the definitive diagnosis of CBT in the patient (Fig. 5). Follow-up evaluations were conducted at 2 weeks, 1 month, 6 months, and 1 year post-surgery to assess both surgical and cardiac outcomes. At each visit, the patient underwent a 12‑lead ECG to monitor the congenital CHB, which remained unchanged throughout the follow-up period (Fig. 6). Transthoracic echocardiography was repeated at 6 months and one year, showing no deterioration in cardiac function and stable ventricular systolic function.Fig. 5. Pathology report images: Macroscopic views (A, B, C), Microscopic views (D, E, F).Fig. 5. Fig. 6Patient's ECG 6 months after surgery: showing complete heart block.Fig. 6
To evaluate the impact of tumor removal on cardiac function, heart rate variability (HRV) analysis was performed preoperatively and at 6 months post-surgery. Preoperative HRV analysis demonstrated reduced parasympathetic activity, likely due to vagal nerve compression by the tumor. Postoperative HRV analysis showed a significant improvement in parasympathetic tone, suggesting that tumor removal alleviated vagal nerve compression and restored normal autonomic function.
Additionally, the patient reported complete resolution of neck and ear pain following surgery, with no recurrence of symptoms during the follow-up period. Imaging studies, including Doppler ultrasound and CT angiography, were performed at 6 months and 1 year, confirming no evidence of tumor recurrence or vascular complications.
Discussion
3
This case highlights the rare coexistence of a CBT and congenital CHB, which holds significant clinical implications. CBTs, due to their anatomical proximity to the carotid sinus and vagus nerve, can exert mechanical pressure or cause neural invasion, leading to abnormal vagal stimulation. This can result in cardiovascular complications such as bradycardia, hypotension, or disturbances in cardiac conduction, particularly in patients with pre-existing cardiac conditions like CHB [4,6,7]. This case underscores the importance of multidisciplinary collaboration between vascular surgeons, cardiologists, and anesthesiologists in managing such complex cases. The preoperative placement of an external pacemaker and continuous hemodynamic monitoring were critical in mitigating risks during surgery. The successful outcome demonstrates that with meticulous planning, surgical intervention can be safely performed even in patients with significant cardiac comorbidities.
Congenital vs. acquired heart block
3.1
The pathophysiological connection between CBT and congenital CHB lies in the potential for vagal overstimulation [7]. The carotid sinus, a key baroreceptor, regulates heart rate and blood pressure through parasympathetic pathways. The congenital nature of the heart block in this patient was substantiated by the absence of acquired causes, such as infectious-inflammatory conditions or degenerative disorders, as confirmed by serological tests and echocardiography [9]. Also, the patient's stable ventricular escape rhythm and lack of structural abnormalities further support the congenital etiology. Indeed, in this patient, the tumor's location at the carotid bifurcation likely caused intermittent pressure on the vagus nerve, exacerbating the risk of hemodynamic instability. While the tumor did not directly cause the heart block, its presence likely exacerbated symptoms due to vagal nerve compression.
Comparison with previous literature
3.2
This case adds to the limited literature on CBTs associated with cardiac conduction disturbances. For instance, Gad et al. (2014) provides a comprehensive analysis of 56 CBTs managed over 25 years, emphasizing the importance of proper preoperative evaluation and surgical expertise in vascular reconstruction [10]. Similar to the current case, the study highlights the use of the Shamblin classification to guide surgical planning and reports a lower incidence of complications in de novo cases compared to those with prior surgical attempts. However, unlike the current case, which involved a rare coexistence of CBT with congenital CHB, they did not specifically address cardiovascular complications or the management of CBTs in patients with pre-existing cardiac conditions. Both studies underscore the critical role of multidisciplinary collaboration and advanced diagnostic tools in achieving favorable outcomes, with the current case further contributing to the literature by demonstrating the safe management of CBT in a high-risk cardiac patient.
In the another study, Darouassi et al., [11] analyzed 10 cases of CBTs over a 5-year period, emphasizing the importance of early diagnosis and multidisciplinary management. Similar to the current case, the study identified a slow-growing neck mass as the primary clinical presentation and relied on advanced imaging techniques, such as CT angiography, for diagnosis. Also, both studies underscore the critical role of surgical excision as the treatment of choice, with the referenced study also highlighting the use of preoperative embolization and postoperative radiotherapy in select cases. However, management(s) of cardiovascular complications in the patients with CBTs was not addressed [11].
Diagnostic and follow-up considerations
3.3
To exclude multiple lesions and confirm the non-secretory nature of the tumor, additional diagnostic studies were performed. An octreoscan and MRI were conducted, which confirmed the absence of multiple lesions. Plasma and urinary catecholamine levels were within normal limits, ruling out a secretory tumor.
Follow-up recommendations included annual imaging (CT angiography or MRI) for the first 5 years to monitor for tumor recurrence, along with regular cardiology evaluations to assess cardiac function. The patient was also advised to report any new symptoms promptly.
Limitations
3.4
This study has several limitations. The follow-up period of 1 year, while longer than initial reports, remains insufficient to assess long-term cardiovascular outcomes and tumor recurrence. Additionally, the lack of genetic testing to rule out familial paraganglioma syndromes is a notable limitation, as genetic predisposition could influence tumor behavior and recurrence risk. Future studies should include longer follow-up periods and genetic evaluations to provide more comprehensive insights.
Conclusion
4
This case report demonstrates that surgical resection of a CBT can be safely performed in patients with congenital CHB, provided that appropriate precautions are taken. The improvement in parasympathetic tone post-surgery highlights the potential cardiovascular benefits of tumor removal, while the 1-year follow-up data confirm the stability of cardiac function and the absence of tumor recurrence. This case underscores the importance of meticulous surgical planning as well as multidisciplinary collaboration in achieving optimal outcomes for complex cases.
Patient consent
Written informed consent was obtained from the patient for publication and any accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal on request.
Ethical approval
The patient provided written consent for this case report, which is presented in an anonymized format. According to the guidelines at our school (School of Medicine, Shiraz University of Medical Sciences, Shiraz, Iran), single case reports do not require separate ethical approval, as they do not contain identifying information and do not involve experimental treatment.
Guarantor
Dr. Hamid Zaferani Arani
Funding
Not applicable.
Author contribution
Ahmad Hoseinzadeh: Conceptualization, Methodology, Software, writing, editing.
Ali Tajaddini, Hamed Nozari, Mohsen Mohebbiniya: Data curation, Writing- Original draft preparation.
Ebrahim Zeraatpishe: Data curation, Writing- Original draft preparation.
Hamid Zaferani Arani: Patient management, Supervision, Writing, editing
Conflict of interest statement
The authors declare that they have no competing interests.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Kilic Y.Jalalzai I.Sönmez E.Erkut B.Jalalzai M.The surgical treatment of carotid body tumor as well as the prevention and management of complications Cureus 161Jan 7, 202410.7759/cureus.51807 PMC 1084675538322070 · doi ↗ · pubmed ↗
- 2Pellitteri P.K.Rinaldo A.Myssiorek D.Jackson C.G.Bradley P.J.Devaney K.O.Shaha A.R.Netterville J.L.Manni J.J.Ferlito A.Paragangliomas of the head and neck Oral Oncol.406Jul 1, 20045635751506338310.1016/j.oraloncology.2003.09.004 · doi ↗ · pubmed ↗
- 3Metheetrairut C.Chotikavanich C.Keskool P.Suphaphongs N.Carotid body tumor: a 25-year experience Eur. Arch. Otorhinolaryngol.273Aug 2016217121792623324410.1007/s 00405-015-3737-z · doi ↗ · pubmed ↗
- 4Vrionis A.N.Olsen K.R.Images in anesthesiology: carotid sinus reflex from neck mass and opioids Cureus 166Jun 10, 202410.7759/cureus.62048 PMC 1123447938989339 · doi ↗ · pubmed ↗
- 5Toscano M.Cristina S.Alves A.R.Cristina S.F.Carotid sinus syndrome in a patient with head and neck cancer: a case report Cureus 122Feb 19, 202010.7759/cureus.7042 PMC 708325432211274 · doi ↗ · pubmed ↗
- 6Cicogna R.Visioli O.A new reflex cardiovascular syndrome: recurrent vasodepressive syncope caused by lesions or tumors of the parapharyngeal space. Etiopathogenesis, clinical picture, differential diagnosis with carotid sinus syndrome and glossopharyngeal neuralgia-asystole syndrome. Therapy by intracranial resection of the 9th cranial nerve G. Ital. Cardiol.185May 1, 19883613683192043 · pubmed ↗
- 7Sutton R.Carotid sinus syndrome: progress in understanding and management Glob. Cardiol. Sci. Pract.20142 Aug 1, 20141810.5339/gcsp.2014.18PMC 422042725405171 · doi ↗ · pubmed ↗
- 8Sohrabi C.Mathew G.Maria N.Kerwan A.Franchi T.Agha R.A.The SCARE 2023 guideline: updating consensus Surgical C Ase R Eport (SCARE) guidelines Int. J. Surg. Lond. Engl.10952023113610.1097/JS 9.0000000000000373 PMC 1038940137013953 · doi ↗ · pubmed ↗